











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Symptoms of anxiety and depression frequently present comorbidity (eg, Hirschfeld, 2001; Noyes Jr., 2001), are present in psychiatric populations and are quite common in the general population (Kessler, Chiu, Demler, & Walters, 2005), even though they do not characterize a specific disorder. As presented over this study, the occurrence of these symptoms in the general population led researchers to conduct studies in order to verify the relationship of these symptoms with broader aspects of psychological functioning, such as personality traits. In this research, we focused on the Beck Depression Inventory (BDI) as a depression measure, on the Beck Anxiety Inventory (BAI) as an anxiety measure, and on the Dimensional Clinical Personality Inventory (IDCP) as a measure of the pathological continuum of personality. Our scope was to investigate the relationships between symptoms of anxiety and depression with personality traits.
Some studies have found that pathological personality traits are related to various psychiatric symptoms, including anxiety and depression (Anaes & Torgesen, 1990; Del Porto, 1999). Britto and Benetti (2012) found that, patients with sexual dysfunction, who had lower scores for neuroticism, also reported fewer symptoms of anxiety and depression. However, Bartholomeu, Axe, Spigato, Bartholomeu, Cozza, and Montiel (2010), using the BDI and the BAI, together with an instrument composed of 64 adjectives based on the Big Five model, applied to football players, showed a significant and negative correlation between Neuroticism and anxiety symptoms, which does not corroborate data usually reported in the literature. Symptoms of depression, in turn, were not significantly correlated with any personality trait.
There are also studies conducted in Brazil focusing only on the relationship between personality traits and symptoms of anxiety or depression. For instance, the literature review conducted by Junior, Lima and Lopes (2014) on the relationship between personality traits and anxiety symptoms, found several studies that point out positive and significant correlations between the Neuroticism dimension and the symptoms typical of anxiety. Morever, a study by Thomas and Alchieri (2005) investigated which personality characteristics contribute to patient adherence to treatment in hemodialy-sis, also assessing symptoms of depression. To conduct their research, they used Millon's Personality Inventory (MPI) and the BDI, and concluded that all subjects who presented high scores in MPI factors also had high scores in the BDI (BDI>17).
Likewise, in the international scenario there are also studies investigating the relations between personality and symptoms of depression and anxiety. Among these studies, the research conducted by Sanja, Elizabeta, and Klementina (2013) stands out. They investigated the relationship between personality and levels of depression (BDI) and anxiety (BAI) in a group of 288 drug abusers, and observed that the subjects who had higher scores in the EPQ relating to Psychoticism, Neuroticism, Criminality, and Drug Addiction, also presented the higher indicators of anxiety in the BAI and depression in the BDI. In another study, conducted in Turkey, with 271 college students, data suggested that the subjects more prone to Internet addiction were those who had higher scores in the Neuroticism and Introversion dimensions in EPQ associated with high scores in the BAI and BDI (Dalbudaka & Evrenb, 2014).
Also, positive correlations were found between the Harm Avoidance dimension from the Temperament and Character Inventory - Revised (TCI-R) and symptoms of depression (BDI) and anxiety (BAI), in a sample with 347 subjects from Finland. Similarly, this dimension of personality and the total scores of BDI and BAI were positively correlated with instruments for the investigation of mental disorders throughout life and in the family history of subjects, as well as psychiatric treatment in the past 12 months (Jylha & Isometsa, 2005).
As observed, there is a fair number of studies involving the assessment of personality characteristics and symptoms of anxiety and depression. However, few studies used instruments to assess personality traits in pathological levels. Among the few studies in this context, Trull and Goodwin (1993) conducted a longitudinal study for 6 months, with a sample of 44 subjects diagnosed with personality disorders. Significant and positive correlations were found between the symptoms of anxiety (BAI) and the obsessive-compulsive personality disorder, as well as positive correlations between the avoidant personality disorder and symptoms of depression (BDI). Dougherty, Bjork, Huckabee, Moeller, and Swann (1999) investigated a group of women who were hospitalized and diagnosed with borderline personality disorder, and found significant associations between symptoms of anxiety in BAI and depression in BDI with the aggressive and impulsive behaviors presented by these patients, in comparison with a control group. Skodol, Geier, Grant, and Hasin (2014) also conducted a study administering two tests in a sample of 34,653 subjects for 3 years. All disorders classified in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) were evaluated. The data collected showed that all personality disorders are predictors of anxiety disorders.
Based on the data presented, and considering the lack of studies in Brazil assessing pathological personality characteristics and symptoms of anxiety and depression, the aim of this study was to investigate whether symptoms of anxiety and depression are associated with pathological characteristics of personality in a non-clinical sample. We have as hypothesis (hi) that individuals who present higher scores (ie, profile with higher scores in comparison to the other group) in the instrument for assessing pathological personality characteristics (IDCP) should also have higher scores in the BDI and BAI in comparison to people with low scores in BDI and BAI. Furthermore, (h2) it was expected that subjects with more symptoms of depression or anxiety would present more specific personality profiles.
METHOD
Participants
There were 106 participants of 18 to 45 years (M=24.3, SD = 5.71), of both genders (65 women; 61.3%), chosen by convenience at a university in the countryside of the state of São Paulo. Two subjects reported being under psychiatric treatment, eight in psychotherapy, and five reported the use of psychotropic medication. As some participants showed missing data, we analyzed 98 cases.
Instruments
We used the Dimensional Clinical Personality Inventory ([IDCP]; Carvalho & Primi, in press A) to assess pathological personality characteristics. The IDCP consists of 12 dimensions (internal consistency values by Cronbach's α in brackets): Dependency (0.91), Aggressiveness (0.93), Mood Instability (0.93), Eccentricity (0.93), Attention Seeking (0.85), Distrust (0.88), Grandiosity (0.89), Isolation (0.83), Critical Avoidance (0.83), Self-sacrifice (0.82), Conscientiousness (0.62), and Impulsivity (0.72). It is noteworthy that almost all dimensions presented adequacy regarding internal consistency, considering a cutoff point of 0.70 (Nunnally, 1978), except for Conscientiousness, which was already reported in previous literature (Carvalho & Primi, in press A). It is a self-report instrument, consisting of 163 items, which should be completed according to a 4-point Likert-like scale, ranging from "it does not describe me at all" (1) and "it describes me accurately" (4)". The IDCP dimensions demonstrated adequacy in relation to the psychometric proprieties (Carvalho & Primi, 2015; in press; Carvalho, Primi & Stone, 2014). The approximate time of administration was 25 minutes.
To assess anxiety symptoms, we used the Beck Anxiety Inventory (BAI; Cunha, 2001). The BAI is an instrument for the evaluation of anxiety symptoms, consisting of 21 items, which should be completed in a Likert-like scale of 4 points, which refer to the presence or absence of symptoms. The time for administration was approximately 10 minutes. The national version of the instrument showed adequate psychometric properties (Cunha, 2001). The internal consistency (Cronbach's α) of the BAI in this study was 0.91.
Depressive symptoms were assessed with the Beck Depression Inventory (BDI; Cunha, 2001). It consists of 21 items in a Likert-type scale from 0 to 3 points, which relate to the frequency or absence of symptoms. The administration time was approximately 10 minutes. Psychometric studies by Cunha (2001) indicated satisfactory indices of reliability and validity. In this study the BDI had an internal consistency (Cronbach's α) of 0.89.
Procedures
After approval of the research project by the Research Ethics Committee (CAAE 0350.0.142.000-08), we proceeded to the collection of data. All participants were approached in classrooms or on the university campus, from different scholar semesters. The time to respond the instruments was on average 50 minutes. Before participating, all subjects signed the Informed Consent Form (ICF).
Data analysis
Based on the objectives of this study, we proceeded to the ANOVA, including effect size calculation (p) and post hoc analysis with groups formed according to the scores in the BDI and the BAI, separately, in IDCP dimensions. In addition, the graphics were printed with the profiles of the groups in the IDCP dimensions, separately by the BDI and the BAI. Data were analyzed only when there was no missing data in item level; significance level was ≤ .05 and effect size (Cohen's d) was interpreted as expressive from .20.
RESULTS
We found that the participants presented minimum (n=73), mild (n=19), and moderate (n=6) symptoms, and nobody presented severe symptoms of depression. Afterwards, the groups were compared using ANOVA and the respective Cohen's d values were calculated in relation to the IDCP dimensions, as shown in Table 1.
Table 1 Means, standard deviation and Cohen's d on levels of depression (BDI) and dimensions of the IDCP.
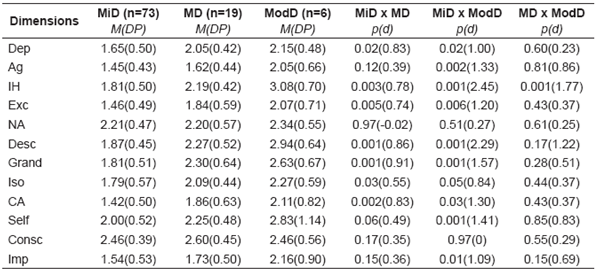
Note. Dep=Dependency; Ag=Aggressiveness; MI=Mood Instability; Exc=Eccentricity; AS=Attention Seeking; Dist=Distrust; Grand=Grandiosity; Iso=Isolation; CA=Criticism Avoidance; Self=Self-sacrifice; Consc=Conscientiousness; Imp=Impulsivity; MiD=Minimal Depression; MD= Mild Depression; ModD= Moderate Depression.
The data suggest that the higher the score in personality pathological characteristics in ten of the twelve dimensions, the greater is the change to be rated at the highest levels of depression, i.e., there is a gradual increase in the means of the IDCP according to the increase in the categories (minimum, mild, and moderate) of depressive symptoms. For two dimensions, this increase was not verified: Attention Seeking and Conscientiousness. Also, most data were significant (excluding the two dimensions mentioned) for the comparisons minimum x mild and minimum x moderate, but not for mild x moderate. This can also be observed by the d coefficients obtained, with the most significant being those between minimum x moderate, followed by minimum x mild, and, finally, mild x moderate. Concerning Table 1, it can also be verified that the highest means refer to the Selfsacrifice dimension and the lowest, to Criticism Avoidance, excluding Attention Seeking and Conscientiousness.
In a post hoc analysis, it was found that the subjects in the groups minimum symptoms x moderate symptoms differed in five dimensions of the IDCP (Dependency, Eccentricity, Grandiosity, Criticism Avoidance, and Impulsivity); while the minimum and mild x moderate groups differed in four (Aggressiveness, Mood Instability, Distrust and Self-sacrifice); the groups did not differ in the dimensions Attention Seeking, Isolation, and Conscientiousness. Complementary to these data, Figure 1 provides a graphical analysis of the profiles of participants from the three groups (according to level of depressive symptoms) in the IDCP dimensions.
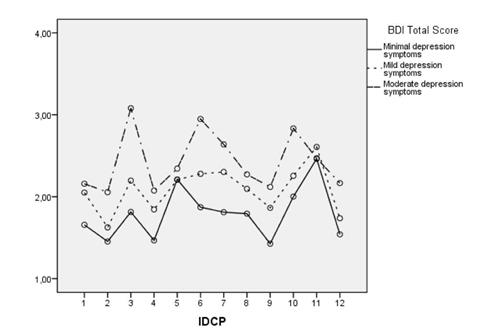
Note. 1=Dependency; 2=Aggressiveness; 3=Mood Instability; 4=Eccentricity; 5=Attention Seeking; 6=Distrust; 7=Grandiosity; 8=Isolation; 9=Criticism Avoidance; 10=Self-sacrifice; 11=Conscientiousness; 12=Impulsiveness.
Figure 1 Profiles of the groups by symptoms of depression in the IDCP factors
According to the figure, the most different dimensions considering the profile with moderate symptoms in relation to others are Mood Instability, Distrust, Self-sacrifice, and Impulsivity. It is also noteworthy that the group with fewer symptoms presented significantly lower scores in the dimensions Eccentricity and Criticism Avoidance.
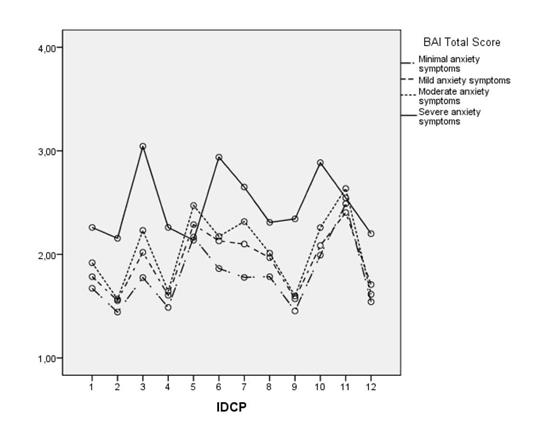
The same analyzes were performed with the BAI variables, referring to the anxiety symptoms. Descriptive analyzes revealed minimal (n=63), mild (n=20), moderate (n=16), and severe (n=5) levels of anxiety symptoms. Of the total number of participants, two did not answer. Tables 2 (descriptive data) and 3 (inferential data), show the data referring to the means in the IDCP dimensions according to the categories of symptomatology severity of anxiety, which were thus divided so as to facilitate the display in accordance with the number of columns.
Table 2 Means and standard deviation on levels of anxiety and dimensions of the IDCP.
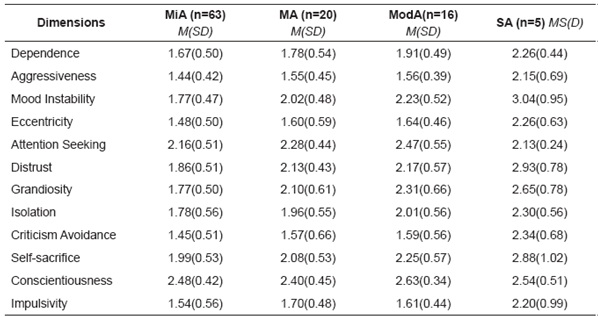
Note: MiA= Minimal Anxiety; MA= Mild Anxiety; Mod=Moderate Anxiety; SA= Severe Anxiety.
Similarly to what was demonstrated for depressive symptoms, there is a clear progression in the IDCP means due to the increase in severity in the BAI categories. An exception to this occurred in the dimensions Attention Seeking and Conscientiousness. Furthermore, by excluding these two dimensions, the highest means were in the dimensions Self-sacrifice and the lowest in Criticism Avoidance and Aggressiveness. Overall, considering the major differences among all groups demonstrated by d (Table 3), the highest scores were in the dimensions Mood Instability and Distrust, with the most significant ones in the comparisons with the severe group.
Table 3 Associations between levels of anxiety and classification in the IDCP dimensions.
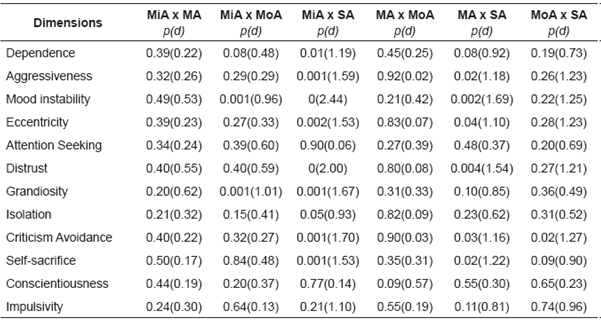
Note: MiA= Minimal Anxiety; MA= Mild Anxiety; MoA= Moderate Anxiety; SA= Severe Anxiety. Significance= p≥0.05
Also, the post hoc analysis showed that the subjects from the groups minimum x severe symptoms differed in the dimensions Dependence, Grandiosity, and Impulsivity; subjects in the groups minimum, mild, and moderate x severe symptoms differed in six dimensions (Dependency, Mood Instability, Eccentricity, Distrust, Criticism Avoidance, and Self-sacrifice); and the groups did not differ in the dimensions Attention Seeking, Isolation, and Conscientiousness, as also observed in the BDI. Figure 2 shows the Graphic with the profiles of the participants in the IDCP according to the scores in anxiety symptoms by BAI. The means in the dimensions Mood Instability, Distrust, Criticism Avoidance, Self-sacrifice, and Impulsivity for the group with severe symptoms are noteworthy.
DISCUSSION
The objective of this research was to investigate relations between symptoms of depression and anxiety with pathological personality characteristics. The hypotheses formulated for this study were corroborated. The subjects who obtained the highest scores in the IDCP dimensions also presented higher scores in the BAI and BDI (h1) as well as specific profiles in IDCP dimensions according to a greater classification in the symptoms of depression and anxiety (h2).
The data showed a higher frequency of low symptomatic levels of depression and anxiety in the general population, which was expected (Cunha, 2001), reflecting what usually occurs in samples from the general population. We must highlight that the same can be pointed out in relation to pathological personality traits, as a high occurrence of these traits is not expected; however, we do observed variability in sample. In addition, published data indicated a trend to higher scores in symptoms of depression and anxiety in cases of clinical samples (Dougherty et al., 1999; Skodol et al., 2014). The progression of the IDCP means in the BAI and the BDI supports the first hypothesis (h1), except for two dimensions: Attention Seeking and Conscientiousness.
The non-progression in the means of these two dimensions in terms of severity in the pathological functioning is in contrast with what was observed by Carvalho and Primi (in press A) and Carvalho, Primi and Stone (in press), i.e., higher mean scores (total and theta scores; the latter from IRT Rasch model) in these dimensions compared to the others in the IDCP, suggesting that these dimensions tend to assess more healthy aspects than expected for the instrument. It is likely that the progressive standard presently found in 10 IDCP dimensions will not repeat for Attention Seeking and Conscientiousness, due to the difference in the range assessed by these two dimensions in the personality continuum. It is noteworthy that both dimensions were reviewed in previous studies, in an attempt to adjust the level of measurement of personality traits (Carvalho, Capitão, Sette, & Primi, 2014; Carvalho, Souza, & Primi, 2014).
We also noted that the highest means in the BDI and BAI were in the dimension Self-sacrifice, and the lowest in Criticism Avoidance. This suggests that the subjects in this study with more depressive and anxiety symptoms tended to present characteristics of exaggerated self-disregard and excessive attitudes of consideration and help to others, implying losses to themselves. Moreover, in contrast, they did not present beliefs of incompetence, humiliation, and criticism by others. These data do not allow for the development of hypotheses about these means in anxiety and depression symptoms with the profiles of these two IDCP dimensions, which suggests the need for verification in future studies. On the other hand, this pattern reflects what was found by Carvalho & Primi (in press A), i.e., the general population seems to tend to present higher means for Self-sacrifice and lower means for Criticism Avoidance compared to the other dimensions the IDCP.
Also, the major discrepancies between the groups (established according to symptoms), found both in the BAI and the BDI were in the Mood Instability dimension. This indicates that the greater the incidence of depressive and anxiety symptoms, the greater the predisposition to report psychological discomfort, tendency to mood instability, and low resilience (Carvalho & Primi, 2015). These data are consistent, since the tendency to psychological discomfort in general and low resilience is related to the presence of psychiatric symptoms (Dougherty et al., 1999; Skodol et al., 2014; Thomas & Alchiery, 2005; Trull & Goodwin, 1993), with a relation that was found in previous studies with this dimension of IDCP (Carvalho & Primi, in press).
With respect to the profiles in the IDCP established in accordance with symptomology severity levels in the BDI and the BAI, it was observed that only the most severe groups in terms of depressive (mild symptoms) and anxious (severe symptoms) symptoms had different profiles from those of groups with minor symptoms. This finding was expected and is in line with h2 of this study, i.e., individuals with more significant symptoms of depression and anxiety must present typical profiles when assessed for pathological personality characteristics.
In the case of the BDI, the dimensions with larger discrepancies were Mood Instability, Distrust, Self-sacrifice, and Impulsivity. These findings are consistent to the extent that individuals with high scores for Mood Instability, as pointed out before, tend to present psychiatric symptoms in general; while subjects with high scores for Distrust may tend to isolate themselves (because they cannot believe people) and present beliefs that others may harm them, which may increase the chance of comorbidity with depressive episodes (Thomas & Alchieri, 2005). Regarding Self-sacrifice, the items of this dimension are related, among other things, to a predisposition to ignore oneself towards the others, which can be considered a symptom of depression (Del Porto, 1999). However, we did not find any data in the literature to support the highest score in this group for the Impulsivity dimension, which should be investigated in future studies. Nonetheless, some sample specificity is the best explanation for this finding as there is no clearly overlap between depression symptoms and the impulsivity trait (Millon, 2011).
In the BAI, discrepancies were found in the same dimensions, and also in the Criticism Avoidance dimension. Higher scores in Mood Instability are consistent, such as reported, and also in Distrust, since individuals with high scores in this dimension tend to constantly fear that others may harm them (Carvalho & Primi, 2015), being anxiety a typical symptom of paranoid functioning (Millon, 2011). The discomfort triggered by anxiety may also be present in people with high scores in the Self-Sacrifice dimension, considering that this dimension includes a constant concern in placing the other above everything. Regarding Impulsivity, although there are no studies with IDCP demonstrating any relation of this dimension directly with anxiety, it is reasonable to hypothesize that more impulsive people also tend to be more anxious (Britto & Benetti, 2010; Junior et al., 2014). Still, the discrepancy in Criticism Avoidance is consistent and expected, since this dimension is related to a constant concern that people around may be harmful (Abela, 2013; Carvalho & Primi, in the press A), which is typical of avoidant functioning (APA, 2013; Millon, 2011).
FINAL CONSIDERATIONS
The findings reported here contribute to the understanding of the relationship between these constructs in a non-clinical sample, adding to what is already reported in the literature. The present findings suggest that professionals, mainly clinicians, should pay attention to the presence of pathological personality traits when facing clients with high scores on depressive and/or anxiety symptoms. Besides that, specificity should be observed in relation to pathological personality traits between clients high only in depression and clients high only in anxiety. The main limitation relates to the sample size, besides the non-specificity of the BDI and the BAI in the assessment of the symptoms evaluated, taking into consideration that only the calculation of total scores is possible in both cases.
Future studies should seek to deepen the data that were not expected, especially the relationship between high scores of depression and impulsivity. Likewise, further studies should also verify the pattern of relation between the dimensions Attention Seeking and Conscientiousness in their revised versions with depressive and anxiety symptoms. Finally, the data here evidenced should be replicated in clinical populations.

