










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.26 no.4 Bogotá Oct./Dec. 2011
Muriatic acid: digestive exposure, case report and literature review
Nicolás Rocha, MD (1), Diego Aponte, MD (2), Rigoberto Montoya, MD (2)
(1) Resident in Gastroenterology at the Clínica Universitaria Colombia in Bogotá, Colombia.
(2) Gastroenterologist at the Clínica Universitaria Colombia in Bogotá, Colombia.
Translation from Spanish to English by T.A. Zuur and The Language Workshop
Received: 02-02-11 Accepted: 11-10-11
Abstract
Digestive tract burns can create high levels of comorbidity in an exposed patient although these levels depend on the different capacities to cause harm of alkalis and acids. The ideal moment for endoscopy in these cases is currently being debated as a patients post burn reactions may be devastating. We present the case of a patient who attempted to commit suicide by ingesting muriatic acid including clinical findings, complications and management.
Key words
Digestive burn, muriatic acid, endoscopy.
INTRODUCTION
The ingestion of caustics and poisoning caused by these substances are serious threats because of the devastating consequences they can produce. They are considered to be a serious medical and surgical problem due to the high rates of morbidity and mortality that ensues. Initial treatment and early endoscopy are fundamental in the management and for the prognoses of patients with caustic digestive tract burns.
We present the case of a patient who had attempted suicide and who had resulting secondary digestive burns caused by muriatic acid.
CLINICAL CASE
A 25 year old woman who had been healthy arrived at the intensive care unit because of heartburn and posterior abdominal pain following prior to attempted suicide by voluntary ingestion of muriatic acid. Upon admission the patient was in pain and experiencing tachycardia. She had mild epigastric pain but no signs of peritoneal irritation or other symptoms upon physical examination. The laboratory tests showed an important leukocyte reaction in the complete blood count. A chest x-ray and high digestive tract endoscopy were performed. The thorax x-ray showed no alterations, but endoscopy found evidence of III or IV degree burns on the Zargar scale in the esophagus and stomach (Figures 1, 2, 3 and 4). Since there was a high risk of perforation, it was decided not to use a nasogastric feeding tube, but to use parenteral nutrition instead.

Figure 1. Esophagus with edema, erythema and friable membranes.
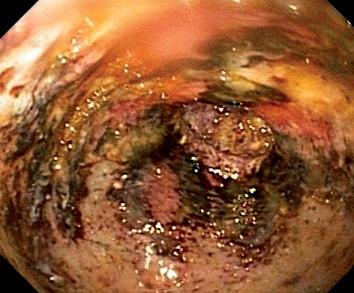
Figure 2. Antrum (Pale mucosa with fibrinoid necrotic material).

Figure 3. Gastroesophageal union with wide cardia.
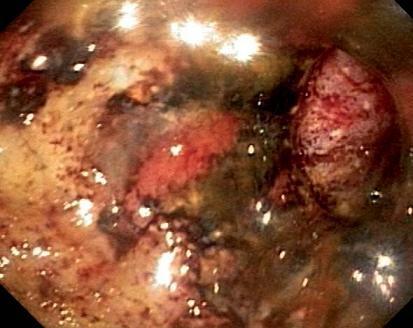
Figure 4. Antrum with extensive necrosis.
During the patient´s subsequent evolution she presented hyporexia, emesis and constant nausea. Another endoscopy was performed which uncovered fibrosis scars in the antrum with serious retraction and secondary pyloric stenosis. The stenosis was treated with balloon dilation without complications leading to an improvement in her symptoms (Figures 5, 6, 7 and 8).

Figure 5. Band of scarring in antrum

Figure 6. Pyloric stenosis

Figure 7. Balloon dilation

Figure 8. After balloon dilation
DISCUSSION
Although the epidemiology of these burns is not completely known, between 5,000 and 18,000 cases are reported each year in the USA (1). Accidental ingestion of caustic materials usually affects children while voluntary ingestion causes serious injuries in adults (2). Suicide attempts using caustics create very large alterations in the esophagus and stomach.
The pathophysiology of caustic burns caused by acid differs from that of burns caused by or alkalis. Acids generally cause coagulation necrosis which sometimes creates a protective barrier that can stop the lesion and its proliferation. In contrast, alkalis create liquefaction necrosis which destroys cellular membranes through saponification and thrombosis which worsen lesions and result in esophageal perforations and greater complications than those caused by acids (3).
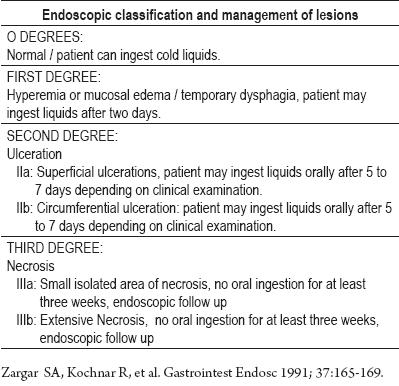
Throughout history there have been different classification systems for this type of burns in order to optimize management of these patients. The type of management is determined by the degree of the lesion (Table 1).
Table 1. Endoscopic classification and management of lesions.
Other complications that should be taken into account include basic life support, analgesics, mucous protectors (sucralfate), proton bomb inhibitors and anti H2. Although, there are no controlled studies regarding adequate and safe time for performance of endoscopy for this type of patients, the procedure should usually be performed as soon as possible between within the first 6 to 12 hours (4).
Antibiotics only play a useful role when there is perforation and the possibilities of complications and consequences. Treatment with steroids has shown no benefit (5).
These types of burns can generate long term sequelae due to stenotic lesions. They usually occur around the esophagus where about 70% of patients present dysphagia because of permanent lesions in which scarring fibrosis replaces muscular tissue of the enteric plexus (6). Once the acute episode is resolved, the treatment focuses on sequelae and late complications. It is also accepted that the sequelae in this type of patient increases the risk of esophageal cancer (both adenocarcinomas and squamous) (7).
The physical evolution of the patient studied was adequate, and she began to ingest tolerable liquids after parenteral nutrition.
REFERENCES
1. Gumaste VV, Pradijuman BD. Ingestion of Corrosive Substances by adults. American Journal of Gastroenterology 1992; 87: 11-15.
2. Bautista CA, Estevez ME, Varela CR, et al. A retrospective analysis of caustic ingestion substances by children. Ten year statistics in Galicia. Eur J Pediatr 1997; 156: 410-414.
3. Jones A. Caustic Ingestions. Techniques in Gastrointestinal endoscopy 2002; 4(4): 196-200.
4. Broto J, Asensio M, Joro CS, et al. Conservative treatment of caustic esophageal injuries in children: 20 years of experience. Pediatr Surg Int 1999; 15: 323-325.
5. Ulman I, Mutaf O. A critique of systemic steroids in the management of caustic esophageal burns in children. Eur J Pediatr Surg 1998; 8: 71-74.
6. Dantas RO, Mamede RC. Esophageal motility in patients with esophageal caustic injury. Am J Gastroenterol 1996; 91: 1157-1161.
7. Mamede RC, de Mello Filho FV. Ingestion of caustic substances and its complications. Sao Paulo Med J 2001; 119: 10-15.
1. Gumaste VV, Pradijuman BD. Ingestion of Corrosive Substances by adults. American Journal of Gastroenterology 1992; 87: 11-15. [ Links ]
2. Bautista CA, Estevez ME, Varela CR, et al. A retrospective analysis of caustic ingestion substances by children. Ten year statistics in Galicia. Eur J Pediatr 1997; 156: 410-414. [ Links ]
3. Jones A. Caustic Ingestions. Techniques in Gastrointestinal endoscopy 2002; 4(4): 196-200. [ Links ]
4. Broto J, Asensio M, Joro CS, et al. Conservative treatment of caustic esophageal injuries in children: 20 years of experience. Pediatr Surg Int 1999; 15: 323-325. [ Links ]
5. Ulman I, Mutaf O. A critique of systemic steroids in the management of caustic esophageal burns in children. Eur J Pediatr Surg 1998; 8: 71-74. [ Links ]
6. Dantas RO, Mamede RC. Esophageal motility in patients with esophageal caustic injury. Am J Gastroenterol 1996; 91: 1157-1161. [ Links ]
7. Mamede RC, de Mello Filho FV. Ingestion of caustic substances and its complications. Sao Paulo Med J 2001; 119: 10-15. [ Links ]

