











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkA 71-year-old hypertensive male who was an active smoker (IPA 51) was admitted to the emergency room due to progressively decreasing bilateral eyesight to the point of bilateral amaurosis, without ocular pain. This was associated with a chronic bilateral pulsatile frontal headache. A brain NMR showed diffuse meningeal thickening related to pachymeningitis. A meningeal biopsy showed pachymeninge. Neoplastic, infectious and autoimmune causes were ruled out; therefore, it was considered to be idiopathic hypertrophic pachymeningitis (IHP).
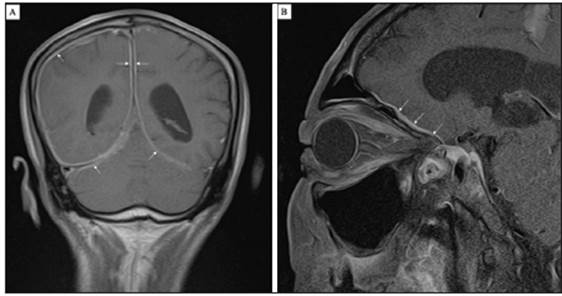
Figure 1. A: Brain NRM with gadolinium, coronal view. Diffuse meningeal thickening, mainly on the right, with significant enhancement on diffuse gadolinium application, compatible with pachymeningitis. B: Orbital NRM with gadolinium. Diffuse pachymeningitis changes which reach the left and right orbital fissures.
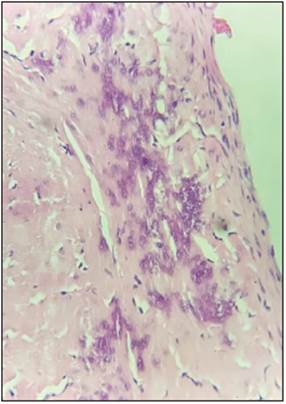
Figure 2. Meningeal biopsy (H&E 40X). Fibroconnective tissue can be seen, with fibroblast proliferation, increased collagen, cal cifications and mononuclear inflammatory infiltrate throughout its thickness, compatible with pachymeninge.
Hypertrophic pachymeningitis is a rare clinical entity characterized by localized or diffuse thickening of the dura mater, with or without associated inflammation. It causes progressive neurological deficit due to compression of the adjacent structures 1.
Headache is the most common initial symptom, followed by ophthalmological symptoms such as vision loss and diplopia 2.
Its etiology is multifactorial. Dural thickening in the posterior cranial fossa, mimicking the Eiffel Tower illuminated at night (Eiffel-by-night sign), is found on imaging studies.

