text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Pregnant women go through a critical moment in their lives. Pregnancy has multiple connotations: it is a biological process, but it is also a social one occurring in a complex and dynamic context; however, the studies tend to concentrate on biological, individual aspects, as well as on diseases, focusing almost exclusively on the fetus and leaving aside the value of women. Therefore, pregnancy and the health of pregnant women are seen, understood, and dealt with in a fragmented, functionalist manner.1
The oral health of pregnant women is an essential component of their health and life. However, the relationship between pregnancy, oral health, dental care, and associated social factors seem to be underestimated in the literature, agreeing with the logics of society concerning the biological understanding of pregnancy and the care it requires. In addition, the big inequities in terms of oral health and dental care of pregnant women make it necessary to conduct new comprehensive research to approach the complexity of this phenomenon and its influencing processes.2
In terms of epistemological perspectives, research on these topics seem to be predominantly addressed from positivism, and rarely from phenomenological and critical approaches.3 However, the literature lacks publications that allow to recognize the topics that tend to be researched in this field, the epistemological perspectives commonly used to approach this field of inquiry, or the prevalent research techniques.
In consequence, one may think that research on these topics is understood in various ways and approached from different perspectives. Hence the interest in the task of characterizing the publications, authors, and institutions researching these topics, assessing the quality of publications, and analyzing the content of related articles, in order to identify the ontological, epistemological, and methodological aspects of the scientific production related to these topics.
METHODOLOGY
The following process was followed for the bibliometric study, systematic review, and content analysis:
First, the literature search plan was formulated, identifying the search terms in the MeSH thesaurus of the PubMed/Medline database using the key words of the specialized literature found in exploratory search. Terms were selected and used consistently in each consulted database, according to the specific search syntax for each system, so the search commands could vary in form, but not regarding the contents obtained (Scopus, developed by Elsevier; PubMed/Medline, by the National Library of Medicine in the United States; and the main collection of the Web of Science databases developed by Thomson Reuters, especially Science Citation Index Expanded and Social Sciences Citation Index. It must be noted that results of SciELO national collections were obtained by this last platform). Terms were also searched in the sources of consultation of grey literature with no restriction in the search period (until the second half of 2014). Search equations were created from the key words, thus creating a list of articles. Duplicates were later identified, selecting the publications that were finally included in this study. The search expressions were set as follows:
(“social determinants of health” OR “multilevel analysis” OR “social gradient*” OR “social capital” OR inequality* OR ethnic* OR gender OR “social class” OR ecosocial OR psychosocial OR “collective health” OR “social network” OR “social support”) AND (“oral health” OR “oral disease*” OR “dental service*” OR caries OR periodontitis OR “dental care”) AND (pregnant* OR “women’s health”)
(“social determinants of health”) AND (“oral health” OR “oral disease” OR “dental care” OR caries OR periodontitis OR “dental care”) AND (pregnant women OR “women’s health”)
(“social determinants of health” OR “multilevel analysis” OR “living standard” OR “social capital” OR inequality OR ethnic* OR sex OR “Socioeconomic Status” OR ecosocial OR “social support” OR “collective health” OR “social network” OR “social support”) AND (“oral health” OR “oral disease” OR “dental care” OR caries OR periodontitis OR “dental care”) AND (“pregnant women”)
(“social determinants of health” OR “multilevel analysis” OR “social gradient*” OR “social capital” OR inequality* OR ethnic* OR sex OR “social class” OR psychosocial OR “collective health” OR “social network” OR “social support”) AND (“oral health” OR “oral disease*” OR “dental service*” OR caries OR periodontitis OR “dental care”) AND (pregnant OR “women’s health”)
Eligibility of articles was then confirmed. To do this, two examiners independently evaluated titles and abstracts of the described search results to determine eligibility of the articles according to the inclusion criteria set in this study. In case of differences in the examiners’ analysis for article eligibility, a third examiner was consulted in order to settle the difference. Articles that were classified as eligible, as well as those that were not easily identified as eligible based on their abstract or title, were obtained in full text in order to confirm inclusion or exclusion.
Characterization of the process of bibliography search and selection
The Web of Science, PubMed and Scopus databases were used for the systematic review, yielding 412 articles. This corpus of articles went through a first filter, which consisted in eliminating exact duplicates. 138 articles were discarded for overlapping (Web of Science and PubMed = 31; PubMed and Scopus = 78; Scopus and Web of Science = 3; PubMed, Scopus, and Web of Science = 26-the latter when publications appeared in the three databases at the same time, while in all the others the articles appeared in just two of the explored databases), keeping 274 articles. The selected articles went through a second filter, discarding those that were not related to the topic or were incomplete. Thus, 67 articles were excluded, leaving 207. Then, 21 articles and documents found in the grey literature were added, for a partial total of 228 texts used for the bibliometric analysis. 131 articles were eliminated because full texts were not obtained, and thus the final selection consisted of 97 articles that met the inclusion criteria and were used for systematic review and content analysis Figure 1.
Once the articles were selected, the following steps were taken:
Bibliometric analysis: 4 extraction of the structured data from the 228 texts from the corpus in machine-readable formats (.csv, .ris, .txt. .xlsx) using text mining software (Vantage Point, licensed by Search Technology Inc., academic version 9.0 by subscription). Activity indicators were obtained according to aggregation levels (frequency of publication by years, countries, institutions, and authors), and relation (co-authorship). All this required a detailed reading of the corpus, in order to refine and normalize the data.
The systematic review was conducted by retrieving information related to authors, years, language, country, journal, and study type. Once eligibility was confirmed, and with the selected articles in full text, two examiners conducted independent analysis of the methodological quality of each article through the Strobe guidelines for observational studies,5 Consort guidelines for clinical trials6 and Prisma guidelines for systematic reviews. 7
For content analysis of articles and documents obtained in full text (97 publications), the researchers identified the categories concerning ontological, epistemological, and methodological aspects related to oral health, dental care, pregnant women, and social determinants in these documents-analysis based on Piñuel’s remarks-.8 The information obtained from the analyzed works was processed in the Atlas-ti 6.0 software according to categories related to the ontological, epistemological, and methodological aspects, based on Breilh’s observations on the way researchers understand their object of study (ontological), have a close relationship with the paradigms from which they “see reality” (epistemological), and develop research (methodological).9
RESULTS
From the bibliometric analysis
The purpose of a bibliometric analysis is to characterize the dynamics of the publication of research results from documents indexed in mainstream bibliographic databases, as well as in grey literature sources, according to the chosen aggregation levels (countries, institutions, and authors), in order to provide a panoramic review of the dynamics of publication of research results chosen for this study in particular. Such panoramic review allows evaluating the impact of research and contextualizing specific research projects. Table 1 outlines the bibliometric indicators of countries with five or more records and their respective institutions and authors.
Table 1 Countries of affiliation with five or more records in the corpus. Institutions and authors associated to two or more documents (data analyzed with Vantage Point, academic license 9.0 by subscription, Search Technology Inc.)
| Countries (number of records) | % of participation in the corpus | Institutions (number of records) | Authors (number of records) |
|---|---|---|---|
| United States (81) | 35.52 | University of North Carolina (7) University of California (San Francisco) (7) New York University (5) Harvard University (4) University of Illinois (4) | Boggess, K.A (3) Beck, J.D (3) Lukacs, J.R (3) Milgrom, P (3) Offenbacher, S (3) |
| United Kingdom (22) | 9.64 | University College London (4) University of Bristol (4) University of Sheffield (3) | Lamarca, G.A* (3) Sheiham, A (3) Vettore, M.V (3) Batty, G.D. (2) |
| Brazil (20) | 8.77 | Universidade Estadual de Campinas (3) Universidade Federal do Rio de Janeiro (3) Universidade de São Paulo (3) Fundação Oswaldo Cruz (3) | Lamarca, G.A. ᵆ (3) Leal, M.D.C (3) Barbieri, M.A (2) |
| Australia (17) | 7.45 | Australian Research Centre for Population Oral Health (University of Adelaide) (7) University of Adelaide (2) | Jamieson, LM (5) Broughton, J. (3) Parker, E.J (3) Roberts-Thomson, KF (3) |
| Colombia (12) | 5.26 | Universidad del Valle (5); Universidad Santo Tomás (4) Universidad Nacional de Colombia (2) | Concha Sánchez SC (4) Corchuelo Ojeda J (3) |
| India (11) | 4.82 | Manipal University (3) | Kumar, A (2) |
| New Zealand (10) | 4.38 | University of Otago (7) | Morgaine, K.C (2) Thomson, W.M (2) |
| Canada (9) | 3.94 | University of Toronto (7) | Lawrence, H.P (5) |
| Japan (7) | 3.07 | Tokyo Dental College (2) National Center for Child Health and Development (2) Tokushima University (2) | Takaesu, Y (2) |
| France (5) | 2.19 | Université Paris VII Denis Diderot (2) INSERM (2) | Bouchard, P (2) |
* Dual affiliation declared in an article.
Frequency of publication by countries of affiliation, institutions, and authors
In 81 documents, the authors state that they belong to universities, institutions, and research centers in the United States. In 57 documents, the authors refer affiliations in Europe, of which 22 records belong to the United Kingdom. 28 records indicate affiliations in Australia, New Zealand, and Fiji. The authors in 36 records belong to institutions in Asia, mostly in India (11 records). 8 records include authors affiliated with institutions in Africa, South Africa, Kenya, Uganda, and Nigeria. Affiliations to Latin American countries are declared in 43 records, in which Brazil is a majority (20 records), followed by Colombia (12 records) and Mexico (3 records). Independent investigators were found in 3 records, and 6 records reported undefined information regarding the authors’ institutional affiliation.
296 institutional affiliations were identified. Most institutional affiliations correspond to the University of North Carolina, United States (9 documents), followed by the Australian Research Centre for Population Oral Health, of the University ofAdelaide, Australia (8 documents). 89 identified affiliations correspond to institutions in the United States and Canada. 48 institutional affiliations were identified in Latin America, mostly in Brazil (23 institutions). However, the Universidad del Valle, Colombia, and the Universidad Santo Tomás, Bucaramanga, appear in most of the records of this region, in 5 and 4 documents respectively Table 1. 801 authors were identified (274 affiliated to institutions in the United States and Canada), 122 of whom are affiliated with institutions in Latin America.
According to the number of records, the authors with most publications are Lawrence, HP (5 records, University of Toronto, Canada); Jamieson, LM (5 records, Australian Research Centre for Population Oral Health); Boggess, KA (4 records, University of North Carolina, United States); Broughton, J. (4 records, University of Otago, New Zealand); Concha Sánchez, SC (4 records, Universidad Santo Tomás, Bucaramanga, Colombia); and the group of authors from the University of Szeged in Hungary (4 records; Gorzo I, Novak T, Pal A, Radnai M and Urbán, E) Table 1; figures 2A, 2B, 2C and 2D of co-occurrence maps based on number of articles coauthored and without international co-authorship).
International co-authorship
International co-authorship is more intense among researchers from institutions in New Zealand (80% of the records linked to that country were published in collaboration with researchers from the countries listed under this item), Canada (78% of their records), United Kingdom (50%) and Australia (47%). The international collaboration of authors from United States institutions corresponds to 17%. On the other hand, 35% of documents by authors affiliated with Brazilian institutions were published in international co-authorship, especially with institutions from the United States and the United Kingdom. Figures 2A, 2B, 2C and 2D show the internal and external co-authorship in the corpus of texts, according to the specified levels of aggregation.
The strongest cluster of institutions in terms of collaboration includes institutions from Australia (Australian Research Centre for Population Oral Health at the University of Adelaide; Flinders University; Curtin University; University of Newcastle; University of Melbourne; Deakin University), and New Zealand (University of Otago; Raukura Hauora O Tainui Trust; Waikato-Tainui College for Research and Development). This network of cooperation includes the University of Toronto (Canada), the Universidade Federal de Santa Catarina (Brazil), the University of North Carolina, and the University of Iowa (both from the United States). The collaboration among Latin American institutions is less representative, as it does not exceed three articles in international co-authorship, which could reflect the dispersion of interest in these research fields.
As for authors, the most prominent are Jamieson LM and Lawrence HP from the Australia-New Zealand-Canada cluster, whose studies were published between 2010 and 2014. Boggess KA is also noticeable (with publications in 2001, 2008, 2010, and 2011) of the cluster of authors from the University of North Carolina Figures 2A, 2B, 2C, and 2D).
From the systematic review
Data related to years of publication and study type
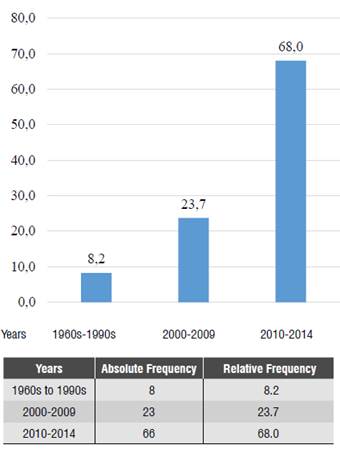
The description of studies according to period of publication shows that 8.2% of studies on this topic were conducted between the 1960s and the 1990s. The period 2000-2009 shows an increase of 23.7% in this type of publications; this means that publications related to this subject doubled in ten years, while between 2010 and 2014 it tripled over the previous decade, reaching a percentage of 68% Figure 3.
The description of publications according to study type shows that observational cross-sectional studies are predominant, with 36.1%, while studies traditionally considered of higher evidence, such as systematic reviews, meta-analysis, and clinical trials, as well as qualitative or mixed studies, are less common Table 2.
Table 2 Description of studies on oral health and dental care to pregnant women according to study type
| Study type | Absolute frequency | Relative frequency |
|---|---|---|
| Meta-analysis and systematic review | 3 | 3.1 |
| Controlled and uncontrolled clinical trials | 7 | 7.2 |
| Cohort study | 8 | 8.2 |
| Case-control study | 11 | 11.3 |
| Cross-sectional study | 35 | 36.1 |
| Population-based study | 11 | 11.3 |
| Review and case report | 15 | 15.5 |
| Qualitative or mixed study | 7 | 7.2 |
In terms of quality of the studies, these are the criteria with the lowest levels of compliance in the 64 articles evaluated by means of Strobe: use a flowchart; describe sensitivity analyses; explain the treatment of missing data; describe the reasons for participants loss in each phase; rate estimates of relative risk with estimates of absolute risk for a relevant period of time; describe other analyses carried out (subgroups, interactions, or sensitivity), and indicate the number of participants with missing data in each assessed variable.
Out of the seven articles analyzed with Consort, these are the criteria with the lowest level of compliance: indicate who generates the random allocation sequence, who registered participants and who assigns participants to the intervention; record the sources of funding and support and the role of funders; indicate, if applicable, who was blinded or masked following the intervention (e.g., participants, those who manage the intervention, those who evaluated the results), and how they evaluated the success of the masking technique process; and describe the mechanism used to implement the random allocation sequence.
Of the three articles assessed by means of Prism, the following criteria were not met: specify the studies’ details (e.g. peak and duration of follow-up) and the characteristics used as criteria for eligibility and validation (e.g. covered years, language, or publication status); describe an electronic search strategy in at least one database, including the limits used, so that it can be reproducible; present the number of studies that were screened, assessed for eligibility, and included in the review, and detail the reasons for exclusion in each stage, ideally using a flowchart.
From the content analysis
In ontological terms, the databases yielded articles focused on three core themes. The first theme focuses on women and how their specific biological condition, linked to puberty, pregnancy, lactation, menopause, and hormonal changes related to these events, make a difference in the oral condition and the needs for dental treatment in comparison to men throughout the life cycle.
The topics emerging in this thematic area refer to biological aspects, economy and work, gender roles, inequities in health, and curriculum in the dental field. Table 3 lists the authors whose publications are identified on this thematic area and in each of the abovementioned topics, as well as potential limitations identifiable in thesepublications Annex 1 lists the references of authors included in table 3). Studies related to this thematic focus advocate for differential care for men and women. However, they focus their attention on biological traits or analyze structural aspects without establishing connections with the overall and oral biological conditions faced by pregnant women.
Table 3 List of the topics, authors, limitations, and paradigms that focus on differences between men and women
| Topics | Authors* | Limitations | Paradigm |
|---|---|---|---|
| Biological aspects | Lukacs et al, Willis et al, Sinkford et al, Russell et al, Konttinen et al, Niessen et | Investigations focusing on biological aspects. They analyze structural aspects with no connections to biological aspects | Positivism |
| Economy and work | Watson et al | Positivism | |
| Gender roles | Silva | Critical | |
| Inequities in health | Senicato | Positivism | |
| Dentistry curriculum | Rezende | Positivism |
* SeeAnnex 1at the end of the article, which lists the references of the publications included intable 3.
In the second thematic area, the relationship between pregnancy, oral health, dental care, and social determinants in pregnant women is analyzed considering the impact of these aspects on the oral and overall health of their children, and therefore the real focus is on the result of the gestation instead of the condition of health, well-being, and quality of life of pregnant women. While recognizing the implications of these studies on children’s oral health, pregnant women become less important in this process, underestimating the impact of oral health and dental care on the life, health and quality of life of women during the gestation period. Table 4 outlines the topics and authors, but also the potential limitations of the studies Annex 2, at the end of the article, lists the references of authors included in table 4.
Table 4 List of the topics, authors, limitations, and paradigms that focus on the
| Topics | Authors* | Limitations | Paradigm |
|---|---|---|---|
| Result of pregnancy | Broughton et al, Do et al, Chamberlain et al, Mobley et al, Horowitz, Watson et al, Acuña-González et al, Chaffee et al, Rezende et et, Dos Santos, Rothnie et al | Pregnant women become less important. They underestimate the impact of oral health and dental care on the life, health and quality of life of these women. | Positivism |
| Interventions in pregnant women for the child’s health | Clifford et al, Chaffee | Positivism |
* SeeAnnex 2at the end of the article, which lists the references of the publications included intable 4.
The third thematic area, the relationship between pregnancy, oral health, dental care and its relationship to social aspects, focuses on pregnant women addressing several specific topics: the first topic relates to the biological changes that pregnant women experience at the immunological and microbiological levels, as well as at the periodontal and oral levels in general. These aspects become important in such studies, which tend to isolate the mouth from the rest of the body, as well as the social realities faced by pregnant women Table 5.
Table 5 List of the topics, authors, limitations, and paradigms that focus on the biological and social aspects of oral health and dental care of pregnant women
| Topics | Authors* | Limitations | Paradigm |
| Biological changes | Christian et al, Karunachandra et al, Rodríguez et al, Nayak et al | Relevance to biological aspects. They isolate the mouth from the rest of the body and the social reality of pregnant women. | Positivism |
| Pregnant women’s representations | Boggess et al, Jamieson et al, Abiola et al, Claas et al, Garvero et al, Córdova et al, Claro et al, Escobar et al, Urrea et al, Sourabha et al, Esa et al | Beliefs and knowledge about self-care. They blame women for their oral conditions. | Positivism, phenomenology |
| Clinicians’ representations | Alves et al, Zanata et al, Chi et al, Patil et al, Doyal et al | Professional representations should be strengthened. They focus investigative efforts on the individual: “the tip of the iceberg”. | Positivism, phenomenology |
| Interventions, access, barriers, and coverage of the health system | Thompson et al, Boggess et al , Geisinger et al, Kaushal et al, Machuca et al, Albert et al, Ramos-Gómez et al, Azofeifa et al, Ayala, Saddki et, Sánchez et al, Marchi et al | Reductionist fragmented view. Structural aspects are neglected. | Positivism |
| Inequality and social determinants of health | Lamarca et al, Corchuelo et al, Boillot et al, Wandera et al, Ben et al, Jamieson, Concha et al, Silva A | Social determinants as external factors. They do not integrate the social reality with the systemic and oral biological conditions of pregnant women. | Positivism, critical |
| Oral pathologies - adverse pregnancy events | Xiong et al, Contreras et al, Scannapieco et al, Baskaradoss et al | Biological aspects are emphasized. Reductionist fragmented view | Positivism |
* SeeAnnex 3at the end of the article, which lists the references of the publications included intable 5.
Pregnant women’s representations of oral health is another topic in this third thematic area. The studies show the influence of beliefs and knowledge on the self-care practices and the attendance of pregnant women to dental consultation. The studies hold pregnant women responsible for their oral health and dental care, based on the representations these women have built throughout their lives, which influence self-care and oral health practices during the process of gestation. A tendency to blame women for their oral situation can be observed in these studies Table 5.
The clinicians’ representations is another topic in this third thematic area. The studies show that clinicians’ representations about overall health, oral health, and pregnant women’s dental care must be strengthened, focusing much of the research efforts on aspects of individual order, with the consequent fragmentation of reality Table 5.
This third thematic area also highlights the studies that evaluate aspects related to the care provided to pregnant women in terms of specific oral health interventions seeking to solve the oral pathologies that may arise during pregnancy. These studies show pregnant women’s poor access to dental consultation, as well as the barriers they usually find. Other studies analyze the situation of oral health and dental care of pregnant women in terms of coverage of the health care system; most studies address the collective aspects of the relationship between pregnancy, oral health, and dental care over the individual level, although they fail to transcend the reductionist fragmented view, due to lack of knowledge on structural aspects Table 5.
In this thematic area, inequity and the social determinants of health are also addressed by researchers. Several studies focus on the theory of social capital and social networks, based on the theory of social gradient and on educational and socioeconomic conditions; some others analyze socio-demographic factors, or racial and ethnic differences, as well as inequity in access to dental care by pregnant women, supported on either the social determinants of health, gender, or the social determinants by the epidemiology of lifestyle. Many studies focus on social determinants as external factors that fail to integrate the social reality experienced by pregnant women and the biological conditions they face in both the systemic and oral levels Table 5.
Finally, it is important to point out that in this last thematic area, the studies tend to analyze the relationship of oral diseases and the adverse events during pregnancy. However, the large number of studies on this topic highlights its importance to the dental profession, but it also suggests the predominance of the biological aspects and the fragmented reductionist view within the profession around pregnancy, oral health, and dental care.
In summary, we can say that the studies that focus on pregnancy, oral health, and dental care of pregnant women and its social determinants in this third thematic area center their attention on biological aspects, and to a lesser extent on the representations on oral health, care and self-care practices by both clinicians and pregnant women. Few studies address the dental care provided to pregnant women based on clinical interventions. Regarding the influence of the dynamics of the health care system, very few studies discuss inequality or the biological relationship with the social determinants of health. Very few studies discuss the relationship of oral health and dental care with the inequality faced by pregnant women seen from a comprehensive perspective, based on the influence of social determinants on pregnant women’s oral health.
In epistemological and methodological terms, the studies on the relationship between pregnancy, oral health, dental care, and social determinants are coherent in terms of the topics and paradigms from which research is conducted. In this regard, it should be noted that the works focused on the biological aspects related to the oral and overall changes in pregnant women, the association with adverse events during pregnancy, the interventions aimed at pregnantwomen’scare,andthecoverageofthehealth care system, are all approached from a positivist paradigm, supported in classic epidemiology, applying quantitative techniques, and using statistical analysis as the main tool to approach the analyzed aspects Tables 3, 4 and 5.
When the focus is on the representations of the different parties related to the process of gestation, oral health, and dental care, the studies are conducted with a positivist paradigm based on classic epidemiology, but other studies are conducted from a phenomenological paradigm Table 5. The studies based on the positivist paradigm rely on quantitative techniques, while those with a phenomenological approach usually rely on qualitative techniques.
The research projects aimed at exploring the relationship of biological and social aspects in oral health as well as inequality in pregnant women’s dental care, while scarce, are usually approached from a positivist paradigm, supported in classic epidemiology or based on what Breilh referred to as “causal epidemiologic transition”, which includes the proposition of the Commission on Social Determinants of Health, among other theoretical developments; 9 it should also be noted that within the framework that seeks to understand the biology-society relationship, some research projects are based on critical perspectives, but such studies are really scarce.
When the studies approach the socio-economic aspects of pregnant women, such aspects are incorporated as variables from the classical epidemiological perspective, namely socio-economic stratum, social security coverage, level of education, housing conditions, or access to health care. However, they are treated as variables that are in the same level as biological variables, without considering other perspectives.
When research on this topic is approached from the social determinants perspective, it accepts the social aspects as factors, using multivariate logistic models or multilevel analysis methodologies, more focused on the power of statistics than on recognizing the structural aspects that determine oral health and dental care of pregnant women. The evidence generally show how the income/poverty rate, social capital and its relationship with community organizations affect people’s oral conditions. This approach agrees with the social determinants approach suggested by the Commission of the World Health Organization (WHO), which proposes the existence of three major components in the proposed model: the socio-political context, the structural determinants, and the economic conditions, as well as intermediate factors, differentiating the closest determinants (individual and biological) from the distal ones (at the social level) that can affect oral health and dental care to pregnant women. This approach also has limitations, such as the inability to overcome the causal vision, which neglects the historicity and dynamics of phenomena in a particular social context; in addition, it centers the transformations on governance.
The literature using critical approaches is generally centered on social dialectics, in connection to the relationship between individual and collective levels, discussed by Breilh citing Samaja.9 Few studies with such approach were found, and they generally rely on qualitative techniques or triangulation of mixed techniques.
Consistent with the ontological analysis, the epistemological and methodological section of this study identifies a predominance of the positivist approach and the implementation of quantitative techniques to support the research on oral health, pregnancy, dental care, and social determinants. The studies from critical perspectives are scarce and in general are based on qualitative or mixed techniques.
DISCUSSION
In the present study, the bibliometric analysis on 228 studies allowed us to identify the countries, institutions, authors, authors’ origin, institutional affiliation, and co-authorship networks that research the relationship between oral health and dental care in pregnant women. The findings suggest that there are stronger networks among researchers, universities, and countries located in regions with greater economic development, compared with the networks in less developed areas. This might be explained by the resources that developed countries invest in research on this topic, which could be related to the statements by the Commission on Health Research for Development regarding inequities in health investment globally.10 These findings seem to go in a different direction to the worldwide interest to strengthening the health research capacities in countries with low to medium development. In this sense, Lansang et al point out that the strategies aimed at strengthening researchers aim to encourage advanced training programs like master’s degrees and doctorates, as well as the promotion of participation in bilateral projects of training and development; in the institutional and international context, they recommend conducting plans for human resources training, considering the scientific, technological and developmental need of each country.11 Based on the results of the present study, strategies could be implemented to promote the consolidation of networks of researchers, institutions, and countries working on oral health and dental care provided to pregnant women.
The systematic review showed the predominance of observational cross-sectional studies, as well as very few controlled clinical trials, focused on treatments for periodontal disease in pregnant women, and few systematic reviews and meta-analysis related to pregnancy, oral health, and dental care. Based on these findings, and considering the criteria of evidence-based dentistry, the level of evidence on the subject tends to be low.12 But if the analysis is conducted from innovative theories, it may be observed that there are few investigations related to the topics of interest from phenomenological or critical theories. This could indicate two important aspects to consider: the first aspect is related to the paradigm with which the professional and investigative practice of dentistry is traditionally approached, and, on the other hand, the fact that this is consistent with the training processes in the field of this profession.13
The content analysis showed that, in ontological terms, the studies are focused on three core themes: the biological differences between men and women, the impact of pregnant women’s oral health on the oral and overall health of their children, and the relationship between pregnancy, oral health and its impact on pregnant women’s overall and oral health; however, few studies explore social determinants. In epistemological terms, studies from the positivist perspective are predominant. In methodological terms, research is usually conducted with quantitative approaches. This form of knowledge construction in the field of pregnant women’s oral health promotes a fragmented view of the body and tends to isolate the mouth of the social context. Researchers on this subject usually disseminate knowledge through the publication of scientific articles that have little impact on praxis, since they usually forget that the knowledge reported in this form can be read by other researchers or improve the authors’ ranking within the National System of Science and Technology, but may not have an impact on the social groups that are affected by the aspects they discuss.13
In trying to analyze the investigative process conducted in the present study, it is worth noting the interest to taking full advantage of the scientific literature that was found on the subject, since by integrating bibliometric analysis, systematic review, and content analysis of the retrieved scientific papers, the researchers achieved a comprehensive understanding of both the research processes and the interactions among researchers. This integration also allowed to recognize trends and gaps existing on the topic of pregnancy, oral health, and dental care worldwide, in Latin America and in Colombia.
Considering the potential limitations of this study, it is worth noting the difficulty to obtain the scientific articles in full text; this is the reason why, despite the efforts to produce a comprehensive overview on the topics of interest, this is still a partial view to the phenomenon, since in the systematic review and the content analysis, 131 references were excluded because they were not found in full text, and that may represent a bias in the results presented in this study. However, the bibliometric analysis included 228 publications, allowing the evaluation of the scientific activity and structures of research networks in the field of oral health and dental care of pregnant women.
CONCLUSIONS
Based on the results of this research, the following conclusions can be drawn:
According to the bibliometric study, networks in developed countries are predominant and collaboration in Latin America is weak, so it would be important to strengthen networking in this region. On the other hand, concerning the dynamics of publication over time, an exponential increase in the number of publications related to the studied topics was evident.
In terms of the systematic review, the quality of publications tends to be low, with predominance of descriptive observational and cross-sectional studies.
The content analysis showed predominance of research in the biological fields and health care areas from a positivist perspective. This suggests the need to strengthen the relationship of biological aspects and social aspects in oral health and the dental care provided to pregnant women, considering different epistemological perspectives, in order to achieve a comprehensive view of oral health and promote better dental care for pregnant women.