










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkColombian Journal of Anestesiology
versión impresa ISSN 0120-3347
Rev. colomb. anestesiol. vol.42 no.4 Bogotá oct./dic. 2014
https://doi.org/10.1016/j.rca.2014.07.012
Essay
About simulation and airway safety *
De la simulación a la seguridad en vía aérea
b Anesthesiology & Biostatistics Departments, Erasmus University Medical Centre Rotterdam, The Netherlands
Correspondence to: C/6 10N-142 Hospital Universitario San Jose, Popayan, Colombia. E-mail address: jacalvache@gmail.com
*Please cite this article as: Calvache JA. De la simulación a la seguridad en vía aérea. Rev Colomb Anestesiol. 2014;42:309311.
Received 8 July 2014 - Accepted 18 July 2014
Abstract
Simulation is a valuable tool in health research, medical education and training of health personnel. Research and simulation-based education can focus on technical and nontechnical skills needed to improve patient safety. This article comments on the effect of simulation on several outcomes, including those related to patient-safety during airway management.
Keywords: Airwa y Management Patient Safety Simulation Education Medical Anesthesia.
Resumen
La simulación es una valiosa herramienta en los procesos de investigación, educación médica y entrenamiento del personal de la salud. La investigación y la educación basadas en la simulación pueden enfocarse en las habilidades técnicas y no técnicas necesarias para mejorar la seguridad del paciente. Este artículo de reflexión comenta aspectos relacionados al efecto de la simulación en diversos desenlaces, entre ellos los relacionados con la seguridad en el manejo de la vía aérea.
Palabras clave: Manejo de la vía aérea Seguridad del Paciente Simulacion Educación Médica Anestesia.
There are strong arguments in favor of simulation used for medical education and healthcare staff training. Exposure to real life patients is essential and necessary for the development of clinical skills; however, to accomplish high-quality performance and safety, there may be some risks inherent to the training process itself and the learning curves and skills. These risks can be minimized with the use of simulated models that mimic real life scenarios and its conditions. Consequently, simulation results in a safe environment where researchers and trainees may test and improve their personal and team skills. Furthermore, the use of simulation in research provides considerable benefits. It allows for exploring and describing the attitude of the various healthcare professionals or trainees and for evaluating the various technologies or devices under diverse scenarios and situations, free of risk for actual patients and with fewer ethical implications.
- By definition, simulation “is a technique, not a technology, that reflects or amplifies actual clinical experiences under participative guidance with an interactive approach”.1,2
Simulation-based training may potentially improve safety through a broad range of mechanisms, including: (1) routine training under emergency situations; (2) team training; (3) development of a sound environment to discuss mistakes without fear of recrimination; (4) safety and feasibility evaluation of new procedures; (5) evaluation of skills; (6) evaluation of the use of new devices; (7) human performance assessment; (8) acquisition of skills beyond the clinical context.3
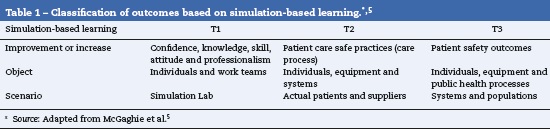
The literature reports the positive impact of simulation on the participant’s knowledge, confidence during the procedures, teamwork performance, and process improvement within the simulation environment (simulated environment or T1). However, presently the data to support that simulationbased interventions resulting in safe outcomes for the individual patient or the population as a whole are scarce (actual patient scenario or T2; population or T3).3,4 McGaghie WC et al.5present a classification of the outcomes to consider under each particular scenario described (Table 1).
In the last few years there has been increasing evidence to support that simulation-based learning really improves the abilities of the staff trained, and the acquisition and retention of new skills.6 However, there are still few studies evaluating the process transition from T1 to T2.7 Crabtree et al. studied the correlation between a simulated scenario of fibrobronchoscopy intubation (T1) and the clinical skills in a real life situation (T2). Although no correlation was identified, the group concluded that the outcome used for the comparison (time to intubation) was not sensitive enough to detect improved performance during the procedure.8 Consequently, the outcomes where a simulation scenario may influence a trainee may be quite different, difficult to assess and quantify, and go beyond the usual outcomes analyzed by researchers. They may be summarized into technical and non-technical “attitudes and skills”, that require complex and validated measurement methods that are not yet widely available.9,10 For instance, some authors consider that attitudes and professionalism should be outcomes considered in the T1 scenarios.3,5 To approach simulation as a mere “transfer” of certain skills (measured for instance as the time to intubation) may be underestimating its value.
In the past issue of the Colombian Journal of Anesthesiology, Uribe et al. present a study that shows the efficacy to secure the airway (tracheal intubation) using the SALT supraglottic device (Supraglottic Airway Laryngopharyngeal tube). Ninety naïve participants were highly competent during their first intubation attempt (90%).11 In addition to their interesting findings and of the feasibility evidenced, this trial carried out under a simulated environment provided the participants with a wide range of abilities, different from those that the researchers studied as outcomes and classified as skills in scenario T1. Most of them were students that faced an intubation situation and their learning experience ranged from where to stand, the respect for a situation when the airway must be secured, to the performance of an expert during the teaching phase. There is no doubt that this experience (recreated within a research environment) was much more valuable for the participants. This is but one of the many advantages of simulation.12
Simulation has been widely used throughout the airway training process and despite the heterogeneity of the populations, the scenarios, and the interventions included in the study, the evidence as a whole supports the use of this tool for most of the outcomes studied.13,14 The benefits of acquiring skills for managing the airway far exceed its limitations. In a recent systematic review, Kennedy et al. document that simulation is superior to non-simulation teaching scenarios, including videos, conferences, or personal study and show the considerable impact of using simulation for learning and developing skills associated to airway management. Nevertheless, the authors fail to report the effect on future behaviors and on the patient’s outcomes (though there is still a shortage of outcome data).15 Some authors defend the hypothesis that the impact on patient outcomes (considered the patient scenario or T2) may be appreciated in this context when structural changes are brought about in the education curricula rather than in individual procedures.15,16
Some research recently published in the Colombian Journal of Anesthesiology shows the boom of the research process within simulation scenarios for the airway and other teachinglearning environments.17,18 Certainly they become a national reference and a broad area for future investigation.
For further information and details about the advantages and disadvantages of simulation, Gómez LM published in the Colombian Journal of Anesthesiology an extensive review on simulation-based training and its implications for teaching and learning.12 Is impact on patient safety is further elaborated in the recent review by Naik VN et al.10
Funding
None.
Conflicts of interest
None.
References
1. Gaba DM. The future vision of simulation in health care. Qual Saf Health Care. 2004;13 Suppl 1:i2-10. [ Links ]
2. Gaba DM, deAnda A. A comprehensive anesthesia simulation environment: Re-creating the operating room for research and training. Anesthesiology. 1988;69:387-94. [ Links ]
3. Griswold S, Ponnuru S, Nishisaki A, Szyld D, Davenport M, Deutsch ES, et al. The emerging role of simulation education to achieve patient safety: Translating deliberate practice and debriefing to save lives. Pediatr Clin North Am. 2012;59:1329-40. [ Links ]
4. Nishisaki A, Keren R, Nadkarni V. Does simulation improve patient safety? Self-efficacy, competence, operational performance, and patient safety. Anesthesiol Clin. 2007;25:225-36. [ Links ]
5. McGaghie WC, Draycott TJ, Dunn WF, Lopez CM, Stefanidis D. Evaluating the impact of simulation on translational patient outcomes. Simul Healthc. 2011;6 Suppl.:S42-7. [ Links ]
6. Lorello GR, Cook DA, Johnson RL, Brydges R. Simulation-based training in anaesthesiology: A systematic review and meta-analysis. Br J Anaesth. 2014;112:231-45. [ Links ]
7. Ross AJ, Kodate N, Anderson JE, Thomas L, Jaye P. Review of simulation studies in anaesthesia journals, 2001-2010: Mapping and content analysis. Br J Anaesth. 2012;109:99-109. [ Links ]
8. Crabtree NA, Chandra DB, Weiss ID, Joo HS, Naik VN. Fibreoptic airway training: Correlation of simulator performance and clinical skill. Can J Anaesth. 2008;55: 100-4. [ Links ]
9. Weinberg ER, Auerbach MA, Shah NB. The use of simulation for pediatric training and assessment. Curr Opin Pediatr. 2009;21:282-7. [ Links ]
10. Naik VN, Brien SE. Review article: Simulation: A means to address and improve patient safety. Can J Anaesth. 2013;60:192-200. [ Links ]
11. Uribe HC, Arenas ID, Acosta JL. Evaluación del tubo laringofaríngeo supraglótico como un dispositivo útil para intubación endotraqueal a ciegas, en personal no experimentado, utilizando maniquíes. Rev Colomb Anestesiol. 2014;42:172-5. [ Links ]
12. Gómez LM. Entrenamiento basado en la simulación, una herramienta de enseñanza y aprendizaje. Rev Colomb Anestesiol. 2004;32:201-8. [ Links ]
13. Lucisano KE, Talbot LA. Simulation training for advanced airway management for anesthesia and other healthcare providers: A systematic review. AANA J. 2012;80:25-31. [ Links ]
14. Kennedy CC, Cannon EK, Warner DO, Cook DA. Advanced airway management simulation training in medical education: A systematic review and meta-analysis. Crit Care Med. 2014;42:169-78. [ Links ]
15. Devitt JH, Kurrek MM, Cohen MM, Cleave-Hogg D. The validity of performance assessments using simulation. Anesthesiology. 2001;95:36-42. [ Links ]
16. Burden AR. Simulation in Anesthesiology. Anesthesiology News. 2011;37. [ Links ]
17. Gomez LM, Calderón M, Sáenz X, Reyes G, Moreno MA, Ramírez LJ, et al. Impacto y beneficio de la simulación clínica en el desarrollo de las competencias psicomotoras en anestesia: un ensayo clínico aleatorio doble ciego. Rev Colomb Anestesiol. 2008;36:93-107. [ Links ]
18. Calvache JA, Sandoval MX, Vargas WA. Fuerza aplicada por el personal de salud sobre un simulador del cartílago cricoides durante la realización de la maniobra de Sellick en la intubación de secuencia rápida. Rev Colomb Anestesiol. 2013;41:261-6. [ Links ]
