











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink
Introduction
Vocology has been first defined as “science and practice of voice habilitation” [1 p5]. Over time, this term has evolved into an umbrella term that combines different disciplines and perspectives related to the human voice. In this context, vocology can be divided [2] into three main branches: basic vocology (laboratory studies such as acoustics, aerodynamics, biomechanics, neurophysiology, imaging, etc.), pedagogical vocology (habilitative and rehabilitative studies for professional voice), and clinical vocology (diagnosis and treatment of voice problems).
Singing pedagogy has proposed many techniques and teachings for the development of the human voice through the use of artistic intuition throughout human history. Singing voice therapy (SVT) [2,3], which has an important role in the vocal habilitation and rehabilitation of singers, is one of the basic tools of pedagogical vocology and the main field of application for safe and sustainable vocal performance throughout professional life.
German classical composer Richard Strauss noted that the human voice is the most beautiful instrument of all, but the most difficult to play [4]. Professional vocal performance has two dimensions: artistic performance and sportive performance. The efficiency and sufficiency of various factors define the quality of these performance modalities. The artistic performance can be defined by time (rhythm), intonation (pitch), sound (blend), and expression (interpretation). These factors are elaborated through vocal training. On the other hand, sportive performance is defined by endurance, speed, agility, timing, focusing, and sustainability. SVT mostly concerns the sportive factors, which define vocal performance ability and sustainability without sacrificing artistic needs. Of course, SVT applications aim to improve performance-based injuries and prevent their recurrence. In this process, singers also learn strategies to enhance their vocal careers.
Habilitation and rehabilitation are similar processes, which are founded upon behavioral treatment and motor learning principles. In habilitation, acquiring and retaining a skilled movement/motor behaviour or task through practice takes place. However, in rehabilitation, since there is a disability, the performer needs to relearn a new set of sensory, motor, or cognitive tasks. In the process of habilitation and rehabilitation of the voices of vocal performers, each of whom is a vocal athlete, the SVT should provide a medical treatment program structured in line with exercise physiology and motor learning principles, taking into account the needs of the individual. SVT needs to be handled from a multidimensional perspective. SVT, though not a singing pedagogy in itself, can include a number of training methods in the protocols.
Vocal performers are the main target audience of pedagogical vocology. The professional vocal performer has been defined as one whose voice is his/her main source of income, who has vocal health concerns during voice use, and whose singing career might temporarily or permanently end in case of dysphonia. After Kaufman and Isaacson [5], a modification for professional voice classification has been proposed by Denizoglu [6], considering the use of performing voice for artistic concerns:
- Based on high-level artistic performance by voice.
- Lose their job or career with a slight voice disorder.
- Soloist opera singers, most well-known singers, some theatre artists.
- Artistic vocal performance on stage (voice quality important).
- Mild to moderate voice disorder affects career and job negatively.
- Most professional choirs, singers, theatre artists.
- Mild-moderate vocal disorder does not affect income, but activity limitations occur that affect quality of life.
- Some singers, students of singing and theatre, amateur choir singers.
- Depends on voice use without artistic concerns.
- Daily job performance is sufficiently impaired because of voice disorder.
- Persuasive voice use (teachers, secretaries, call center workers, receptionists, lawyers, politicians).
- Voice use is required for daily practice, but voice quality is not important
- Physicians, police, most officers, some businessmen.
- Voice does not have a major influence for career.
- Workers, writers, painters, etc.
Understanding human voice begins with understanding movement; the fourth dimension of the anatomy. A vocal exercise is a pre-structured neuromuscular task based on functional anatomy, exercise physiology, principles of physical therapy and sports medicine, principles of motor learning, and behavior change. Sports and Exercise Medicine can be regarded as the “work-based healthcare” [7 p5] for the performance health of individuals who are seriously interested in physical exercise and sports in a multidisciplinary approach. In this sense, two key components of practice take place: habilitation and rehabilitation. Habilitation can be defined as acquiring, preserving, and developing certain (sportive) skills and behavioral adaptation. Rehabilitation is the re-gaining and behavioral transfer of a certain motor skill that has been lost for some reason. This reason may be organic or functional, but the main goal is performance efficiency and sufficiency. These principles can be applied to SVT, which is a major branch of performing arts medicine. Habilitation, in this sense, is the process of enabling, equipping for, and capacitating the vocal performance level by providing solutions for the specific needs of a vocal performer. Rehabilitation, as in sports medicine, aims to return the impaired vocal performance level to a former state or condition through treatment principles.
Exercise processes are determined by four main variables: muscle fiber type, training adaptation, bioenergetics (conversion of energy into action), and age/sex. In the habilitation and rehabilitation processes, it is important for the singer/patient to design education/treatment programs consciously with the perspective of exercise physiology. From the point of view of exercise physiology, the factors that can be effective in the habilitation and rehabilitation processes can be listed as follows [8,9]:
Duration of the effort.
Amount of effort (average and limits of loudness used during exercise).
The rate of daily use of the application requiring maximum skill (singing or stage performance time).
Work-rest ratio (normal life other than professional voice use or professional voice use in second job: day teacher plus night stage performance).
Pre-training (acquiring technical skills, conscious awareness, coping with fatigue).
Genetic factors (anatomical structure, muscle fiber type, motor ability, level of acoustic processing, etc.).
The idiom “voice is muscle” fits with the essential rule of exercise physiology. The vocal exercises are supposed to be structured according to the vector forces and fiber types of the related muscles in a specific motor task. In this sense, the clinician should be aware of the target muscle to be trained by manipulating the speed and type of the vocal exercise. So, regardless of age, training, experience, professional status, and singing style, SVT is for all singers.
Muscle tonus is a main concern in physical therapy. The myofascial system creates a tension network as a continuum that enables the body to move and function in unity [10,11]. Considering the biotensegrity principle, hypotonicity and hypertonicity are elaborated when diagnosis and treatment programs are applied to vocology. Muscle-specific strength and stretch training exercise patterns have similar aims and consequences in vocal training. Various factors and principles in training (overload, progression, rest/recovery, retrogression, plateau, maintenance, reversibility, adaptation, specificity, individualization, warm-up/cool-down) are also considered in programming the vocal exercise structure. As an example, the overload principle requires unaccustomed stress applied regularly. The body detects the pattern of stress (repeated physical activity) and responds by adaptation; strength increases as the body adapts. With the overload -progression- adaptation cycle, several physiological consequences (increased strength, muscular hypertrophy, range of motion, etc.) are obtained, which results with increased efficiency, enhanced ability to perform the activity, higher level of performance, and more resistance to injury and disease.
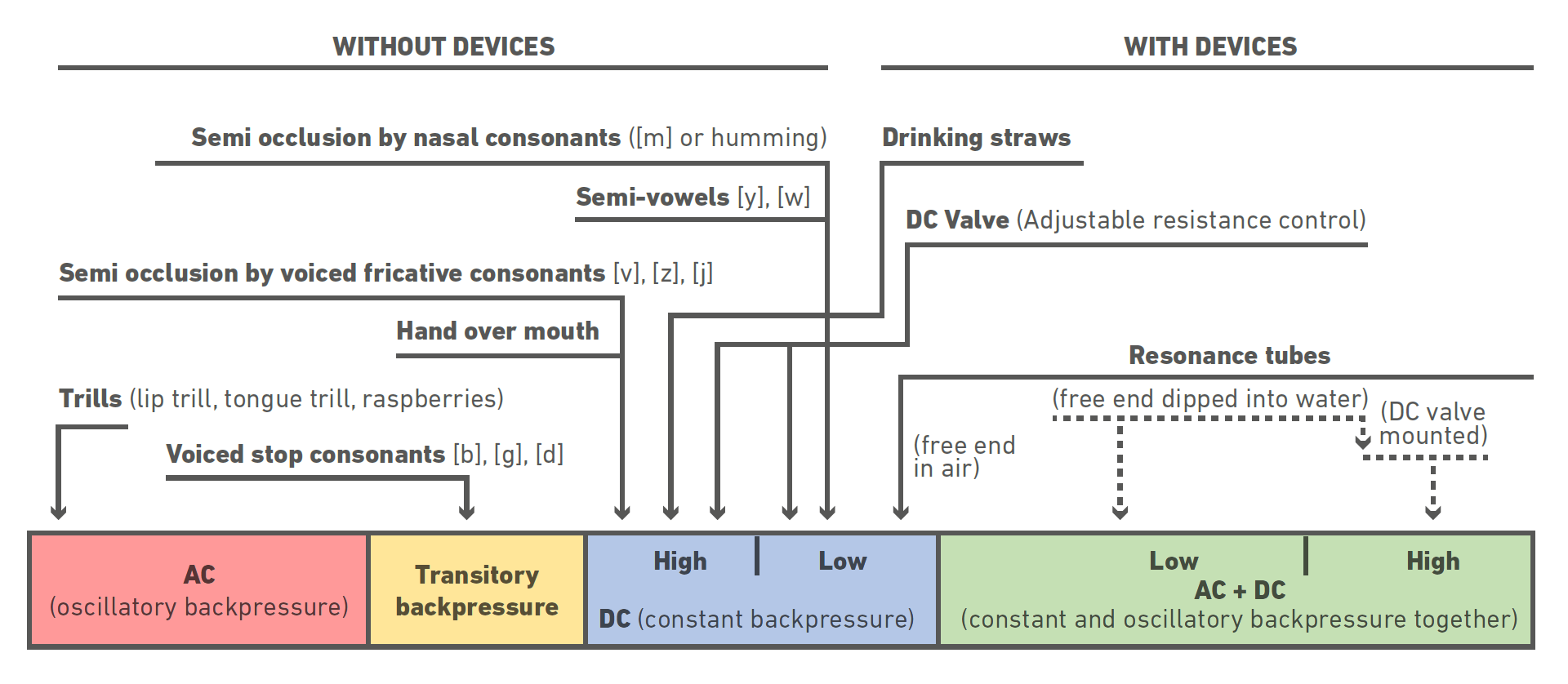
Semi-occluded vocal tract (SOVT) exercises (Figure 1) can be considered as the SVT equivalent of overload in training principles. They are well known in singing pedagogy since they provide vocal economy and safety, muscular strength, and endurance to the performing singer [12]. SOVT exercises may be applied with devices (drinking straws, glass tubes, silicone tubes, masks, or valves) or without devices (trills, various consonants, hand-over-mouth, etc.). The resistance in an SOVT procedure may be continuous or alternate, and the backpressure may be obtained with low-to-high resistance levels [6].
The exercise program using a SOVT procedure can be structured in line with the overloading-progression-adaptation principles. It is important to know which muscle or muscle group the load is intended for. This is the reflection of the specificity factor in the training principles into the SVT program as a muscle-specific voice exercise. Factors such as muscle fiber type, muscle contraction vector, and function form the basic physical-physiological basis for specificity.
Emphasizing the words “form follows function”, adaptation is another important factor of training principles that is reflected in SVT practices. As defined in mechanotransduction, starting from the cellular level, the human organism gives a 'response' to applications and exercises during therapy [13]. Muscles (strength, mass, endurance, dexterity), joints (range of motion and flexibility), mucosa (epithelial thickness, cell type and density, structure of submucosal layers) are the main target tissues to be examined in this tissue response.
Reflection
“Good luck knocks on the door of knowledge”. In medical treatment applications, the clinician is expected to have knowledge about the pathological situation in-depth, and then how and when to apply a certain treatment method. In this context, the question what to do next is to be answered when performing an application and why. This methodological basic knowledge can be treated in three dimensions. The first dimension is the action plan (a multiaxial approach will be presented), which includes what to do during the treatment process. It is possible to evaluate this dimension as the big picture. The second dimension is the equivalent of how the application will be done. Knowing how to perform an exercise means that the clinician knows not only the application procedure, but also the physical and physiological mechanisms and consequences of the application on the cell, tissue, organ, and organism. The second dimension also includes the process of structuring an exercise. The third dimension is related to the timing of the treatment and corresponds to the personalized haute couture scheduling; a periodization schedule is designed according to principles of training.
I. The Multiaxial Approach to Performing Voice
The clinical approach to the professional vocal performer is a teamwork by different disciplines. A multiaxial approach is proposed [14] for evaluation and management of the performing voice (Figure 2).
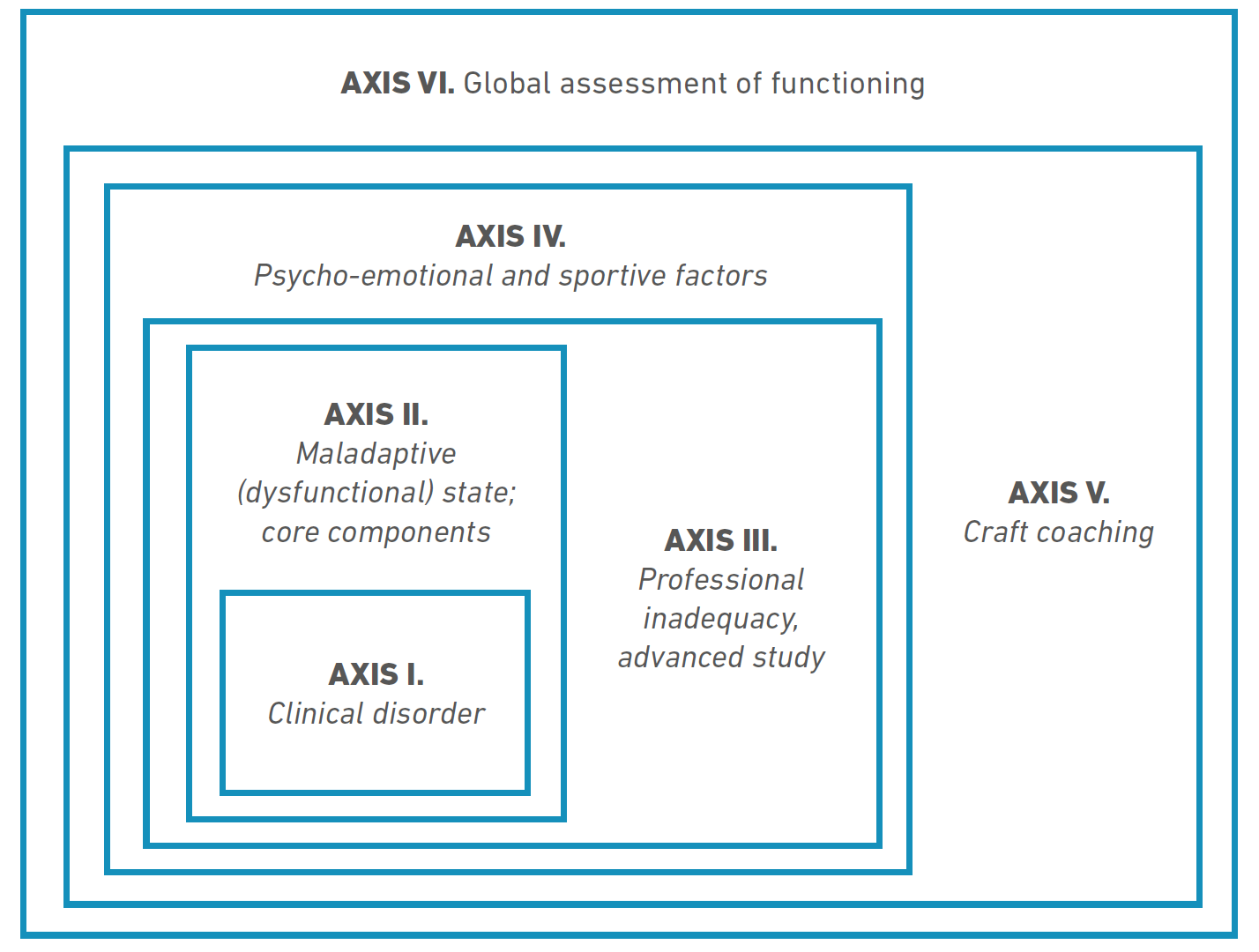
Axis I includes general medical interventions such as organic lesions (inflammation, allergy, laryngopharyngeal reflux, etc.) and functional disabilities. Understanding and analysing the physiology and acoustics of the singing voice [15] is a major concern in the Axis I. Proceeding for the next step may need some time for the Axis I treatment process.
Axis II is a common practice applied to every professional vocal performer referred to the voice clinic. The basic concepts are applied to the subjects. Basic behavioural intervention for a healthy vocal performance starts with cognitive support. The cognitive study includes counseling, explaining, teaching, and instructing about the healthy and unhealthy behaviors, exercise details, and causes and consequences of a given dysfunction. Vocal hygiene (mechanical, chemical trauma, hydration, and humidification) and fitness for performing voice are defined in addition. The vocal exercise in Axis II includes core elements of vocal pedagogy [16], which are primal sound, posture, breathing, and support. Additionally, patterns of speaking voice must also be taken into account and included in therapeutic practices.
Axis III is comprised of elaborative strategies to maintain and improve the stage performance. Advanced vocal performance strategies and practice for a high-level skill acquisition exist in the third axis. Advanced source and filter applications such as refinements in primal sound, vocal muscle development, vocal focusing and registering, case-specific support (appoggio) strategies, and advanced cognitive study are the main factors of Axis III.
Axis IV is concerned with psycho-emotional and sportive issues that affect performance quality. Starting from the general psycho-emotional condition, relaxation, motivation, and coping with musical performance anxiety (MPA) are components of the psycho-emotional approach. On the other hand, the sportive conditioning and rehearsal strategies (periodization) are concerned in this axis.
Craft coaching is applied in the Axis V. Periodization strategies are primarily elaborated in this axis. Singing as a craft must be scheduled consciously and in a scientific-based fashion, concerning performance quality and sustainability. The stage environment is a complicated medium, and every parameter may affect the singer’s performance quality. On-site technical support (amplification, stage monitor speakers, optimum sound-check, microphone technique, etc.), room acoustics, climate (humidity, temperature), and pollution must be considered in the stage environment. In addition, costume, make-up, and stage team are important factors which may influence vocal performance. Performance schedule (lodging and boarding, diet) must be planned consciously. The decision for optimum repertoire according to the genre, voice type, and individual preferences is mandatory. In this process, the ‘Showbiz’ part, in addition to vocal expression, is to be considered. Body language, expressions, handling the audience, and using the stage effectively are separately studied. On-site follow-up is a part of this axis, the clinician is supposed to support the vocal performer backstage as well.
Axis VI is the “global assessment of functioning”, which is a scale that rates the social, occupational, physical, and mental functioning of the professional vocal performer. In this axis, the clinician needs to determine how well the singer adapts and performs on stage. If there is a polyp that adds some roughness to the voice during singing, and if this becomes a characteristic color for the singer, then excision of this polyp may end the career. A careful follow-up is needed through performance.
II. Methodology and Methods in SVT
In addition to sports medicine and physical therapy and rehabilitation principles, motor learning data provides valuable information to the clinician for the programming and structuring of vocal exercises and form the main rationale of the treatment methodology and exercise schedule. Influences on motor learning (pre-practice, practice, and feedback) [17] are to be taken into account in SVT methodology.
Pre-practice considerations include factors about the patients’ understanding of the purpose of the exercise. The practice mainly indicates the SVT exercises, and several factors are considered in designing the exercise structure: pattern, type, target complexity, specificity, schedule, variability, timing, amount, repetition, and mental practice. Feedback is the second important tool in motor learning after exercise. Feedback is the information about the consequences of action (movement) and it promotes problem-solving, self-monitoring, and self-correction, which makes it a powerful determinant of learning. Feedback design through SVT also has several factors: type (intrinsic, augmented), application (positive, negative), timing (immediate, delayed, concurrent, terminal), frequency (continuous, intermittent, faded, bandwidth), specificity (general, specific), and process (knowledge of performance, knowledge of results).
SVT is a complex dynamic process that must be structured in an haute couture fashion, which can be programmed according to clinician and patient.
Clinician-based programming
The “how to” issue in SVT includes clinician and patient-based programming and application of the techniques. Knowing how to perform a particular exercise, as well as tailoring the treatment program, is the basis for SVT process. Clinician-based programming may be explained with a four-level staging that may help a better understanding of the interactions of the components of human vocal instrument involved in the habilitative/rehabilitative processes:
Stage I (Preset)
After vocological assessment and diagnostic process, the patient needs to be prepared cognitively and structurally (posture, breath), although no vocal exercises are included in the first stage.
Stage II (Exploration)
Finding the sound of the target vocal behavior is simply described as primal sound. Finding this vocal pattern prepares the patient for the vocal exercise and muscular development, combining the cognitive and associative phases of motor learning.
Stage III (Development)
Developing the target voice needs practice. The muscles of voice system now memorize a new pattern (vocal technique). Vocal hygiene counseling and core elements of vocal pedagogy (primal sound, posture, and breathing-support) are mandatory for a safe vocal development. Source and filter applications are generally applied simultaneously: the clinician should have a multidimensional way of thinking by blending acoustics, aerodynamics, biomechanics, and physioanatomy, as well as arts, for each and every individual.
Patient-based Programming
Patient-based programming has three phases (cognitive, associative, autonomous) that have been defined [18] in motor learning, which also enables the clinician to monitor the patient throughout the SVT process. These phases are not strictly separated; they are almost always blended and can exist at the same time.
Cognitive Phase
It refers to the information regarding the nature of the problem (i.e., improper glottal closure), why and how it is supposed to be solved, what to do and how to do the task (vocal exercise) safely and correctly and the ultimate goal or purpose. They learn what it feels like to phonate correctly and often. Their attention needs a lot of concentration in this phase, especially because phonation is mainly monitored by auditory feedback. Distractions should be minimized during voice therapy session and proper feedback should be given until they are able to monitor their own sound of voice. Visual feedback is a powerful one and patient’s own vocal folds during voicing may be shown for this purpose.
Associative Phase
It requires working on fine-tuning (glottal attack and glottal damping, correct registration, etc.), concentrating on producing the most consistent and efficient movements (primal sound). Performing the movements or task under different conditions forces the patient to use problem solving when errors do occur. Less feedback is required during this phase.
Autonomous Phase
It involves less and less attention from the patient, so that they can do other tasks at the same time (singing with the new muscle technique). They should be able to easily adapt to variations in task (glissando/portamento/staccato, among others) demands. Unless symptoms occur, the clinician has very little feedback demands during this phase of therapy. The patient is likely ready for returning to stage.
SVT Methods and Applications
SVT shares and combines similar procedures and applications with voice therapy and vocal training methods and techniques. Regardless of the genre, type or style of the singer, there are common practices to some extent. This situation is similar to the application of closed to exercises done by athletes from different sports (football, basketball, tennis, etc.) to a certain extent. After the basic applications, the requirements of the singer regarding performance type and technique are then studied. Singing voice therapy methods can be classified [14] according to application procedures: (1) counseling, explaining, teaching, instructing, (2) vocal hygiene, (3) core elements of vocal pedagogy, (4) advanced applications for voice source, (5) advanced vocal tract applications, (6) relaxation and coping with musical performance anxiety, and (7) management of environmental factors.
Counseling
Explaining, teaching, instructing, in addition to basic knowledge about the phonatory system, determining the problem, and the etiopathogenesis are important aspects for the patient to proceed. The main goal is to create a picture of self-voice (mirroring) and increase the vocal awareness. Counseling also includes knowledge about the whole SVT process (vocal hygiene precautions, vocal fitness program, relaxation, and coping with musical performance anxiety), as well as environmental factors.
Vocal Hygiene
Vocal hygiene factors are mechanical trauma, chemical trauma, and dryness of the vibrating mucosa. Increased amount of glottal impact such as yelling, vocal overuse, and chronic cough are defined as vocal abuse. In vocal misuse, an increased impact on vocal fold mucosa is focused on a limited area (mostly midmembranous region) and also creates a mechanical trauma. Chemical trauma may be the result of inhalatory irritants (tobacco, marijuana, etc.) or laryngopharyngeal (gastric acid and enzyme) reflux. Hydration and humidification are shown to be important in vibratory dynamics and both adequate water consumption and the breathing of humid air affect vocal fold mucosal moisture.
Core Elements of Vocal Pedagogy
Primal sound, posture, and breathing are defined as the core elements of vocal training [16], and three basic factors while creating a vocal instrument. They can be structured separately and combined in advance, which provides a modular manipulation when a problem exists in the professional life. The primal sound is like a vegetative function of the body, which is the safest way to react. In this sense it can be achieved by grunting, sobbing, moaning, crying sighing, yawning, humming, coughing, laughing, trilling (lips, tongue, razz). Oren Brown’s statement is descriptive: “Primal sound is the key for the artist in you to communicate as a singer and for the thinker in you to reach the audience as a speaker. Primal sound is essential for your vocal health as a singer or speaker” [19] Posture and breathing can be treated in a combined way, because the effort for intrathoracic pressure is formed mainly by posture muscles. In classical singing pedagogy, noble posture is a key concept, which includes high sternum, relaxed shoulders, and active spine. The effort vector is proposed to be felt downwards with a low breath. The main goal is to keep extrinsic laryngeal muscles free from inhalation and forced expiration in order to create a balance between breathing and phonation [20].
Advanced Applications for Voice Source
Management of the vocal vibration pattern starts with glottal attack and damping practice. A balanced attack and damping, instead of hard or breathy glottal onset/offset patterns, is acquired before the muscular development tasks. Ventricular fold control plays an important role in unnecessary effort during phonation. Vocal focusing has a specific place in vocal pedagogy. Different glottic closure patterns create different acoustic spectral structures. When the energy distribution in the spectrum changes, the region that resonates this acoustic energy changes. This technique is a traditional training tool used by singing teachers. As well, the kinesthetic feeling may be used to manipulate glottic closure patterns. The concept of “singing into the mask” is a well-known vocal placement exercise related to this feedback [14].
Vocal muscle development exercises may be defined as registration when applied in a specific schedule. In this sense, different vocal tasks (sostenuto, glissando, staccato, etc.) can be used to develop intended vocal muscle(s) and muscle fiber types. Developing and blending the registers can be achieved with conscious, muscle-specific training patterns. For example, exercises with naïve falsetto may be used to develop cricothyroid muscle, and chest register is studied for thyroarytenoid muscle development. Type of muscle contraction (isotonic, isometric) is also a factor in exercise pattern. Pitch-based tonal exercises and loudness-based exercises may be combined with linguistic load and articulatory patterns in advance.
Advanced Vocal Tract Applications
Vertical larynx position is a major interest, environmental factors classical singing pedagogy. A comfortable low laryngeal posture is proposed in opera genre, while the high larynx may be a component of belting [21]. The vertical positioning not only affects the filter function of the vocal tract (length and shape), but also changes the biomechanical properties of the vocal folds (mass and stiffness) [22-25]. Of course, the glottic registration mechanisms are supposed to be combined with vocal tract procedures in order to create a better vocal technique.
Resonation strategies and formant tuning have an important role in SVT applications. Specifically, they relate to how the vocal tract resonates the harmonics that are produced by the vocal folds. The term resonation strategy relates to the process of making specific vocal tract reshaping choices, in order to compose a particular spectral structure created by formant/harmonic relationships, thereby creating different timbres. These strategies are essential for determining how to create stability especially in high/low pitches, modify vowels, and sing in different styles. Reshaping the resonator spaces in the vocal tract results in filter dynamics and acoustical changes. Various maneuvers (lowering the larynx, lip rounding/retracting, tongue forwarding, epilaryngeal tube formation, etc.) can be used to adjust the acoustic effects. Artificial elongation of the vocal tract with resonance tubes [26,27] may also provide advantages during the practice of vocal exercises.
Relaxation and Coping with Musical Performance Anxiety
Stage performance is a multifactorial activity that includes the psycho-emotional state. Musical performance anxiety is a spectrum between excitement and phobia [28]. Management starts with understanding the etiology. Perfectionist evaluation is the most prominent cause whereas fear about making a mistake (words, intonation), unceasing self-judging, rehearsing and memorizing obsessions, difficulty of digesting critics, and sticking in the past can be other causes. Management includes before, during, and after performance strategies [29]. Before a performance, proper rehearsal is the best way to cope with MPA. Relaxation, memorizing methods, proper evaluation are other options with professional help and vocal coaching. During the performance, living for the moment and enjoying are crucial factors in management of MPA on stage. After the performance, a realistic evaluation of expectations and critics will help for the MPA management for the future [30].
Management of Environmental Factors
A professional vocal performance is influenced by various environmental (non-vocal) factors. Although context of professional vocal coaching may vary widely, beyond voice-related activities (vocal rehearsal, style, repertoire, etc.), there are other different non-voice related performance factors. Management and orienting the environmental factors such as acoustics (room acoustics, electronic amplification, etc.), air-conditioning (temperature, humidity, particle density, etc.), and emotional factors (audience, stage partners, etc.) are crucial. Tour-concert program (travel, lodging and boarding, stage and backstage conditions), dietary conditions, sleeping arrangements, and several other factors influencing vocal performance should be considered in the development of an SVT program.
III. Periodization in SVT
A sustainable stage performance depends on the training strategy based on physiological approaches. Periodization is being used in sports medicine and implies the systematic planning of training and exercise [31]. It can be transferred into vocological practice and defined as systematic planning of vocal habilitation due to performance schedule (Figure 3). Periodization process can be evaluated in three cycles: macrocycle (the yearly performance program), mesocycle (rehearsal for a specific performance or concert tour) and microcycle (the day of performance).
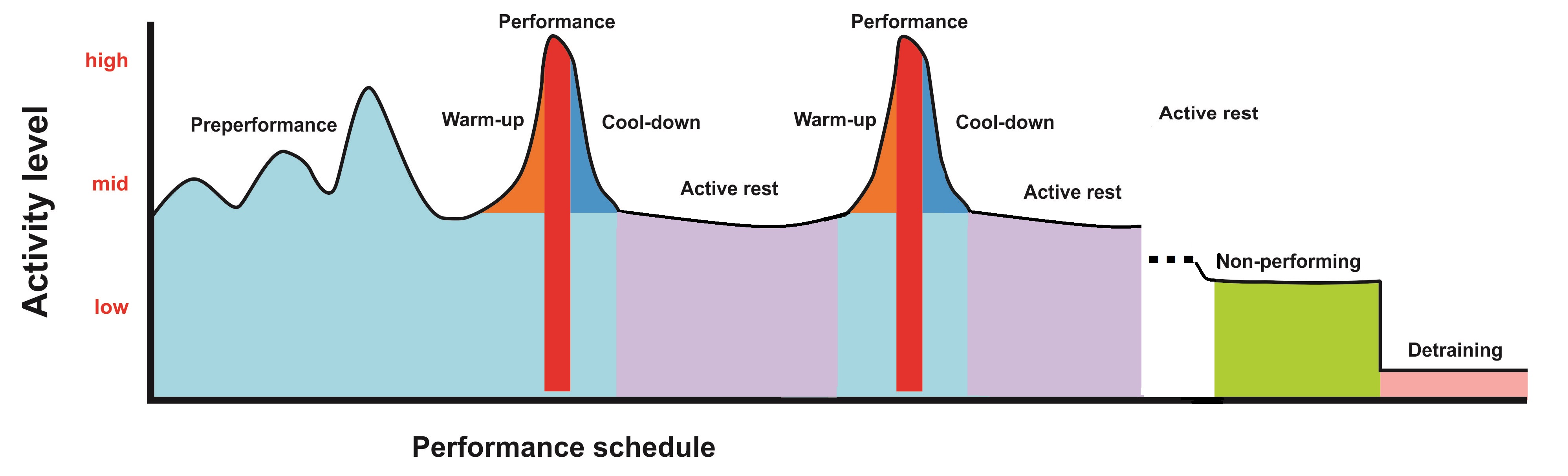
The preperformance period includes the rehearsal study that may last weeks to months. Vocal skill and endurance (muscle development) exercises take place in this period. Peri-performance period is the day of performance that starts from the morning and includes vocal warm-up and cool-down procedures. The transition (active rest) period starts from next morning until the next performance day. It is a period after a performance to let tissues recover and keep the level of preperformance state.
The maintenance (non-performing) period is a good example for pandemics. The active performances are cancelled, but the activities of the vocal athletes must be maintained. Detraining is a partial or complete loss of training-induced adaptations as a result of a training reduction or cessation, which needs a specific program before the active stage performance.
Conclusion
The clinical approach to professional voice is a team effort that includes various factors and many disciplines. Diagnosis is the first step of treatment and cannot be separated from treatment. The clinician should internalize the basic mechanisms of the exercises he/she chooses and should be able to accurately demonstrate them. The source of practical information is primarily vocal pedagogy; in addition, the principles of sport-exercise medicine, physical therapy and rehabilitation, behavioral therapy, and motor learning should be included in the process of structuring and applying the exercises. Practices should be reproducible and based on cause-effect relationships, in line with the principles of physics, physioanatomy, and physiopathology. They should be free from random and rote-based expectations.
It is not possible to examine this extremely broad subject in all its aspects and to fit it within the confines of a single article. In this respect, it is important for the reader to further investigate details (as briefly discussed above) in order to enrich their clinical practices.

