











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink
Introduction
The history of neuroauriculotherapy (also known as auriculotherapy, and referred to as NAT in this article), a recognised branch of medicine [1], is very old. Centuries before the common era, Hippocrates, the ancient Jews, and many Chinese practitioners used to needle the auricle to treat diseases ranging from lower back pain to headache [2]. At that time, auriculotherapy was something mystical. Despite the reference to Chinese practitioners, NAT now has nothing to do with Chinese auricular acupuncture; it does not lay its foundations on traditional Chinese medicine but on neurophysiology, so it can be defined as an applied neurophysiology. In fact, only in the early 1960s the French doctor Paul Nogier started a scientific study of the links between the auricle and the brain. He observed that many of his patients had a thermic cauterization at the intersection between the upright branch and the lower root of the navicular dimple (an area that we now know corresponds to the muscles innervated by L5) [2]. Patients reported having had a case of sciatica that was cured thanks to a cauterization made at this point. Nogier gathered the most important French neurophysiologists to conduct scholarly studies giving life to the GLEM (Groupe Lyonnais d’Études Médicales) and, after few years, they discovered that the auricle resembles a fetus with the head positioned downward [3].
Early in the 21st century (2002), David Alimi, a French neurophysiologist from Paris, used Functional Magnetic Resonance (fMRI) [4,5] to demonstrate the neurophysiological connection between the auricle and the contralateral brain [2]. Thanks to Alimi’s work, NAT is now accepted by the World Health Organization (1987). It is a method that can be used only by a physician because it requires appropriate medical diagnosis. Based on studies of neuro-dissection and neuroimaging using tools such as fMRI, he developed a method for mapping the surface of the auricle that identifies every point, localizing each point with a letter and a number. This map (proposed, and adopted by World Health Organization in 2010) replaced the older inaccurate empirical charts.
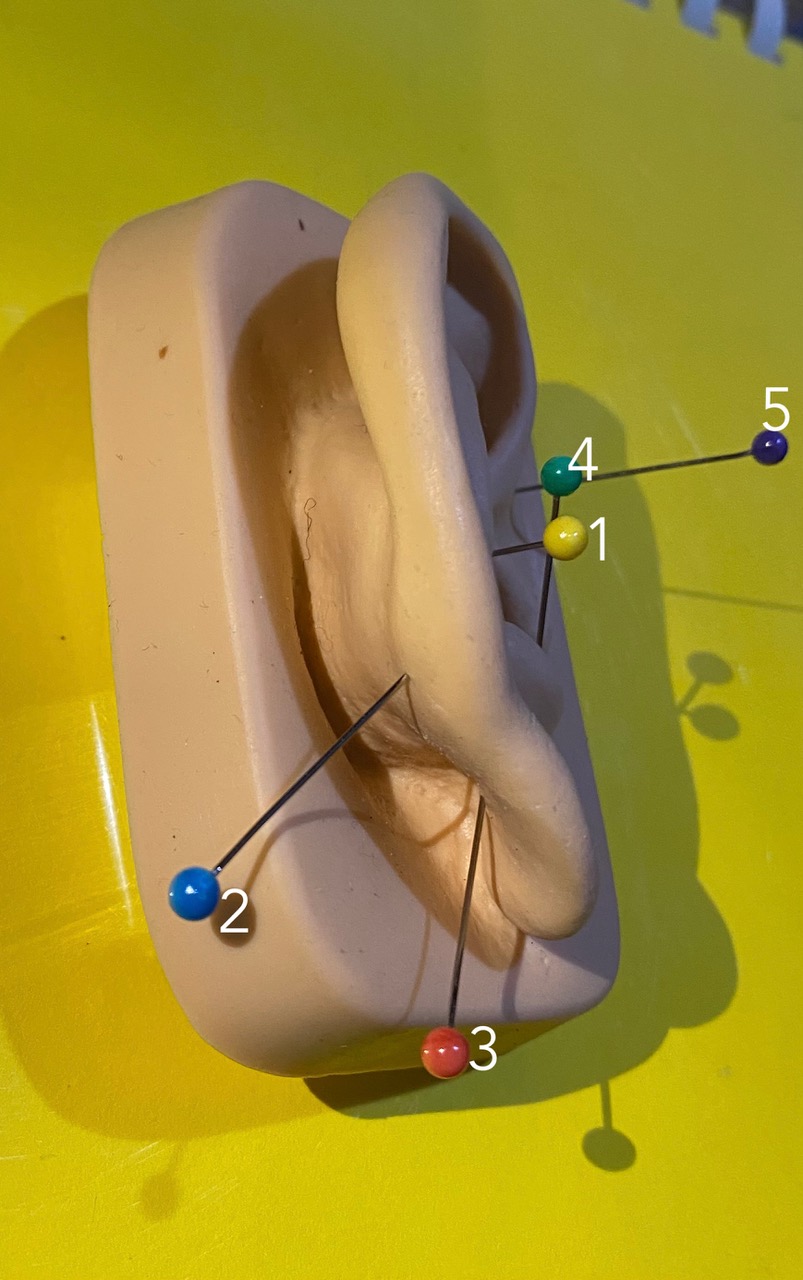
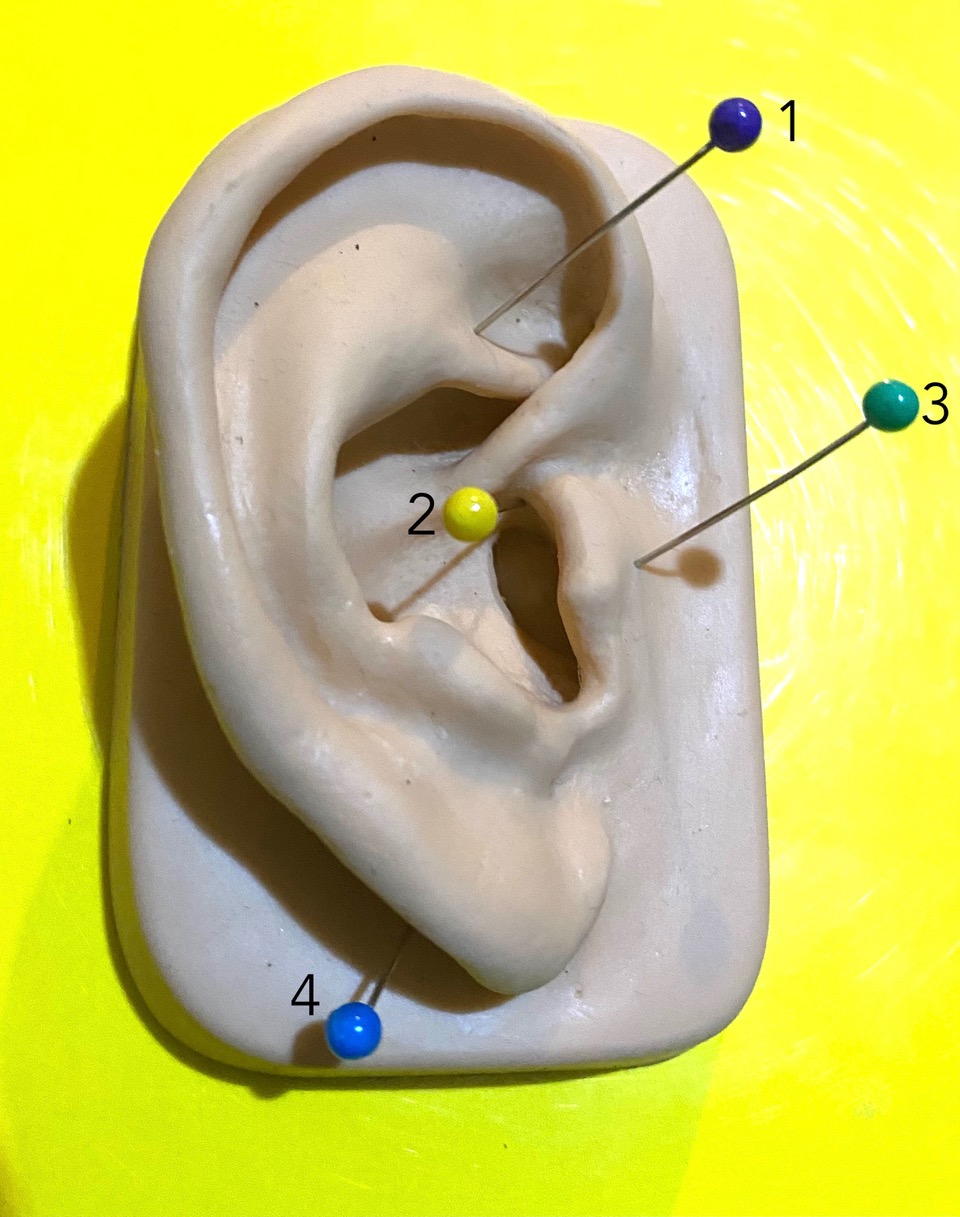
Alimi’s map establishes an epicenter in the middle of corpus callosum from which he plotted a set of Cartisian marks comprising 20 radial lines (numbered from 1 to 20, separated by a 9° angle), intersecting with 11 semicircular lines (identified by A to K) [5]. According to studies of neuro-dissection, Alimi noted that the same organization exists in the brain [2,6]: if we draw 20 radial lines originating from the center of the corpus callosum, the same configuration will be obtained. On the lateral face of the auricle, 196 sensorial-sensitive points are present, while on the medial face, 84 motor and visceral areas are represented. Special symbols are used to locate a point above or below a relief or medial face. On the map, the points are represented by a color that identifies the embryological origin: ectodermic points in blue, mesodermal in red, and those of endodermic origin in green [7].
Our central nervous system works using maps [2]; it creates somatotopic maps at each neural level (metameric, trunk, thalamus, cerebellum, cortical, base ganglia, etc.).
The maps begin to form during the growth of the fetus and are under the control of specific genes [2]. Every mammalian possesses specific maps [2]. Somatotopiae (the somatotopic sensory areas) develop with cerebral maturation, growing with each individual’s life experiences. At birth, certain points are already well-formed and highly receptive because there are no parasitic circuits, memorial circuits, etc.; however, not all points are well formed: some will be formed during early life in tandem with the myelination of the brain.
After conception, the morula will come from the zygote, then the blastula and, subsequently, the blastocyst. The blastocyst presents a thickening called "embryo node", which will differentiate into three leaflets (ectoderm, mesoderm, and endoderm).
In the auricle, as a memory of these embryological stages, some vestige points can be identified [2]. These points, called Master Points, are very powerful and have various functions. They not only affect the tissues related to them but also the psychic sphere. They are also called "Omega Points": Omega (the ectodermal point), Omega 1 (the endodermic point), and Omega 2 (the mesodermal point), respectively.
In neuroauriculotherapy, the ear is used to give to the brain logical orders based on the diagnosis and on the laws of neurophysiology [2]. The analogy between the auricle and the corresponding brain areas is extremely precise (as demonstrated in fMRI) and reproduces clearly the sensory, motor, and visceral homunculus present at the cortical level.
The auricle really is a "keyboard" connected to the "central computer", through which it is possible to type precise strategies and orders that the brain will accept, so long as they are logical and follow the "language", the "alphabet" of the brain, that is, neurophysiology.
Therefore, auriculotherapy is really an applied neurophysiology [2], and we can use the auricle to send orders to the brain in accordance with a correct diagnosis and the laws of neurophysiology.
NAT speeds up results compared to the traditional approach, because it forces the brain to return to the best homeostatic configuration from prior to the disease. In practice, it is as if a sort of system reset is performed. In this sense, NAT integrates with other techniques and speeds up results.
Voice is a complex activity under the control of our brain. We can talk or sing, but this activity must be regulated by epiphysis cerebri [8]. Vocal tract diseases can be dysfunctional or organic. Our experience suggests that we can use neuroauriculotherapy in both situations. For instance, we can activate the filters of pain, enhance the activity of the parasympathetic or sympathetic nervous system and modulate the autonomic balance, enhance the production of cortisol, order the rhythm of speech, coordinate the activity of the two hemispheres in control of voice using the corpus callosum (over 298 million fibres that connect the two hemispheres), reduce anxiety, and so on [8].
In this article, we want to discuss in more detail some of these applications, in order to highlight the potential usefulness of neuroauriculotherapy in voice science and phoniatrics.
The methods used to write this article were structured in two main phases: 1) phase 1 was based on an in-depth analysis of the literature on this subject, followed by a comparison between its content and what we have learned observing some common voice disorders in our professional practice; 2) phase 2 consisted of the creation of therapeutic protocols for some patients who were suffering from the voice disorders previously examined and compared with the literature on NAT. Most of these protocols were originally suggested to us by David Alimi (see references) and they have subsequently been reworked and informally tested by us. The application of these protocols has given consistent and appreciable results, relevant enough to suggest sharing the protocols with the scientific community. However, the analysis of the process has not been formally structured; therefore, we should consider this article as a discussion rather than a research article.
Reflection
The brain follows fundamental laws of neurophysiology [2], which are constantly repeated and cannot be ignored. For this reason, it has some "obsessions" that it seeks to satisfy. The first is that each neuron must connect with another through synapses within 1 millisecond. If it does not, the neuron goes into apoptosis -a natural process of rehash and reorganization that allows the system to maintain good efficiency, avoiding useless and malfunctioning connections- and it is eliminated [2]. The second is to ensure the homeostasis of time, place, and space. In Greek, Homeostasis means perfect balance. There may be a disruption of the general or local homeostasis. In this sense, pain is a tool that the brain uses to know if there is a perturbation of homeostasis in an area [2]. For example, a pharyngeal pain means that there is a pharyngeal problem to be remedied. The third is to follow the law of entropy [2], which is a progressive and inevitable aging of the structures until their end.
Our central nervous system works using maps [2]; at each neural level (metameric, trunk, thalamus, cerebellum, cortical, base ganglia, etc.), it creates somatotopic maps. In the same metameric level, the peripheral information of skin, muscles, and viscera arrive and converge; this assumption coincides with Kahler's first law, called "law of the convergence" [2]. Each metameric level is then connected to another three higher levels and seven lower metameres; the information that comes to the metameric level "resounds" in the higher and lower planes. Moreover, there is an interneuron that correlates the afference coming from viscera with the sensitive one coming from the spine or the periphery [2]. This phenomenon of "metameric resonance" can explain, for example, how a colon problem can cause a pain, or increase a block, in the lumbar spine, and vice versa, as a primary problem in the spine may resonate with a visceral organ. The maps are then formed from the most peripheral metameric levels by implementing the information as you ascend to the trunk. The map of the head and, in part, of the neck is provided by the cranial nerves [2]: primarily the trigeminal with its three branches (V1-V2-V3 carrying sensory and, partly, motor information), facial (motor and sensory), glossopharyngeal and vagal, and superficial cervical plexus. It happens as if, at the level of the trigeminal nucleus and the reticular substance, there were an exchange of reciprocal information leading to the constitution, in both these structures, of the complete somatotopic map represented by the inverted homunculus of Penfield. This same map is then conveyed by the nerves that serve the ear (trigeminal) at the auricle level [9]; thus, in the auricle, the characteristic of the homunculus with the head downward is maintained. The somatotopy with the inverted homunculus (present at the level of the reticular formation) is then transported to the thalamus where a horizontal homunculus is formed and from here, through the corona radiata (radiating crown), it is conveyed to the parietal cortex exactly at the level of the Gyrus postcentralis, that is, areas 3a -3b, 1 and 2 of Brodmann. This defines the somatosensory area S1 [10]. At the level of the upper lip of Silvio's Scissura, there is another somatotopia (the somatotopic sensory area) called S2 [10].
The aim of our brain is to maintain the best possible homeostasis of time, place and space for our organism, both in general and in specific areas [2]. To obtain this purpose the brain receives plenty of information, both external and internal, thanks to proprioceptive and exteroceptive sensors. The information makes precise maps at every level (metameric levels, trunk, thalamus and so on); the last maps, at highest level, are in the cortex. Therefore, there are sensory, motor, and visceral maps. The brain uses the information it receives to adopt the best strategy for every situation. Sometimes the control is direct, while other times it is guided by the autonomic system, so that there is a neurovegetative balance in perfect equilibrium between the orthosympathetic and parasympathetic systems [10]. Every response or activity of our brain in the maintenance of correct homeostasis is under the control of the limbic system.
In case of a problem in a specific area, using the auricle as a keyboard, in accordance with a correct diagnosis and sound knowledge of the laws of neuroscience, we can send a request to the brain, and, if this is right, the brain goes back to its memorial maps to reach the best possible homeostasis that existed before the problem arose. In fact, the brain uses Kahler’s third law [2] to go back to the best homeostatic configuration from before the problem, so the brain resets the system. It would take from one to three requests, depending on how old the problem is, to make this reset [2]. So auriculo-strategy alerts the brain to the problem and other therapies, drugs, rehabilitation and so on go better because the brain knows what to do.
By definition, in order to be more effective, the NAT point must be temporarily deactivated, that is to say, temporarily destroyed [2]. This will result in transient interruption of the information from the ear to the cortex, which will force the brain into a massive response to our requests. Obviously, the reaction is greater when clinicians have a precise diagnosis that allows them to formulate a sensible and calibrated strategy on precise neurophysiological bases. Strategies that do not follow these rules are rejected or, at least, are less effective [2].
To go back to the memories, it is generally suggested [2] to perform an "induction" treatment: at first, three therapies spaced about 20-30 days apart; then, longer intervals, depending on the problem. If the disease is chronic, treatment should be performed over a period of 2, 3 or 4 months, depending on the circumstances. If there is a degenerative pathology (e.g., Parkinson's) the treatment must be repeated every 2-3 months. There are no restrictions on the type of patient. The only non-responders for their pathology are cancer patients, for whom NAT can act on pain and on the complications of radio and chemotherapy, but not on the control of the disease. Some points, such as the point of synthesis (which generally accelerates protein synthesis), should be avoided in patients who have had an oncological pathology in the last 10 years, or who suffer from autoimmune or psychotic pathologies. There are some specific points that can accelerate labor during pregnancy. NAT can be applied to all ages with some precautions in the pediatric age, especially in the neonatal and perinatal age, as due to incomplete cerebral myelination the brain maps are not yet perfectly formed.
Needles can be:
Extemporaneous: they have copper or steel handles and are similar to those of acupuncture.
Semi permanent Needle (SPN): these needles are about 1 mm in diameter and are inserted at the point through an applicator to stay infused to the skin for a depth of about 2 mm.
Made of ice (Cryogenic Needle): we utilize a liquid nitrogen oxide (N2O at a temperature of -89 ° C) that is emitted out from a glass tube (in which a 60 μ channel was made with the laser). The jet runs at a speed of 40 meters per second and penetrates for a diameter of 1 to 10 mm, with a power of 18 to 22 watts (1000-1200 KOhms). This results in immediate freezing at -40°.
Made of glass (palpation chopsticks): They can be useful in Pediatrics, especially if you want to solicit but not inactivate the point.
We can find the activated point in the ear auricle by evaluating the electrical resistance in the area of the auricle where we believe there is the problem and noticing a decreased resistance compared to the surrounding areas [2]; even applying a palpeur (i.e., a tool that provides a constant pressure of 100, 150 or more grams). If the point is perturbed, there will be pain when applying the palpeur.
Considering the auricle as a keyboard, there are many possible application of NAT across several medical fields. For example, NAT is effective in treating all kinds of pain, reducing anxiety, and it works in both acute and chronic diseases [8].
To avoid damage from NAT, a few rules must be followed:
The first is to ensure a correct diagnosis;
the method is not effective in severe cachexia and psychoses where the control of the general homeostasis is completely lost;
it should be remembered that the "Synthesis Point" (that gives an acceleration of protein synthesis) should not be used in patients who have undergone an oncological disease in the last ten years [2] or who suffer from an autoimmune disease [2];
in pregnancy some points are prohibited [2];
NAT should be carried out with accurate asepsis (with denatured alcohol) of the posterior auricle (especially at the auriculotemporal sulcus where staphylococcus stays easily).
The strategy must be characterized by neurophysiological consistency, so the succession of points, precision in locating them, and the choice of which side to start on are crucial factors [2]. For this reason, it is first necessary to establish the patient's laterality. Everything is lateralized [2]. We have an eye-director and an eye-of-guard (the first plays a major role in distinct vision, the second in peripheral vision) [11], as well as for the ear and for the limbs [2]. Such physiological and functional lateralities must be fully respected [2]. There are many tests to identify the dominant side of the subject [2]: the most common is the “applause test”; another one is folding the arms, etc. [12].
There are, in fact, pathologies linked to an externally imposed change to the physiological laterality of the subject; possible examples of such pathologies could be dyslexia, night enuresis, etc. [2].
For example, if there is an edema of both the vocal folds but more pronounced in the right one, the treatment starts on this side. If the problem has an affective or emotional significance, it is preferred to start from the non-dominant side, the emotional hemisphere (this would be the left hemisphere in a right-handed person, linked to the left ear), and then move to the opposite side [8].
As our discussion is oriented toward voice medicine and to performing arts medicine, we would like to present a few examples of voice problems to describe the use of NAT in these medical areas.
As described in the Introduction, our experience proves that we can use neuroauriculotherapy in both dysfunctional and organic voice disorders and diseases. NAT helps in every single pathology if you have a precise diagnosis; by typing on the auricular keyboard, you can apply the most appropriate strategy to cause a return to the best homeostatic configuration from prior to the pathology.
Laryngitis
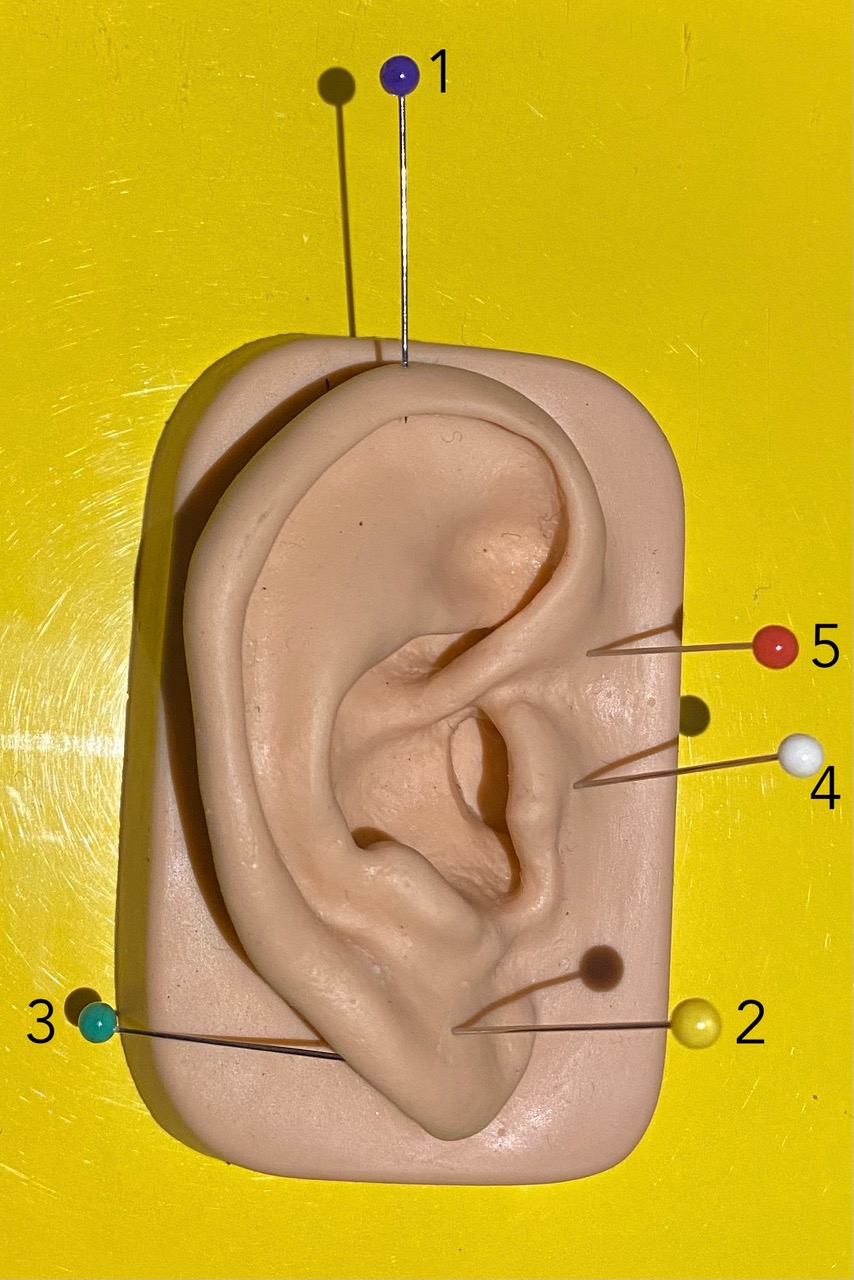
For example, in Photo A we see the specific strategy that we can use in laryngitis, an organic inflammation:
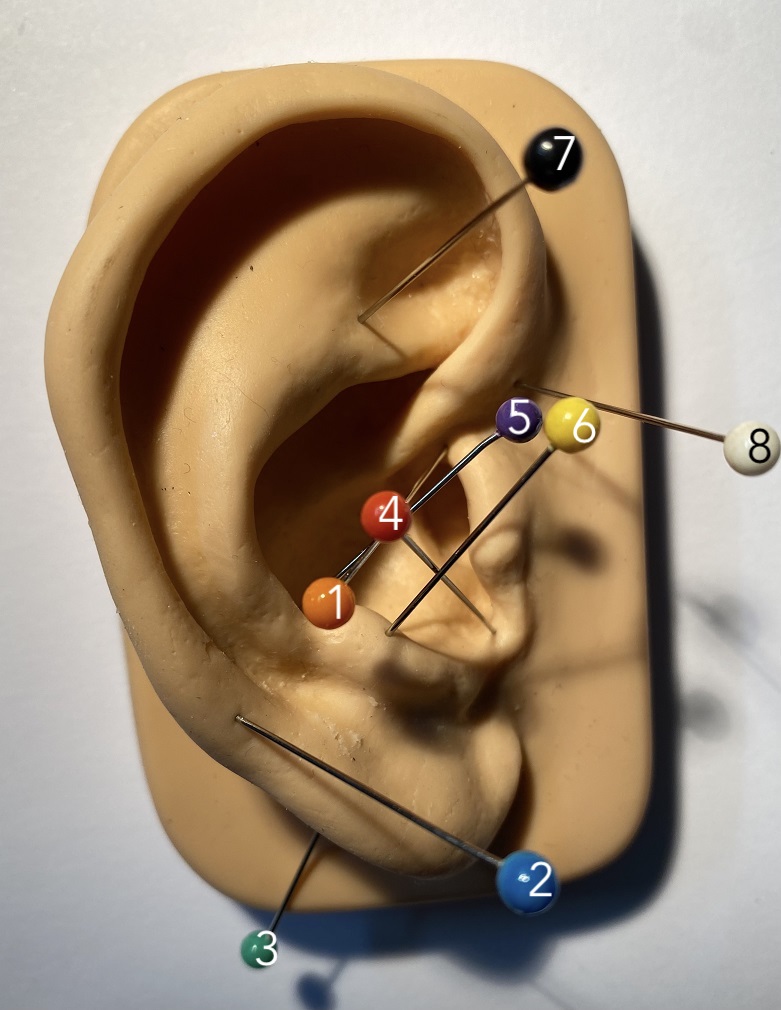
we start with a point named Deep Throat (it corresponds to the Pharyngo-Laryngeal Plexus) to put the brain in alert; it is the point of organ.
Ninth Cranial Nerve, called Glossopharyngeal nerve (sensory), because the mucosa of the larynx is innervated by this nerve.
Tenth nerve Nerve (Vagus) (motor), because the recurrent nerve originates from vagus, and so we can give a better tonus to the muscles of larynx.
ACTH to improve the production of cortisol, stimulating the pituitary gland; it gives a long-acting stimulation.
A point called “Wonderful Point” by Nogier (sympathetic ganglions of C3); it regulates the autonomic activity of the larynx.
PMR (Master Point of reticular substance); it has many activities, and it plays a role in pain control.
Cosmonaut Point (sympathetic ganglion T12-L1); it plays a role in the control of anxiety and in limbic activity.
Epiphysis Point to achieve an appropriate rhythm in the vibration of the vocal folds.
This strategy works in isolation, but also improves outcomes of other therapies in order to achieve a rapid resolution of the problem [8], because the brain reverts to recreate the best homeostasis that it knows.
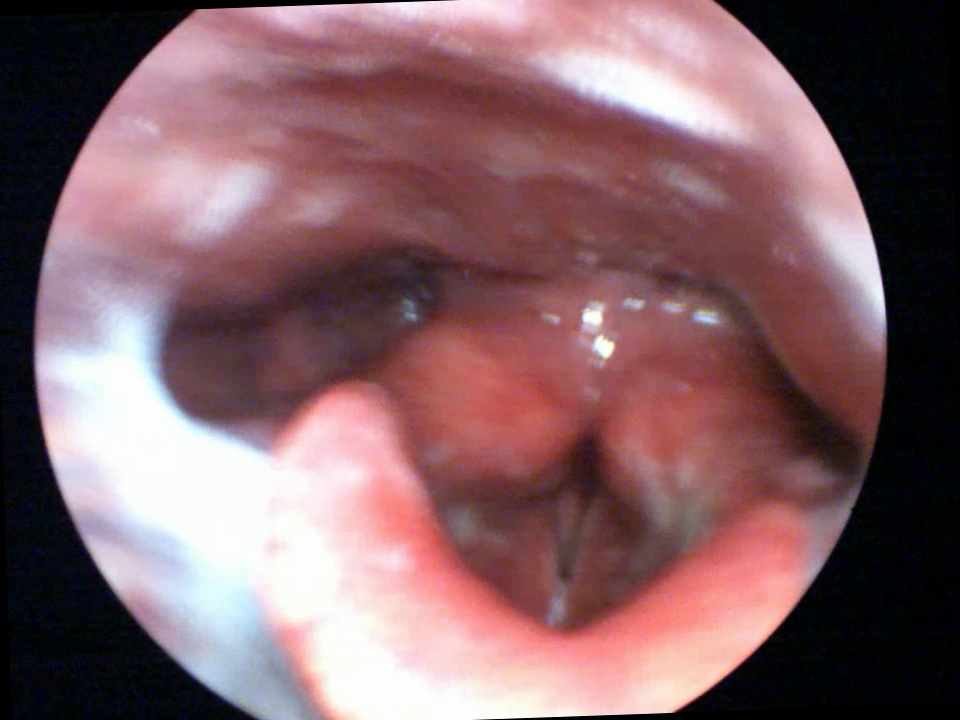
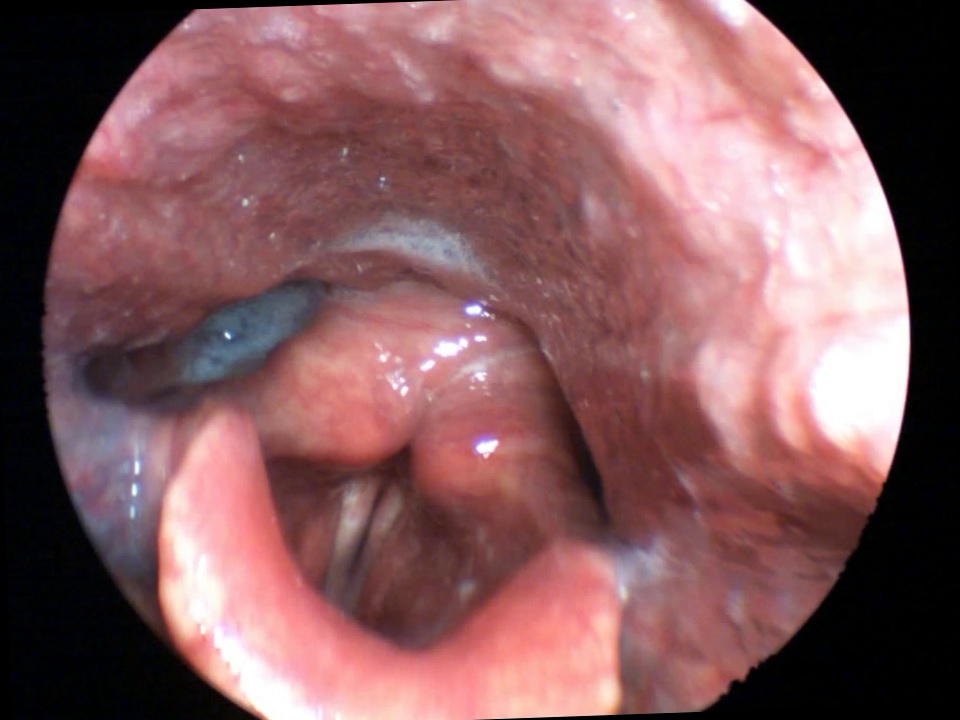
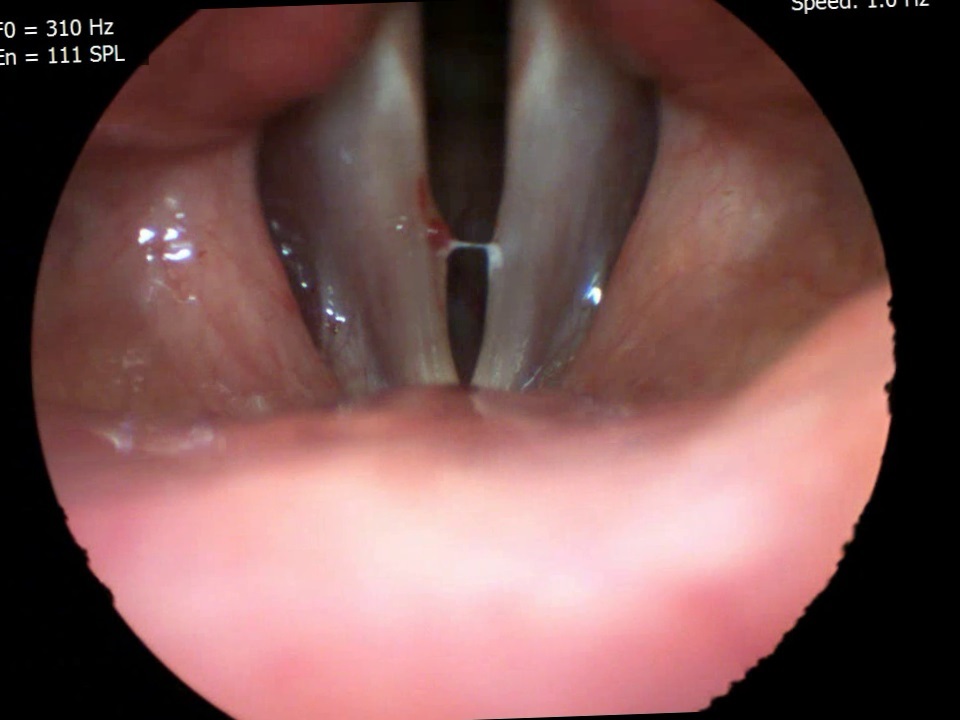
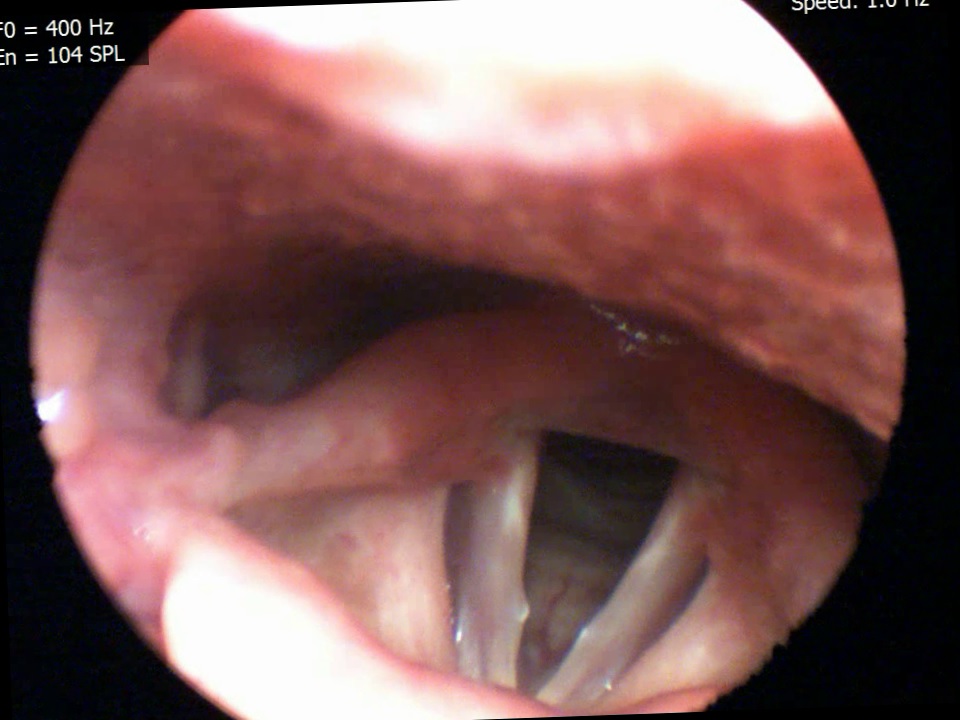
In laryngitis, the induction of endogenous production of cortisol leads to an improvement in inflammation and edema, the action on the cervical sympathetic plexus improves local vascularisation, and the other points of the strategy accelerate healing, which is observed in laryngostroboscopy, as shown in Photos A1 (before the treatment) and A2 (after the treatment).
The larynx is suspended from the hyoid bone, and in turn the skull and the mandible, by muscles and ligaments. It is connected to the postural chains [13], so that possible contractions of these muscles or of other neck muscles, as well as any problems in the temporomandibular joint (TMJ) can change the position of the larynx and influence the efficiency of voice use [8]. A contraction of chewing muscles can affect the quality of the voice by causing the larynx to rise or affecting the cervical muscles [8]. In fact, the postural chains start from the stomatognathic system [8,14]. The postural muscles (tonic postural muscles) are organized in 5 chains [8,13]: anterior (flexors), posterior (extensors) and crossed. They all start from the mouth and end at the feet [14,15]. We can use NAT to solve this problem, working together with speech therapists to rapidly obtain optimal results. The result is emblematic of a well-known phenomenon: posture correction can improve voice [8].
Hypokinetic Dysphonia
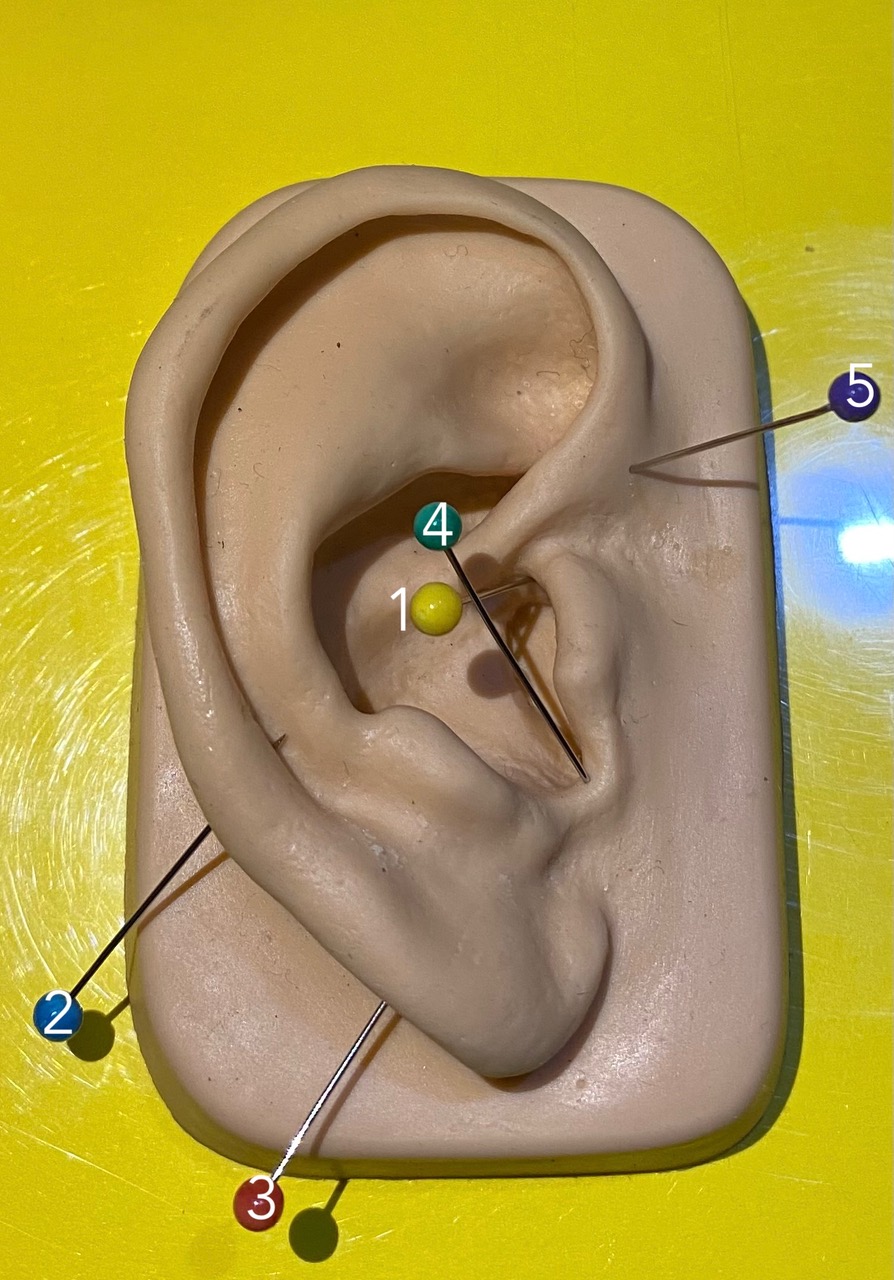
Photo B describes a NAT strategy to work on hypokinetic dysphonia, where objective examination generally shows a deficit of adduction-tension of the vocal folds [8], with varying degrees of incompetence in closing the vocal folds [8]:
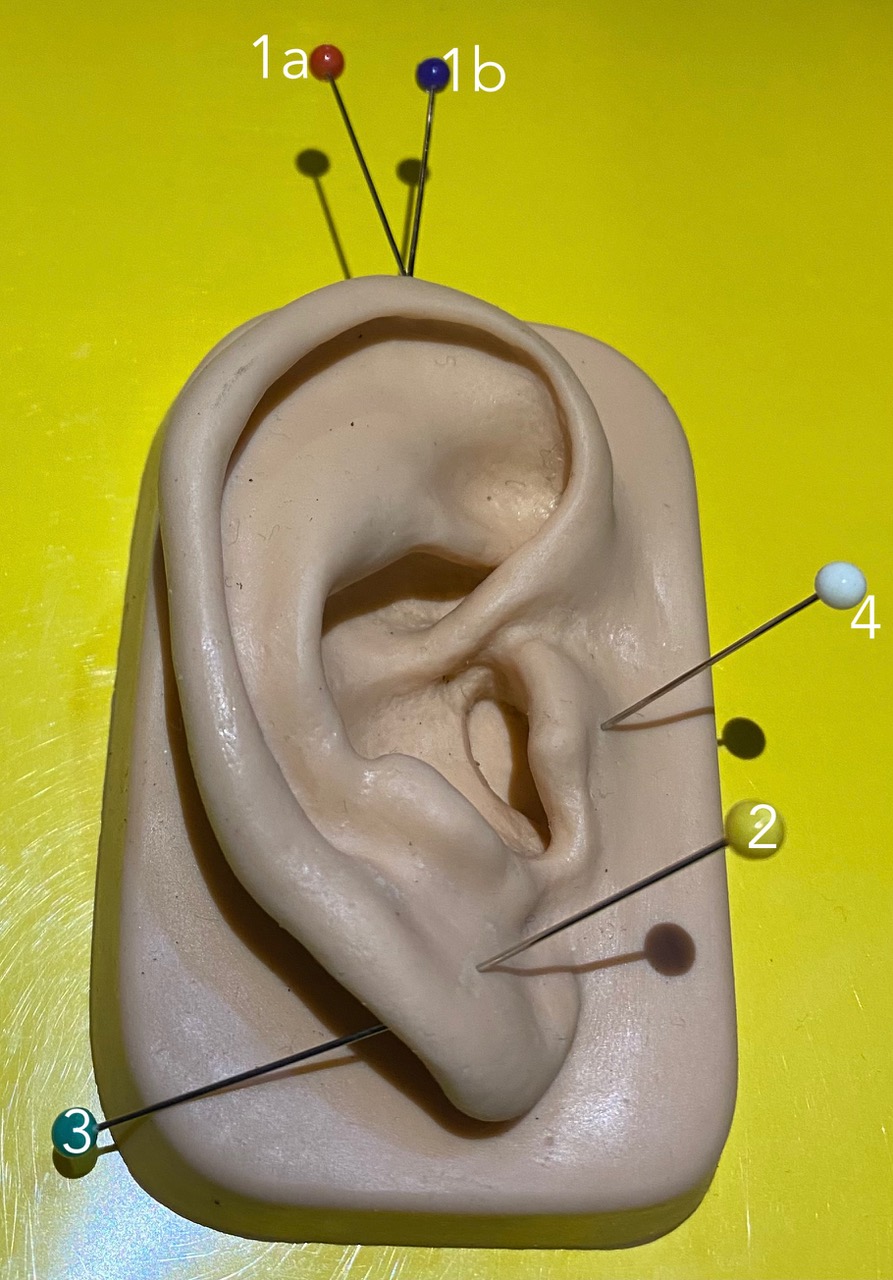
1a Omega2 + 2 PMS (Sensory Master Point) and 3 Motor Master Point + 4 Corpus Callosum + and again 1b Omega 2.
Omega2 is the master point of the mesoderm. By using it, we activate all points of mesodermal origin on the auricular “keyboard”, corresponding to the osteo-arthro-muscular system and to the cardiovascular system. Needling Omega2 also leads to better vascularization of the organ [8].
PMS is located in the center of the lobule and has multiple functions. It is the 4th pain filter (it corresponds to the cortex) [8], but in this case we can use it like a very important central associative area. In fact, it corresponds to the central beam of the telencephalon [8], an impressive intracerebral connection that joins the frontal, temporal, and parietal lobes, and its stimulation increases the phenomena of neuroplasticity and redundancy, improves local homeostasis, promotes secretion of estrogen and progestin hormones, and contributes to the elimination of inhibitions [8].
Motor PMS has an equivalent value from a motor point of view to that of the sensory PMS.
Finally, returning to Omega2 reinforces the strategy. This strategy could enhance rehabilitation techniques and bring better results in the treatment of the problem.
Hyperkinetic Dysphonia
In hyperkinetic dysphonia, the voice is strained [16]; we observe a hard attack, with pneumo-phonetic incoordination associated with the involvement of ancillary muscles (not directly needed for phonation: such as mimics, limb orbicularis, etc.) [8]. In objective examination, though not showing chordal pain, there is protrusion of the false vocal folds, which in adduction tend to cover the true vocal folds until they (false folds) begin to vibrate (hence the phenomenon of bitonality).
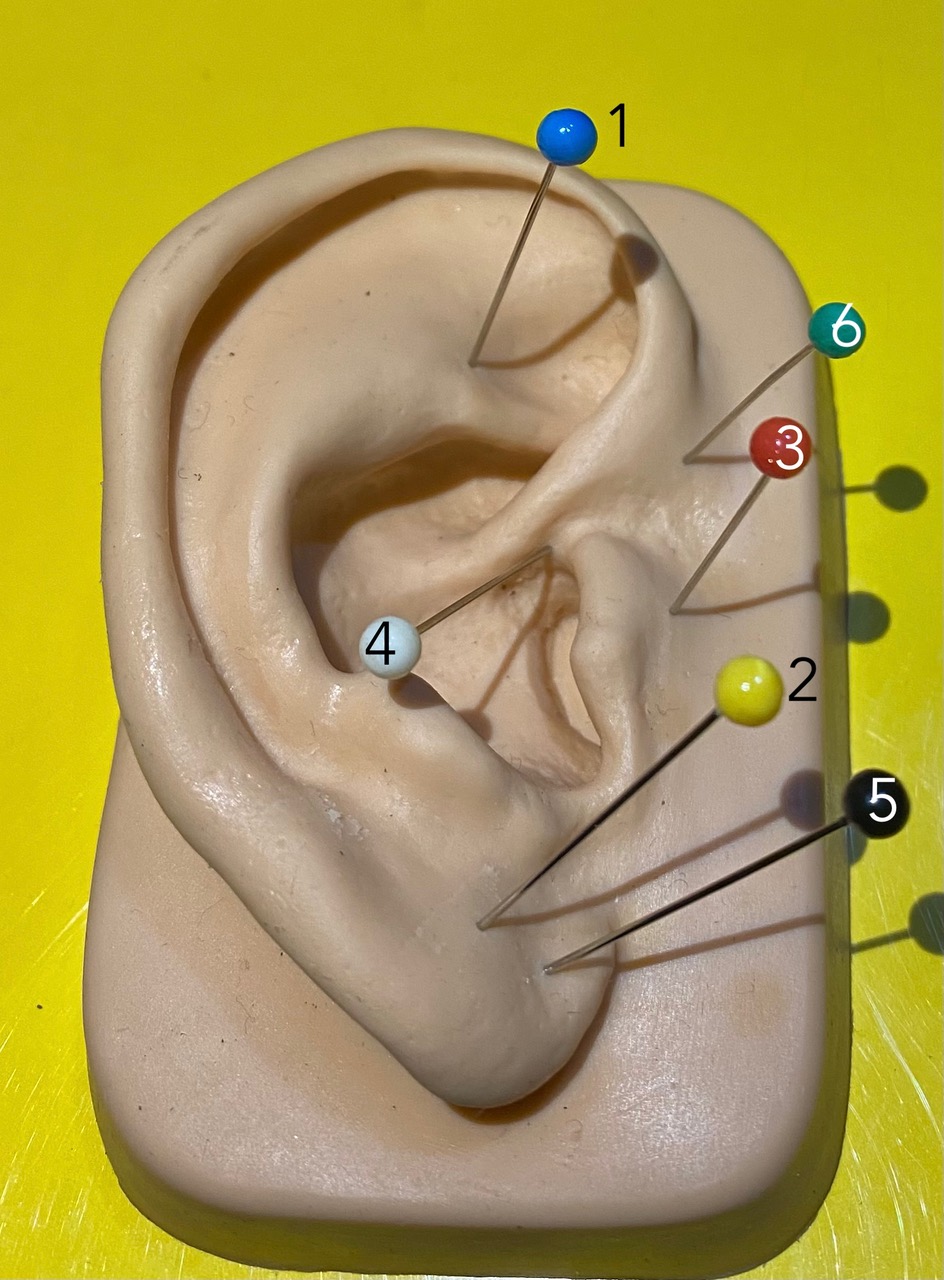
In Photo C we can observe the NAT strategy that we suggest for the treatment of hyperkinetic dysphonia, in addition to logopedic therapy.
1 Omega 2 + 2 PMS Sensitive + 3 PMS Motor + 4 Corpus Callosum + 5 Epiphysis. This last point aims to regularise the frequency of vocal fold vibration.
In dysfunctional dysphonia, such as hypokinetic dysphonia and hyperkinetic dysphonia, NAT helps to acquire the right vibrational rhythm of the vocal folds and the right muscle tone and eliminate the anxiety associated with these pathologies.
Anxiety
NAT is very useful in reducing the anxiety and fear that an artist often has on stage [8].
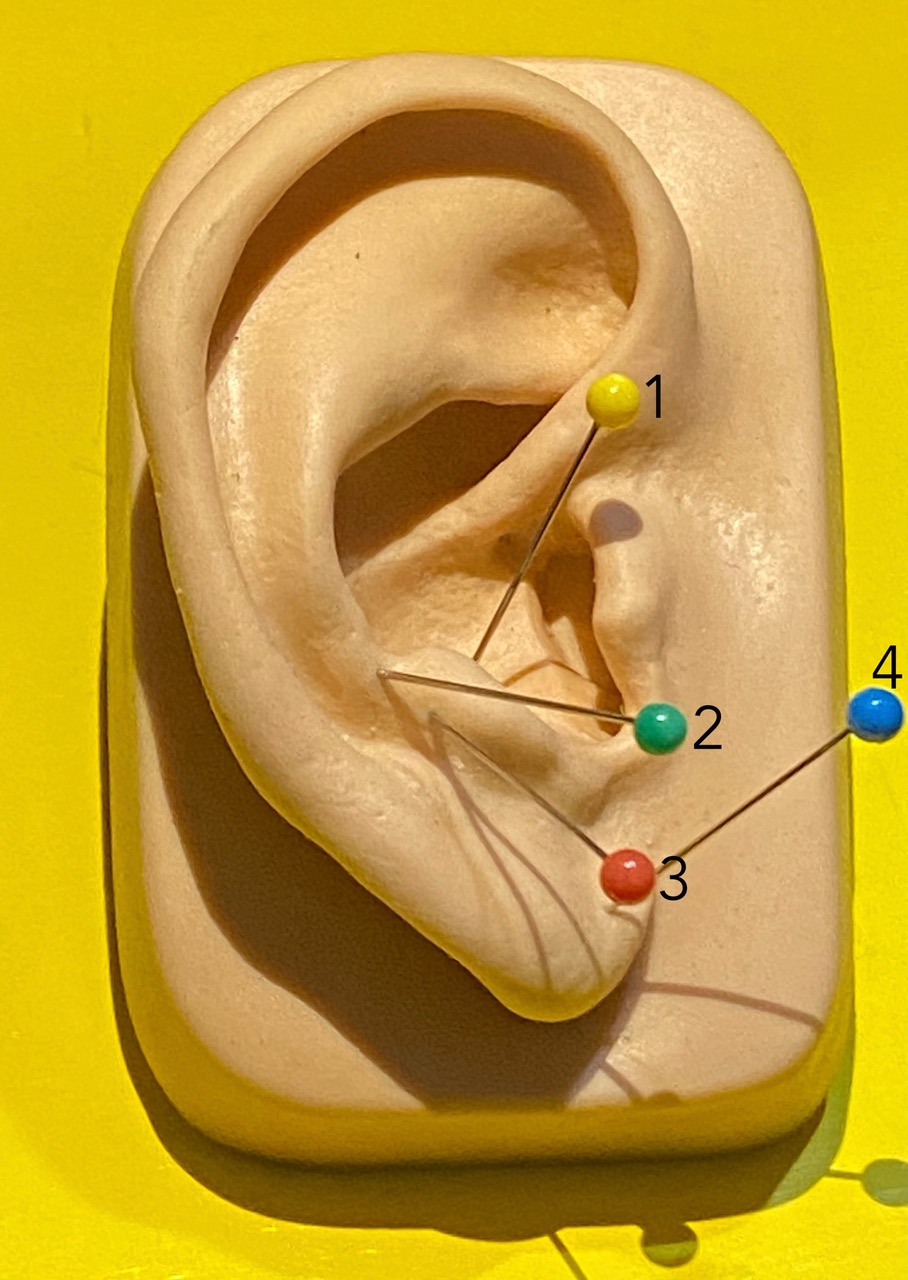
In Photo D we show the NAT strategy suggested for this kind of problem.

We use the Relaxation Triad (called “Triade de Relaxation” in French [2]: 1 Cosmonaut + 2 Sensitive PMS + 3 Corpus Callosum; the needles must be inserted exactly in this sequence). The treatment must be administered bilaterally, beginning with the contralateral side of the dominant ear, because everyone has two different cerebral hemispheres, with different activities [8]. In the right-handed person, the left hemisphere is the rational and the right hemisphere is the artistic, the limbic [8]. The right hemisphere is linked to the left auricle and the left hemisphere to the right auricle [8]. The two hemispheres are connected thanks to the fibers that form the corpus callosum. In the left-handed we use the same triad but starting with the right side.
In the treatment of anxiety, a rebalancing of the autonomic balance is obtained by reducing orthosympathetic activity and therefore reducing the production of stress hormones such as adrenaline, cortisol etc. This action leads to a state of muscular relaxation and remarkable physical well-being.
MTD - Muscle Tension Dysphonia
Another disease where NAT would be very useful is MTD (Muscle Tension Dysphonia).
The causes and the nature of MTD are still unknown. There are many theories, one is that there is an incomplete relaxation of the posterior cricoarythenoid muscle, which is responsible for the opening of the vocal cords. This would result in an excessive contraction of the thyroarytenoid muscle (vocalis muscle). Other theories consider the possibility of excessive compensatory contraction of the intrinsic and/or extrinsic laryngeal muscles. It is also thought that there may be an in-coordination of the laryngeal muscles, associated with contraction, which results in a reduction in the vibration of the vocal folds leading to fatigue and excessive strain in speech.
In laryngoscopy, the whole glottic tract appears to be forced and contracted. It is thought that non-specific irritants such as acid reflux, powders, and cigarette smoke can contribute to the triggering of symptoms.
Some MTDs may, perhaps, derive from the odontostomatognatological pathologies; others may originate from surmenage or malmenage or cervical spine problems (especially atlas or C4). In this case, in addition to ortho-pneumo-phonic and ortho-pneumodic1 re-education (including hygiene re-education), neuroauriculotherapy is useful.
Photo E shows the strategy that we propose for MTD (in conjunction with the well-known therapies):
Relaxation Triad (1 Cosmonaut + 2 Sensitive PMS + 3 Corpum Callosum) with a Mild-Stress and Anti-Noise Effect + 4 Deep Throat + 5 Frontal Lobe (which manages all sphincters, including the larynx) + 6 Epiphysis to bring order to the phonetic rhythm). The treatment is bilateral, starting with the lateral side [8].
Spastic dysphonia
"Spastic dysphonia" or "laryngeal dystonia" is a neurological condition, a form of local dystonia affecting the vocal muscles of the larynx. It is characterized by abnormal involuntary vocal fold movements; the thyroarythenoid muscles are contracted and make render speech tedious, forced, and choked. The voice may tremble or be aspirated and rarely manages to produce low sounds.
Symptoms can improve or disappear when the patient yawns, laughs, sings, or relaxes. The perceptual-acoustic and spectrographic "signs" of spasmodic dysphonia may worsen in certain circumstances such as talking on the phone or in the presence of emotional tension. In some patients, involuntary muscle contractions produce vocal tremor more than a spasm properly mentioned.
Since the causes of spasmodic dysphonia are still unknown, there is currently no cure for this disorder. The injection of periodically repeated botulinum toxin is considered the most effective treatment for most cases.
However, neuroauricolotherapy offers a possible complementary shown in Photo F:
1 Thalamus + 2 Hippocampus + 3 Amigdala + 4 Frontal Lobe.
Thalamus is the last station before the cortex. From there, in fact, begins the corona radiata (thalamo-radiated crown). Pain filter is an integral part of the limbic system [8]. There are four filters of pain starting from the periphery to the brain. The first is the gate control system (the peripheral pain control), the second is reticular substance (this filter controls the pain signals coming from the periphery), the third is thalamus (controls pain signals before they reach the cortex), and the fourth is the cortex (the last filter).
Hippocampus (F14). This is the emotional memory seat, used when you want to dissect emotional memory [8].
Amygdala or Point of Fear (F15). This point is dangerous to elicit because it can trigger anxiety and therefore strong emotional reactions. Its rationale here is based on the pathology being due to a limbic resonance event.
In forms of spasmodic dysphonia, muscular relaxation and regular vibration of the vocal folds are obtained using points of the emotional (limbic) system such as the hippocampus (which is the seat of emotional memory), the amygdala (which is the seat of fear), and the frontal lobe (responsible for the control of all sphincters).
True Vocal Folds Lesions
Vocal fold lesions with “something more” are those in which a vocal fold (or both) has something (congenital or acquired) projecting in the lumen, or characterized by exophytosis: nodules, polyps, cysts, papillomas, malignant tumors, etc.
Depending on the specific pathology, intervention is usually based on speech therapy; other times surgical exeresis is also necessary. To enhance the effects of speech therapy and surgery, a neuroauriculotherapy strategy administered in pre- and post-surgery can be useful.
Photos G1 and G2 show the NAT strategy for unilateral or bilateral lesion of the vocal fold, from two different points of view for a better understanding:
If the vocal fold lesion is unilateral or bilateral, the recommended protocol, as pictures G1 and G2 show, is composed of:
1 Deep throat + 2 IX motor + 3 Vagus Motor + 4 ACTH + 5 Epiphysis
Deep throat to orient the brain towards the larynx, the affected organ.
IX Motor Nerve because the muscles of pharynx involved in the tone of the resonators are innervated by the glossopharygeal nerve.
Vagus Motor Nerve because the cranial nerve X innervates the intrinsic laryngeal muscles.
ACTH to induce cortisol production from the adrenal cortex with prolonged anti-inflammatory and trophic effect.
Epiphysis because voice and vibration of the vocal folds are functions interconnected and linked through a precise relationship/rhythm (epiphysis is the gland which manages all biological rhythms).
Photo H shows a different strategy proposed for the same problem:
The suggested strategy consists of 1 Cosmonauts + 2 Deep throat + 3 Corpus Callosum + 4 Synthesis Point. Corpum Callosum is required to improve coordination of the entire larynx movement and not just the one of the two true vocal folds [8].
In lesions of the vocal folds, such as those described above, excellent results are obtained in association with speech therapy. The cranial nerves that innervate the intrinsic laryngeal muscles are stimulated in order to maintain a correct tone, the production of endogenous cortisol is increased for anti-inflammatory purposes, and a regular vibration of the vocal folds is achieved through stimulation of the epiphysis.
Photo H1 shows a laryngoscopy of a lesion before treatment and Photo H2 shows a laryngoscopy of the same patient after treatment.
Conclusions
In conclusion, as voice is a complex activity under the control of our brain, and as speaking and singing are activities that must take place under the right rhythms in frequencies (regulated by the epiphysis [8]), NAT appears to be a viable method to improve the treatment of voice problems, to enhance the results of other therapies based on drugs or rehab, and to induce relaxation. In neuroauriculotherapy, the ear is used to give the brain orders in a process that has a logical basis in neurophysiology [2]; fMRI has demonstrated that the analogy between the auricle and the corresponding brain areas is extremely precise, and it reproduces clearly the sensory, motor and visceral homunculus present at the cortical level.
NAT is a young discipline, scientifically proven with functional dynamic MRI. At the beginning of the 2000s, there were several studies on pain, but there are no specific studies on the voice to date.
Diseases of the vocal tract can be dysfunctional or organic. According to our clinical experience, we can say that neuroauriculotherapy can be used in both situations. Some effective applications of NAT in voice science that revealed noticeable improvements of the related disorder are the activation of the filters of pain, the enhancement of the activity of parasympathetic or sympathetic nervous system and the modulation of autonomic balance, the enhancement of cortisol production, an improvement of the rhythm of speech, a better coordination of the activity of the two hemispheres in control of voice using the corpus callosus (over 298 millions of fibers that connect the two hemispheres), the reduction of anxiety, and more [8].
As the results presented here are part of our clinical practice, more formally structured studies are required to make solid conclusions. However, we believe that in the meantime these observations based on our experience can stimulate a productive discussion on the possible applications of NAT to voice medicine that might be helpful as a reference for further studies.

