










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista MVZ Córdoba
versión impresa ISSN 0122-0268versión On-line ISSN 1909-0544
Rev.MVZ Cordoba vol.24 no.2 Córdoba mayo/ago. 2019
https://doi.org/10.21897/rmvz.1399
Clinical Case
Canine atypical hyperadrenocorticism associated with hypothyroidism
1Universidade Federal de Rio Grande do Sul (UFRGS), Faculdade de Medicina Veterinária, Laboratório de Análises Clínicas Veterinárias, Porto Alegre, RS, Brasil.
2UFRGS, Faculdade de Medicina Veterinária, Departamento de Medicina Animal, Serviço de Endocrinologia e Metabologia do Hospital de Clínicas Veterinárias, Porto Alegre, RS, Brasil.
Hyperadrenocorticism (HAC) is one of the most common endocrinopathies in dogs, caused by excessive synthesis of cortisol. Atypical or occult HAC is a syndrome characterized by the presentation of clinical, biochemical, and imaging alterations compatible with hypercortisolism, but normal results in endocrine tests that are conventionally used for HAC diagnosis. However, these patients present high serum concentrations of precursors or other corticoadrenal hormones. The present study describes the case of an 8 years old female canine, Bichón Frisé, epileptic and treated with phenobarbital, presenting clinical signs associated with HAC, in which the low-dose dexamethasone suppression test and stimulation with ACTH resulted within normal values. The measurement of adrenal steroids, after ACTH stimulation, showed abnormal elevation of estrogen and progesterone, the latter persisting after the patient was spayed. Treatment with trilostane allowed the reduction of progesterone levels and the partial resolution of clinical signs. However, full clinical recovery was only achieved after the diagnosis and treatment of concomitant hypothyroidism. The challenge that represent the diagnosis of atypical HAC highlights the importance of performing and having availability of panels that include measurement of adrenal steroid hormones other than cortisol, as well as considering the occurrence of other concomitant endocrine metabolic diseases.
Keywords: Adrenal; canine; progesterone; steroids; trilostane (Source: DeSC)
El hiperadrenocorticismo (HAC) es una de las endocrinopatías más frecuentes en caninos, producida por la síntesis excesiva de cortisol. El HAC atípico u oculto es un síndrome caracterizado por la presentación de alteraciones clínicas, bioquímicas e imagenológicas compatibles con hipercortisolismo, pero con resultados normales en las pruebas endocrinológicas utilizadas convencionalmente para diagnóstico de HAC. Sin embargo, estos pacientes presentan elevada concentración sérica de precursores u otras hormonas corticoadrenales. El presente estudio describe el caso de una canina hembra, Bichón Frisé de 8 años de edad, epiléptica y tratada con fenobarbital, presentando signos clínicos asociados a HAC, en la que el test de supresión con dexametasona a dosis bajas y de estimulación con ACTH arrojaron valores normales. La medición de esteroides adrenales, post estimulación con ACTH, mostró elevación anormal de estrógenos y progesterona, persistiendo esta última después de que la paciente fuera esterilizada. El tratamiento con trilostano permitió la disminución de los niveles de progesterona y la resolución parcial de los signos clínicos. Sin em bargo, la recuperación clínica en su totalidad sólo se obtuvo después del diagnóstico y tratamiento del hipotiroidismo concomitante. El desafio que representa el diagnóstico del HAC atípico resalta la importância de realizar y disponer de paneles que incluyan medición de hormonas esteroideas adrenales diferentes al cortisol, además de considerar la ocurrencia de otras enfermedades endocrinas metabólicas concomitantes.
Palabras clave: Adrenal; canino; esteroides; progesterona; trilostano (Fuente: DeSC)
INTRODUCTION
Hyperadrenocorticism (HAC) is a common endocrinopathy in dogs, representing more than 30% of endocrine cases presented in clinical settings 1. It is estimated that 80-85% of cases are caused by hypersecretion of adrenocorticotropic hormone (ACTH) mainly of pituitary origin, being called pituitary-dependent HAC (HPD), or also ACTH-dependent HAC. Rarely, it may arise as a paraneoplastic syndrome, secondary to ectopic ACTH-producing neuroendocrine tumors 2. The remaining 15-20% corresponds mainly to adrenocortical tumors, or to less frequent causes, such as bilateral adrenocortical hyperplasia generated by aberrant expression of hyperactive ectopic or eutopic hormone receptors 3.
The classic HAC clinical signs include abdominal distention, bilateral alopecia, muscular and cutaneous atrophy, hepatomegaly, arterial hypertension, persistent panting, polyphagia, polydipsia and polyuria. The most relevant hematological and serum biochemistry alterations include stress leukogram and elevation of the activity of hepatobiliary enzymes such as alkaline phosphatase (ALP) and alanine aminotransferase (ALT), in addition to the concentration of glucose, cholesterol and triglycerides. Urinalysis may reveal proteinuria and reduced specific gravity 4,5.
These findings are usually associated with hypercortisolism, however, they have been reported in patients with negative results to conventional HAC diagnostic tests, such as low-dose dexamethasone suppression test (LDDST), and the ACTH stimulation test (ACTHST). This syndrome is known as "atypical" or "occult" HAC (AHAC), and has been widely debated in the literature, without a full clarification of its etiology, as there is not enough scientific evidence to explain the pathophysiological mechanisms that produce the clinical signs 6.
According to the 2012 ACVIM consensus statement for the diagnosis of HAC, AHAC is defined as a "syndrome in which a dog apparently presents HAC based on anamnesis, physical examination and clinical-pathological findings, but the LDDST, urinary cortisol: creatinine ratio (UCCR) and ACTHST result within reference values" 3. In 2015, only 14 cases reported met the specified characteristics 4,5. The last one was published in 2017, in Germany 7.
The aim of this study is to report an AHAC case associated with hypothyroidism from the referral of the patient to the Endocrinology Service of the Hospital of Veterinary Clinics of the Federal University of Rio Grande do Sul, until the resolution of the case, illustrating the diagnostic complexity of the syndrome.
PATIENT EXAMINATION
Anamnesis. An 8-year-old bitch, Bichon Frisé, sexually intact, was admitted to the Endocrinology Service of the Hospital of Veterinary Clinics from the Federal University of Rio Grande do Sul. The owner reported that few months ago the patient gained weight and was constantly panting, presenting polyuria, polydipsia, polyphagia and non-pruritic abdominal alopecia. Additionally at home, it remained prostrate and very sleepy. The patient was being medicated with S-adenosyl methionine (SAMe), a nutritional supplement for liver patients, and phenobarbital (2.5 mg/kg BID) due to a previous diagnosis of primary epilepsy. According to the owners, the patient had sporadic seizure episodes. Liver enzymes activity elevation had not responded properly to the treatment with SAMe. Severe hypercholesterolemia (700 mg/dL), moderate hypertriglyceridemia (240 mg/dL), mild non-regenerative anemia, and thrombocytosis (600x 106/ mm3) were found in previous routine examinations. In a previously performed LDDST test, basal serum cortisol was 0.26 ug/dL (reference value: 0.5-6 ug/dL), and 8 hours post-dexamethasone administration it was 0.07 ug/dL (reference value: <1.4 ug/dL), suggesting a negative result for HAC due to effective hypothalamic-pituitary-adrenal axis inhibition.
Clinical findings. Constant panting, potbellied abdomen difficult to palpate, truncal hypotrichosis, alopecic abdominal skin, hyperpigmented, and comedones (Figures 1, 2). Body condition score (BCS) of 4/5, abdominal circumference: 61 cm. There were no other relevant findings on the clinical examination.

Figure 1 Ventral view of the patient. On the left side in the first consultation, presenting a distended abdomen, alopecia, hyperpigmentation and the presence of comedones. On the right, four months after starting trilostane treatment, with hair growth and less distension.

Figure 2 Side view of the patient. On the left side in the first consultation, there is evident abdominal distension and poor quality coat, with preserved extremities. On the right, one year after treatment with trilostane and syntectic levothyroxine, showing less abdominal distension, repigmentation and marked improvement in coat quality.
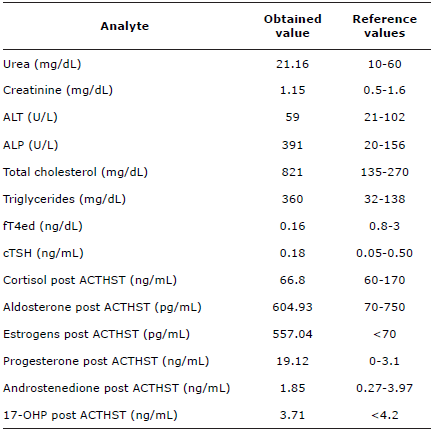
Diagnostic tests used. Basal blood samples were collected from the jugular vein of the patient, in EDTA tube for complete blood count (CBC), and in glass tube without additives to evaluate free T4 by equilibrium dialysis (fT4ed), cTSH and serum biochemical analytes (urea, creatinine, ALT, ALP, total cholesterol and triglycerides). An ACTHST was performed, administering cosyntropin (5 ug/kg IV) and one hour later, a blood sample was collected in glass tube without additives for measurement of cortisol, aldosterone, total estrogen, progesterone, androstenedione and 17-hydroxyprogesterone (17-OHP). Analytes results are shown in table 1. For ovarian hormones reference values for sexually intact females were considered.
Table 1 Values of serum biochemistry and endocrine analytes evaluated in the patient's first consultation.
The CBC showed normal results, except for the red blood cell count, which was 4.17x106/mm3 (reference value, 5.5-8.5 x 106/mm3). The decrease in fT4ed was initially considered secondary to phenobarbital chronic treatment. Abdominal ultrasound revealed hepatomegaly with hyperechoic parenchyma and moderate quantity of sediment within the gallbladder. The adrenal glands presented usual echogenicity and adequate dimensions, measuring the left 1.61 x 0.54 cm and 1.66 x 0.44 cm the right. No alterations were observed in the ovaries, although a mild increase in size of the uterine horns (0.72 cm) was reported.
Treatment and evolution. The patient was spayed as a treatment for diagnosed hyperestrogenism. However, four months after surgery, a new ACTHST was performed evaluating post-stimulation cortisol, estrogen and progesterone due to the persistence of clinical signs, especially dermatological ones, as well as biochemical alterations. Elevation in progesterone was observed (15.80 ng/mL, spayed female reference value, <1.3 ng/mL), while cortisol remained within normal values (132.2 ng/mL) and estrogen decreased to 0.13 ng/mL (spayed female reference value, <0.5 ng/mL).
Treatment with trilostane was instituted (0.7 mg/kg BID) associated with ursodiol (8 mg/kg PO BID). One month after starting treatment, there was a reduction in post-ACTH cortisol and progesterone concentration (71.3 ng/mL and 2.14 ng/mL, respectively). Clinically, polyuria and polydipsia decreased, as well as panting. Despite still potbellied, there was a moderate decrease in abdominal circumference (55 cm). Abdominal skin was still pigmented, but without comedones, and with few areas of hair growth. It should be mentioned that despite numerous tegument characteristics associated with HAC were present, the patient did not show evident dermal atrophy.
Four months after starting trilostane treatment, alopecia and potbellied abdomen decreased significantly (Figure 1). Trilostane dose was adjusted (0.9 mg/kg PO BID) due to overall laboratorial results and post-ACTH cortisol concentration higher than the desired value for a patient under treatment (20-60 ng/mL). Two weeks after the readjustment, thyroid status was reviewed. The fT4ed concentration was still reduced (0.30 ng/ dl), while the TSH was within the reference values. Sodium levothyroxine was instituted (12 ug/kg PO SID) to normalize the low ft4ed concentration evidenced in previous analysis. One year after starting trilostane and thyroxine treatment, the patient was clinically stable, presenting normal water and food consumption, with resolution of abdominal alopecia, and mild abdominal distension (abdominal circumference: 43 cm) allowing abdominal palpation (Figure 2). The CBC, serum biochemical analytes, ACTHST, steroid profile and basal fT4ed were performed, all within reference values, except for ALP activity (248 IU), probably induced by phenobarbital. The owners did not report recurrence of epileptic seizures in the patient, who continued receiving treatment with phenobarbital, ursodiol, trilostane in doses adjusted according to need, and levothyroxine. The patient deceased with 13-years old due to endocardiosis and congestive heart failure complications not related with endocrine diseases control.
DISCUSSION
According to the established by Behrend et al 3, the patient presented 7/9 of the most frequent clinical signs associated with HAC, 4/7 of the less frequent signs, and several characteristic biochemical alterations of the disease. The previously performed LDDST discarded HAC and before treatment with trilostane, post-ACTH cortisol concentrations were within reference range. This fact plus to the persistent progesterone elevation after sterilization, and the adequate response to treatment with trilostane, allowed to determine the diagnosis of AHAC in this particular patient.
Usually, it is possible to diagnose HAC using the LDDST, which offers a sensitivity around 85% and specificity of 80%, in contrast to the sensitivity of 80% and specificity of 64 to 86% of the ACTHST 4. The risk of false positive is greater in geriatric patients, who may present clinical signs compatible with HAC, caused by another disease. An extended LDDST was recently proposed for the diagnosis of AHAC, performing the last measurement of cortisol 12 hours after administration of dexamethasone (0.01 mg/kg IV), however, there was no statistically significant difference between the cortisol concentration of healthy patients and patients with suspected AHAC 6,8. The AHAC syndrome is potentially, the result of outdated reference values for LDDST and ACTHST 4. However, even if more stringent reference intervals were used for the LDDST and ACTHST tests in this case, cortisol was suppressed in the LDDST, and there was no exacerbated cortisol response (value close to the upper reference limit) in the ACTHST. In addition, patients treated with phenobarbital can have false positive results in the LDDST test due to the inductive effect of this drug on metabolic liver enzymes 4, so these results must be interpreted with caution, making an adequate correlation with the clinical picture.
Currently, the only test that allows diagnosis of AHAC is the ACTHST with subsequent steroid hormones and cortisol precursors measurement. However, the concentration of cortisol precursors such as 17-OHP, 21-deoxycortisol and 11-deoxycortisol can be highly variable, generating overlaps between the values of patients with HAC, other diseases, and even healthy ones 9.
Recently, 17-OHP has been proposed as the precursor of choice in steroid hormone profiles for the diagnosis of AHAC and for treatment monitoring 10. However, in the case, post-ACTH 17-OHP was found within the reference values, explaining why this recommendation was ruled out. Patients with non-adrenal neoplasms can also present high concentrations of 17-OHP, so the role of cortisol precursors in the pathophysiology of the disease is a controversial issue that has not been elucidated yet 9,11.
The patient presented high serum concentrations of progesterone, even after being spayed. In canines and felines, hyperprogesteronism per se may produce clinical signs similar to those seen in HAC and, in women, it has been demonstrated that high levels of progesterone can displace cortisol from corticosteroid-binding globulin (CBG), increasing the concentration of the free fraction, which exerts the biological activity 12. In the study by Monroe et al. 13, in patients with HAC of adrenal, pituitary, and other non-adrenal origin, the measurement of progesterone and 17-OHP reached sensitivity of 88% and 91%, respectively. However, due to the low specificity of these two hormones (55 and 59%) it is not recommended to use them as routine tests for HAC diagnosis, except in those cases where conventional tests show negative results and there is strongly evidence suggesting HAC 4.
One of the most persistent paraclinical abnormalities in the patient was the decrease in erythrocyte count. In a low proportion of dogs with HAC, erythrocyte membrane antiphospholipid antibodies were identified 14, being an uncommon finding. The concomitant hypothyroidism in the patient, added to the chronic disease process, could explain the anemia that resolved after the levothyroxine treatment.
The inhibitory action of endogenous glucocorticoids in the hypothalamic-pituitary-thyroid axis of humans, rodents and canines has been widely described, demonstrating that management of HAC can solve the problem. However, the influence of the elevation of other corticoadrenal steroids on the thyroid function of patients with AHAC has not been described. In this case, the decrease in free T4 was initially attributed to phenobarbital, which increases its hepatic metabolism. Phenobarbital could also have contributed to the elevation of ALP, a characteristic biochemical alteration of the HAC that the patient presented until the last performed tests. It is considered that hypothyroidism secondary to hypercortisolism is a consequence of the pituitary suppression of TSH exerted by glucocorticoids 5, however, it is interesting that in this case, TSH suppression was not detected. Moreover, a cTSH within reference range does not rule out primary hypothyroidism. Therefore, the continued suppressed fT4ed concentration even after adequate trilostane therapy, and excellent clinical response to levothyroxine therapy were considered supportive evidence for associated primary hypothyroidism in this patient.
The adequate response to trilostane treatment was a key element to confirm AHAC diagnosis. Considering that there were no structures compatible with adrenal tumors on abdominal ultrasound, trilostane treatment was suggested instead of mitotane to avoid the side effects of this medication. The patient received low doses of trilostane, administered at a 12-hours interval according to the protocol proposed by Feldman 15, achieving absolute resolution of the clinical signs, without side effects after several years of administration. Treatment with trilostane at low doses, twice a day, has been shown to be effective in patients with HAC of pituitary and adrenal origin. Trilostane decreases the synthesis of 17-OHP, however, it is not recommended to control the effectiveness of the treatment, considering that some patients may have an increase in this hormone 10. Even after medication and adequate management of the HAC, some patients may present changes in the pigmentation of the coat, as seen in Figure 2. Histologically, there is an increase in the proliferation of melanocytes in the stratum corneum, epidermis and dermis, however, the physiopathological mechanism of this phenomenon has not been clarified 5.
The adrenal steroid profile is a useful tool for the diagnosis of patients with AHAC; however, it does not replace the standard tests (LDDST and ACTHST) and should be used only when conventional tests results are negative in patients with history and clinical signs compatible with HAC. Treatment using low doses of trilostane demonstrated excellent efficacy in the control of the AHAC in the patient, encouraging its use in patients with HAC of any origin, reducing the risk of adverse effects associated with the treatment, as long as the owners follow the established administration times.
REFERENCES
1. Pöppl A, Coelho I, Da Silveira C, Moresco M, De Carvalho G. Frequency of endocrinopathies and characteristics of affected dogs and cats in southern Brazil (2004-2014). Acta Sci Vet. 2016; 44(1379):1-9. https://doi.org/10.22456/1679-9216.81099 [ Links ]
2. Castillo V, Pessina PP, Gardía JD, Gallelli MF, Miceli DD, Cabrera MF. Ectopic ACTH syndrome in a dog with mesenteric neuroendocrine tumour: a case report. Vet Med. 2014 59(7):352-358. https://doi.org/10.17221/7623-VETMED [ Links ]
3. Kooistra HS, Galac S. Recent advances in the diagnosis of Cushing's syndrome in dogs. Topics in Compan An Med. 2012; 40(2):259-267. https://doi.org/10.1016/j.cvsm.2009.10.002 [ Links ]
4. Behrend EN, Kooistra HS, Nelson R, Reusch CE, Scott-Moncrieff JC. Diagnosis of spontaneous canine hyperadrenocorticism: 2012 ACVIM Consensus statement (small animal). J Vet Intern Med. 2013; 27(6):1292-1304. https://doi.org/10.1111/jvim.12192 [ Links ]
5. Behrend EN. Canine hyperadrenocorticism. En: Feldman EC, Nelson RW, Reusch C, Scott-Moncrieff JC, Behrend EN. Editores. Canine & Feline Endocrinology, 4a ed.. St Louis: Saunders Elsevier; 2015. https://doi.org/10.1016/B978-1-4557-4456-5.00010-9 [ Links ]
6. Behrend EN, Kennis R. Atypical Cushing's syndrome in dogs: Arguments for and against. Vet Clin Small An. 2010; 40(2):285-296. https://doi.org/10.1016/j.cvsm.2009.11.002 [ Links ]
7. Hoffrogge S, Fels L, Schmicke M, Mischke R. Atypisches Cushing-Syndrom bei einem Hund. Tierarztl Prax Ausg K. 2017; 45(3):186-192. https://doi.org/10.15654/TPK-160255 [ Links ]
8. Fowler KM, Frank LA, Morandi F, Whittemore JC. Extended low dose dexamethasone suppression test for diagnosis of atypical Cushing's syndrome in dogs. Domest Anim Endocrinol. 2017; 60:25-30. https://doi.org/10.1016/j.domaniend.2017.03.002 [ Links ]
9. Sieber-Ruckstuhl NS, Boretti FS, Wenger M, Maser-Gluth C, Reusch CE. Evaluation of cortisol precursors for the diagnosis of pituitary-dependent hypercortisolism in dogs. Vet Rec. 2008; 162(21): 673-678. https://doi.org/10.1136/vr.162.21.673 [ Links ]
10. Ristic JME, Ramsey IK, Heath FM, Evans HJ, Herrtage ME. The use of 17-Hydroxyprogesterone in the diagnosis of canine hyperadrenocorticism. J Vet Intern Med. 2002; 16(4): 433-439. https://doi.org/10.1111/j.1939-1676.2002.tb01261.x [ Links ]
11. Behrend EN, Kemppainen RJ, Boozer AL, Whitley EM, Smith AN, Busch KA. Serum 17-alpha-hydroxyprogesterone and corticosterone concentrations in dogs with nonadrenal neoplasia and dogs with suspected hyperadrenocorticism. J Am Vet Med Assoc. 2005; 227(11):1762-1767. https://doi.org/10.2460/javma.2005.227.1762 [ Links ]
12. Syme HM, Scott-Moncrieff JC, Treadwell NG, Thompson MF, Snyder PW, White MR, Oliver JW. Hyperadrenocorticism associated with excessive sex hormone production by an adrenocortical tumor in two dogs. J Am Vet Med Assoc. 2001; 219(12):1725-1728. https://doi.org/10.2460/javma.2001.219.1725 [ Links ]
13. Monroe WE, Panciera DL, Zimmerman KL. Concentrations of noncortisol adrenal steroids in response to ACTH in dogs with adrenal-dependent hyperadrenocorticism, pituitary-dependent hyperadrenocorticism, and nonadrenal illness. J Vet Intern Med. 2012; 26(4):945-952. https://doi.org/10.1111/j.1939-1676.2012.00959.x [ Links ]
14. Miller AG, Dow S, Long L, Olver CS. Antiphospholipid Antibodies in Dogs with Immune Mediated Hemolytic Anemia, Spontaneous Thrombosis, and Hyperadrenocorticism. J Vet Intern Med. 2012; 26(3): 614-623. https://doi.org/10.1111/j.1939-1676.2012.00922.x [ Links ]
15. Feldman EC. Evaluation of twice-daily lower-dose trilostane treatment administered orally in dogs with naturally occurring hyperadrenocorticism. J Am Vet Med Assoc. 2011; 238(11):1441-1451. https://doi.org/10.2460/javma.238.11.1441 [ Links ]
How to cite (Vancouver) Quishpe-Contreras y Gomes-Pöppl. Canine atypical hyperadrenocorticism associated with hypothyroidism. Rev MVZ Cordoba. 2019; 24(2):7262-7267. DOI: https://doi.org/10.21897/rmvz.1399
Creative Commons Attribution 4.0 International License This article is distributed under the terms of the (https://creativecommons.org/licenses/by-sa/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source. 
Received: September 01, 2018; Accepted: February 01, 2019; Published: June 01, 2019
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
