










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957versión On-line ISSN 2500-7440
Rev Col Gastroenterol v.24 n.3 Bogotá jul./sep. 2009
Single balloon enteroscopy. A new tool for gastrointestinal evaluation
John Ospina Nieto, MD., MSCC., MSCG., MSCED., MSCH., MFELAC. (1), John Villamizar Suárez, MD., MSCG., MSCED. (2)
(1) Gastrointestinal Surgeon and Digestive Endoscopist. Coordinator of Gastrointestinal Surgical Services and Endoscopy at the Hospital Cardiovascular El niño'de Cundinamarca (Children's Cardiovascular Hospital of Cundinamarca) in Soacha, Cundinamarca and at the Dispensario Médico Gilberto Echeverri Mejìa (Gilberto Echeverri Mejìa Medical Dispensary in Bogota. Member of the Gastrointestinal Surgery Committee of the Colombian Surgical Society. Bogotá, Colombia.
(2) Gastrointestinal Surgeon and Digestive Endoscopist. Hospital Cardiovascular del Niño de Cundinamarca SALUDCOOP Liga contra el cáncer. (League against Cancer) Bogotá, Colombia.
Received: 05-02-09 Accepted: 13-08-09
Summary
Introduction and aims: Until recently the most useful tools designed for evaluating the small intestine were the endoscopic capsule and double balloon enteroscopy. However, the search for a safer, faster, less complicated technique has led to the development of the single balloon enteroscopy system. This paper presents our experience with this technique in the Hospital Cardiovascular del Niño in Cundinamarca (Soacha-Colombia) along with a brief review of the most important aspects of performing this procedure.
Patients and Methods: Between January 15, 2009 and February 15, 2009 a prospective study was conducted on 29 patients at the Hospital Cardiovascular El niño'. A total of 41 single balloon enteroscopies were performed on these patients. Indications, times of procedures, findings and complications were studied in all of these patients.
Results: Average diagnostic time was 28.5 minutes with 71 minutes of total procedure time. Total explorations using mixed approaches were performed on two patients (16%). Findings included foreign bodies, angiodysplasias, Crohn's disease, Peutz-Jeghers Syndrome, vasculitis, nodular lymphoid hyperplasia, intestinal varicose veins and neoplasias. Diagnostic yield for occult bleeding was 81%. No complications were registered.
Conclusions: Although this technique has been used for only a few weeks, we can already conclude that Single Balloon Enteroscopy is a safe, fast and reliable technique for small intestine evaluation.
Key words
Enteroscopy, Single Balloon, Small intestine.
INTRODUCTION
A few years ago endoscopic studies of the small intestine were limited for a variety of anatomical and structural reasons that made exploration difficult. The small intestine was commonly known as the "Dark Continent" of the gastrointestinal tract (1).
Classically, attempts to evaluate this organ endoscopically appeared around 1972 with Dr. Classen's reports on ileoscopy in Dtsch med Wochenschr (Deutsche Medizinische Wochenschrift - German Medical Weekly). Nine years later, Dr. Bosseckert wrote about intra-operative enteroscopy in Endoscopy. (This is still a useful tool in countries like ours. Until recently it was the gold standard for intestinal evaluation.) Then, in 1986, Dr. Tada published his work with transnasal enteroscopy. In 1997 Dr. Benz's technique called "Push enteroscopy" appeared.
The new century welcomed in the most useful tools yet: the endoscopic capsule and, one year later, the possibility of performing endoscopic therapy in the intestine through the Double-Balloon enteroscopy system of Dr. Yamamoto. The evolution of these tools has continued, resulting in the single balloon enteroscopy system in 2007.
In the present article we show the experience of our group with the single balloon enteroscopy system and briefly review technical aspects of this procedure (2-7).
MATERIALS AND METHODS
Equipment, technical requirements and preparation
Single balloon enteroscopy was performed by oral, anal or combined routes in accordance with clinical indications. To perform this procedure a single balloon video enteroscope (Olympus Enteropro Single Balloon SIF-Q180) was used with the standard preparation recommended for colonoscopy. Patients were Bly advised not to consume red beverages and/or jelly the day before the procedure, but consumption of abundant oral liquids was insisted upon.
The procedure was performed under sedation. In our institution all sedation is performed with Midazolam® and Profolol®. Dosage was 0.5mg/Kg Bolo followed by 1.5-4.5mg/Kg/hour infusion in patients under 55 years. 80% of these dosages were administered to patients over 55 years old. Procedures were monitored by the anesthesiology group. Oxygen was supplied through nasal cannula. Anesthesia was administered intravenously through a permeable vein in the right arm. Electrocardiogram limb lead II, pulse oximetry and measurement of blood pressure were used to monitor the patient.
Push Technique
Once the enteroscope has been introduced by the oral or anal route, we used the push technique described by the Japanese group (12). It is important to note that memorization and strict application of these steps decrease the procedure time, risks and complications of the procedure (for easier memorization of the procedure which "adds direction" in the intestine, we designed a mnemonic device - ADD DIR - based on the Spanish phrase Adicionar Dirección (Add Direction) and the initials in Spanish of the steps in the procedure Avanzo, Doblo, Desinflo, Deslizo, Insuflo, Retiro.)
Push Technique
Push the enteroscope (Avanzo)
Fold and anchor the tip of the device (Doblo)
Deflate the balloon from the overtube (figure 1) (Desinflo)
Slide the overtube over the enteroscope (figure 2) (Deslizo)
Insufflate the balloon again. (Insuflo)
Remove enteroscope and overtube (figure 3) (Retiro)
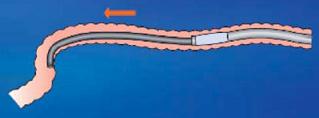
Figure 1. Balloon deflated from the overtube.
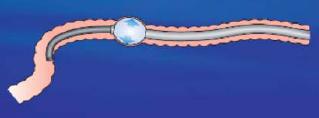
Figure 2. Overtube slid over enteroscope.
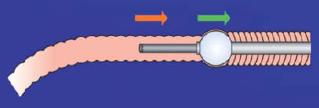
Figure 3. Enteroscope removed from overtube.
Source: Images from the performance of single balloon Enteroscopy. Japanese enteroscope insertion technique study group. Published in collaboration with Olympus Medical System group.
RESULTS
41 enteroscopic procedures were performed on 29 patients: 21 urgent cases with occult sources of bleeding and 8 elective-hemorrhages (with obscure bleeding, polyposis and neomasses) in the Hospital Cardiovascular del Niño de Cundinamarca between January 15, 2009 and February 15, 2009 (table 1). 13 of the 29 patients were women and 16 were men. Their ages ranged from 13 to 69 years with an average age of 46.
Table 1. Indications, studies performed, and symptoms encountered for each patient evaluated with the single balloon technique.
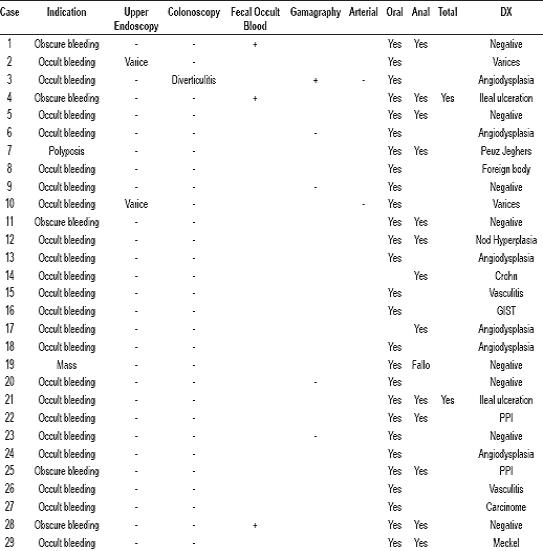
There were 6 cases of obscure bleeding, 21 cases with occult sources of bleeding, one case of a mass in the digestive tract (diagnosed by intestinal transit radiology) and one polyposis case (diagnosed by endoscopy). Patients' histories showed:
Superior endoscopy performed on all patients. Two had evidence of esophageal varices that did not explain bleeding. The other endoscopies had not explained the patients' medical states.
Colonoscopy was performed on all patients. One had diverticular disease without evidence of hemorrhaging. Another patient presented slight ulceration that did not explain the patient's medical condition/state.
Gammagraphy was performed with Tc -99m labeled red blood cells on five of the 21 patients with occult hemorrhaging. The exam was positive in one case with reported hemorrhaging in the upper left abdominal quadrant.
Ateriography was performed on two of the patients (celiac trunk study and inferior mesenteric celiac trunk study). Both showed negative for digestive tract hemorrhaging.
Capsule Endoscopy was not performed because of lack of resources.
Presence of occult blood in fecal matter (Hemoccult® II) was found in three patients diagnosed with obscure bleeding.
Digestive tract study of one patient (intestinal transit of hydrosoluble media) showed an image suggestive of jejunal mass.
The approach was decided upon according to each patient's medical condition (Melena, hematemesis or rectorragia). Complete intestinal explorations were performed on two patients (16% of studied patients) using a combined approach (12 in total) and 1cc sterile India ink administration. It should be noted here that complete explorations were not performed in four other cases because the exploration was suspended once the causes of hemorrhaging had been identified. It was not possible to pass the ileocecal valve of one patient through rectal entry. No major or minor complications (fever, abdominal pain, odynophagia, ileum) were registered.
Average diagnosis time (time between beginning of enteroscopy and identification of pathology) was 28.5 minutes. Average procedure time was 72 minutes. Average fluoroscopy time was 48 seconds. It should be noted that this last procedure was performed on only 24 patients. The other 5 studies were performed in the intensive care unit where fluoroscopy is not available. The average speed of advance of the enteroscope was calculated at 7.4 cm/sec. It ranged between 3.5 and 12.5 cm/sec. This measure was obtained with approximations of the times it took to evaluate segments and to remove them making it inexact. It may be the least important of these measurements.
Total exploration was performed on two patients, who were dyed with sterile India ink during oral exploration. Combined procedures were performed, with procedure times of 85 minutes.
The following findings were reported: 8 negative cases, 3 of them with obscure bleeding; one foreign body (gauze) (figure 4), six angiodysplasia cases (figure 5), Crohn's disease; two ileal ulcerations (figure 6), one Peutz-Jeghers Syndrome (figure 7); two vasculitis cases, one Ileal-lymphoid-nodular hyperplasia (figure 8), two patients with intestinal varices (figure 9); two patients with neoplasmic lesions (gastrointestinal stromal tumor (GIST) and Adenocarcinoma); one Meckel's diverticulitis and two cases of multiple intestinal parasitism.
Seventeen patients were diagnosed with occult hemorrhaging. Yield obtained was 80%. In obscure bleeding the Yield obtained was 60%.

Figure 4. Gauze in the Jejunum.

Figure 5. Intestinal Angiodysplasia.
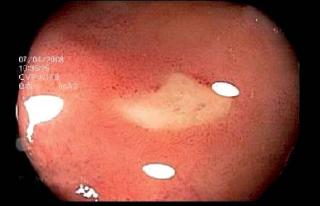
Figure 6. Ileal Ulceration.

Figure 7. Peutz-Jeghers Syndrome.

Figure 8. Ileal-Lymphoid-Nodular Hyperplasia.
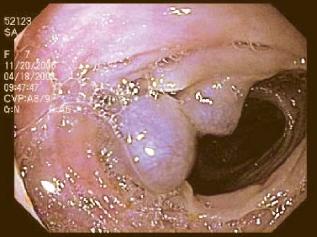
Figure 9. Ileal varices.
DISCUSSION
A few years ago, small intestine pathology studies were complicated and not very precise. The concepts of obscure and occult bleeding were not that clear. The challenge of surgery was faced without important tools including TAC, intestinal transit, gammagraphy, arteriography and even intraoperatory enteroscopy (Recommended by Dr. Bosseckertand considered to be the gold standard study for small intestinal evaluation (1, 2, 4, 7).
As previously mentioned attempts at endoscopic evaluation of the small intestine began around 1972 with Dr. Classen's ileoscopy reports. Nevertheless, the most useful tools for evaluation of the small intestine have appeared in the 21st century. They include the endoscopic capsule, double-balloon enteroscopy and single balloon enteroscopy (2-7).
The single balloon enteroscopy technique for studying small intestine pathology was developed recently, and was only approved in 2007. This technique aims at decreasing exploration time and making intestinal evaluation easier.
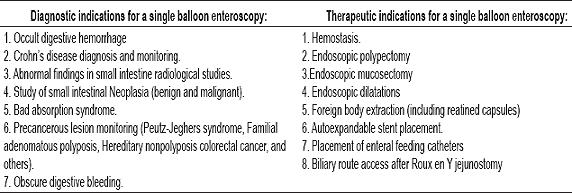
Indications for performance of a single balloon enteroscopy are the same as those for other kinds of enteroscopies and small intestinal studies. They are divided into diagnostic and therapeutic indications as in table 2 (1, 8, 9, 11-14, 19).
Table 2. Indications for Enteroscopy
Our series corroborates the conclusion that the most important diagnostic indication for this procedure is occult digestive bleeding which was found in 75% of the cases in our study.
Other indications for this procedure are:
Endoscopy study in patients with bariatric surgery
Difficult ileal intubation during colonoscopy
Difficult colon polypectomy
Calibration of the device and its angulations is important to facilitate difficult colonoscopy procedures and complicated polypectomies because it makes retroflection simpler (figure 10).

Figure 10. Retroflexion maneuver during colonoscopy.
There are few contraindications to performance of this procedure. They include:
Gastrointestinal tract perforation
A patient with a generally poor state of health
Characteristics associated with ill health
Uncooperative and/or difficult patient
Health provider lacking knowledge of technique
Complications
Although few studies have been published regarding this type of enteroscopy, the technique is considered to be very safe, and no major complications have been reported. Complications similar to those encountered with the double balloon technique can be expected with the single balloon technique. They are rare and include (1, 8, 12-15):
Intestinal perforation
Hemorrhaging
Mucosal lacerations
Acute pancreatitis
Elongated ileum following the procedure.
Secondary effects including abdominal pain, self limiting fever, and odynophagia.
Inherent complications in therapeutic procedures including polypectomy, dilatations, hemostasis, and foreign body extraction.
Complications related to sedation.
In our short experience we have experienced no major or minor complications with this technique. Since our institution does not perform double balloon technique it is not possible for us to compare the two techniques. However, our evidence fully supports the utility of combining endoscopic capsule and enteroscopy techniques to improve the diagnostic yield of studies.
To recapitulate, single balloon enteroscopy is a safe new endoscopic procedure which presents several advantages over other small intestine diagnostic study techniques. Nevertheless, there have been few studies comparing enteroscopic techniques due to the recent appearance of single balloon devices. Among the advantages which found with this new technique, and which should be evaluated in the future, we found:
A reduction in time required by endoscopic exploration which should benefit both doctors and patients.
Fast preparation. To begin exploration it is sufficient to lubricate the overtube interior with sterile serum and introduce the endoscope into the overtube.
Incorporation of narrow band imaging vision allows observation of enteric mucosal vascular patterns which aids in diagnosis of tumor tissue.
Hypoallergenic. Enteroscope components which contact the patient are made of silicon, decreasing risks of inducing hypersensitivity reactions caused by exposure to allergenic materials such as latex.
Disposable material. The overtube, insufflation tube and cover for long distance handling are all disposable which decreases the risk of infection by cross contamination.
Having a conventional caliber work channel allows use of accessory materials of all types, which is less expensive than if a different caliber had been used.
Direct examination of the total enteric mucosal can be done.
Additional diagnostic and therapeutic procedures can be done without changing the equipment.
More than 300 procedures confirm that the technique is safe when performed under adequate conditions.
Before finishing, it is important to emphasize that although single balloon enteroscopy's appearance holds great promise as a new tool for evaluating intestinal pathology, it is not a replacement for other techniques such as the endoscopic capsule or double balloon enteroscopy.
The current recommendation is to associate capsule technique with all enteroscopic techniques to improve diagnostic performance. Finally, we would like to reiterate the point that literature and published studies comparing the two enteroscopic techniques, and which would thus allow a conclusion of which one is better, still do not exist.
REFERENCES
1. Reyes G. Estudios para intestino delgado - parte I. Sociedad Colombiana de Gastroenterología.
2. Carey J, Fleischer D. Investigation of the Small Bowel in Gastrointestinal Bleeding-Enteroscopy and Capsule Endoscopy. Gastroenterol Clin N Am 2006; 34(4): 719-734.
3. ASGE Technology Status Evaluation Report: Wireless capsule endoscopy.
4. Linder J, et al. Diagnostic Yield and Clinical Implications of Push Enteroscopy. Results from a Nonspecialized Center. J Clin Gastroenterol 2002; 35(5): 383-6.
5. Gostout CJ Sonde-enteroscopy: technical depth of inserts and yield of lesions. Gastrointest Endosc Clin N Am 1996; 6: 777-847.
6. Cave DR, Cooley JS. Intraoperative enteroscopy: indications and techniques. Gastrointest Endosc Clin N Am 1996; 6: 793-802.
7. Yamamoto H, Sekine Y, Sato Y, et al. Total enteroscopy with a nonsurgical steerable double-ballon method. Gastrointest Endosc 2001; 53: 216-20.
8. May A, Nachbar L, Ell C. Double-balloon enteroscopy (push-and-pull enteroscopy) of the small bowel: feasibility and diagnostic and therapeutic yield in patients with suspected small bowel disease. Gastrointest Endosc 2005; 62: 62-70.
9. Kaffes A, et al. Double balloon enteroscopy in the diagnosis and the management of small bowel diseases: an initial experience in 40 patients. Gastrointest Endosc 2006; (63): 81-6.
10. Ell C, May A, et al. Push and pull enteroscopy in the small bowel using the double-balloon technique: results of a prospective European Multicenter study. Endoscopy 2005; 37 (7): 613-6.
11. Heine GD et al. Double-balloon enteroscopy: indications, diagnostic yield, and complications in a series of 275 patients with suspected small-bowel disease. Endoscopy 2006; 38(1): 42-8.
12. Practice of single Ballon Enteroscopy. Japanese enteroscope insertion technique study group. Published in collaboration with olympus medical system group 2007.
13. Lapalus M, Ponchon T, et al. Single-balloon enteroscopy: a preliminary experience. Gastrointestinal endoscopy 2007; 65: AB184.
14. Hartmann A, Eickhoff R, Tamm J, Riemann F. Balloon-assisted enteroscopy using a single-balloon technique. Endoscopy 2007; 39: E276.
15. Tsujikawa T, Saitoh Y, Andoh A, Imaeda H, Hata K, Minematsu H, Senoh K, Hayafuji K, Ogawa A, Nakahara T, Sasaki M, Fujiyama Y. Novel single-balloon enteroscopy for diagnosis and treatment of the small intestine: preliminary experiences. Endoscopy 2007.
1. Reyes G. Estudios para intestino delgado - parte I. Sociedad Colombiana de Gastroenterología. [ Links ]
2. Carey J, Fleischer D. Investigation of the Small Bowel in Gastrointestinal Bleeding-Enteroscopy and Capsule Endoscopy. Gastroenterol Clin N Am 2006; 34(4): 719-734. [ Links ]
3. ASGE Technology Status Evaluation Report: Wireless capsule endoscopy. [ Links ]
4. Linder J, et al. Diagnostic Yield and Clinical Implications of Push Enteroscopy. Results from a Nonspecialized Center. J Clin Gastroenterol 2002; 35(5): 383-6. [ Links ]
5. Gostout CJ Sonde-enteroscopy: technical depth of inserts and yield of lesions. Gastrointest Endosc Clin N Am 1996; 6: 777-847. [ Links ]
6. Cave DR, Cooley JS. Intraoperative enteroscopy: indications and techniques. Gastrointest Endosc Clin N Am 1996; 6: 793-802. [ Links ]
7. Yamamoto H, Sekine Y, Sato Y, et al. Total enteroscopy with a nonsurgical steerable double-ballon method. Gastrointest Endosc 2001; 53: 216-20. [ Links ]
8. May A, Nachbar L, Ell C. Double-balloon enteroscopy (push-and-pull enteroscopy) of the small bowel: feasibility and diagnostic and therapeutic yield in patients with suspected small bowel disease. Gastrointest Endosc 2005; 62: 62-70. [ Links ]
9. Kaffes A, et al. Double balloon enteroscopy in the diagnosis and the management of small bowel diseases: an initial experience in 40 patients. Gastrointest Endosc 2006; (63): 81-6. [ Links ]
10. Ell C, May A, et al. Push and pull enteroscopy in the small bowel using the double-balloon technique: results of a prospective European Multicenter study. Endoscopy 2005; 37 (7): 613-6. [ Links ]
11. Heine GD et al. Double-balloon enteroscopy: indications, diagnostic yield, and complications in a series of 275 patients with suspected small-bowel disease. Endoscopy 2006; 38(1): 42-8. [ Links ]
12. Practice of single Ballon Enteroscopy. Japanese enteroscope insertion technique study group. Published in collaboration with olympus medical system group 2007. [ Links ]
13. Lapalus M, Ponchon T, et al. Single-balloon enteroscopy: a preliminary experience. Gastrointestinal endoscopy 2007; 65: AB184. [ Links ]
14. Hartmann A, Eickhoff R, Tamm J, Riemann F. Balloon-assisted enteroscopy using a single-balloon technique. Endoscopy 2007; 39: E276. [ Links ]
15. Tsujikawa T, Saitoh Y, Andoh A, Imaeda H, Hata K, Minematsu H, Senoh K, Hayafuji K, Ogawa A, Nakahara T, Sasaki M, Fujiyama Y. Novel single-balloon enteroscopy for diagnosis and treatment of the small intestine: preliminary experiences. Endoscopy 2007. [ Links ]

