










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957versión On-line ISSN 2500-7440
Rev Col Gastroenterol v.24 n.4 Bogotá dic. 2009
The relation of dyspepsia and gastroesophageal reflux to emotional factors: impact on the education and social activity of adolescents
Jenny Molano C. (1), Sandra Piñeros O. (1), Clara López de Mesa M. (1)
(1) Area of Internal Medicine, Faculty of Medicine, Universidad de La Sabana, Bogotá, Colombia.
This study was approved by the subcommittee of investigation of the Faculty of Medicine of the Universidad de La Sabana and financed by the patrimony fund for research of the Universidad de La Sabana.
Received: 29-09-09 Accepted: 21-10-09
Summary
Introduction and objectives. Anxiety and depression have been related with dyspepsia and reflux disease. We conducted a cross sectional, population based study, with the objectives to determine relation of dyspepsia and reflux symptoms with emotional factors and the impact on school assistance and social activity in students.
Methods. 937 students between 12 to 20 years selected at random answered a survey on the presence, frequency, leading events and other characteristics of dyspeptic and reflux disease symptoms occurred in the last year and the Zung´s scales of anxiety and depression. Correlation with endoscopic findings was established.
Results. Self - reported symptoms of depression and anxiety were statistically significant in adolescents (p=0,001), whereas only anxiety symptoms were significant in adolescents with reflux disease (p=0,001). Neither anxiety nor depression was related to type of dyspepsia (organic or functional). Cigarette smoking and alcohol use were significant in adolescents with dyspepsia. (p=0,004) and (p=0,015)
Conclusions. Dyspepsia and reflux disease symptoms have a B association with school assistance and with daily and social activities in adolescents. Self reported symptoms of anxiety and depression are frequent in students with dyspepsia and symptoms of anxiety are frequent in students with reflux disease symptoms, but are not related with type of dyspepsia (organic or functional).
Key words
Dyspepsia, reflux disease, adolescents, anxiety, depression, Quality of life.
Introduction
Emotional factors are considered in both onset and evolution of dyspepsia and acid peptic disease (1). Comorbidity with psychiatric disorders, especially anxiety disorders, was considered (1, 2).There are few publications about the epidemiology of dyspepsia in adolescents (3, 4) its effect on education and social activities and its relation with anxiety and depression.
The biopsychosocial model proposes that high emotional stress, regardless of cause, is related both in origin and evolution to acid peptic disorders. (5, 6)
Knowledge of emotional factors in children and adolescents with dyspepsia and reflux and its effect on education and daily and social activities are relevant for successful intervention among members of this population suffering from this pathology. It is also important for its projection into the adult population. For these reasons we chose to undertake this study within this population base.
The study determined the prevalence of disorders including organic and functional dyspepsia and gastroesophageal reflux among educated adolescents. Those results have already been published in the Revista Colombiana de Gastroenterologia (4). Now we are publishing results obtained relating to the effects of dyspepsia and reflux on students education and social activity, the of these digestive tract symptoms of anxiety and depression and to the consumption of cigarettes, alcohol and analgesics, and the relation of that consumption with dyspepsia, different types of dyspepsia, and with gastroesophageal reflux among educated adolescents between 12 and 20 years of age.
Materials and methods
A community-based cross-sectional study of people between 12 and 20 years of age was conducted within the greater metropolitan area of Bogotá in Cundinamarca Department in Colombia. The cities and municipalities of Bogotá, Chia, Tabio, Cajicá and Sopó were covered. All are located in savannah of Bogotá, an Andean plain 2600 meters above sea level. It has an urban and rural population of approximately ten million people, of which approximately 1,500,000 are between the ages of 10 and 20 years old. www.dane.org.gov.co.
35 educational institutions situated in the selected geographic area were randomly selected. None of them serve populations with special educational needs. 12 of these 35 institutions agreed to participate in the study.
There were no statistically significant differences in variables of socioeconomic status and sex between participating and non-participating institutions. Lists of all students between 12 and 20 years of age were requested. From those lists students were randomly selected according to age, sex, location and socioeconomic strata of the educational institution. Invitations to participate in the study were sent to students and their parents or guardians.
The size of the sample was calculated based on expected peptic ulcer frequency of 4%, with an alpha error of 0.005%, and a margin of random sampling error of 1.5%. The number of subjects was 722. A 30% overestimation was made to take into account the percentage of subjects not answering the questionnaire. Finally 937 subjects were recruited.
All subjects between 12 and 20 years of age, except for pregnant teenagers, were included. Guidelines for performing upper endoscopies were established which included treatment to eradicate Helicobacter pylori 6 months before the endoscopy. A self-processed instrument for collecting information was designed and then evaluated in a pilot sample to determine comprehensibility of questions. Since subjects with low levels of education were included, medical students were trained as tutors to assist in this process. Training emphasized that tutors were not to induce answers. The instrument contained questions about the presence of dyspeptic symptoms and typical symptoms of gastroesophageal reflux (GER) within the last year. It also included questions about the presence of alarming symptoms including upper digestive tract bleeding, vomiting, weight loss and epigastric pain affecting normal sleep. It included questions about triggering events for symptoms and related school absenteeism, effect on daily and social activities, and consumption of cigarettes, alcohol and analgesics. Zung questionnaires on anxiety and depression were included.
Symptoms of dyspepsia considered included: epigastric pain, epigastric discomfort, gastric fullness, precocious satiety, nausea, and epigastric distention. Alarming symptoms considered were: epigastric pain that affected normal sleep, weight loss, vomiting, history of upper digestive tract bleeding. Symptoms considered for gastroesophageal reflux were pyrosis and regurgitation.
According to the participants predominant symptoms two groups were established, one based on reflux, the other on dyspepsia:
1. "Patients" with diagnoses of dyspepsia included those who "always" or "frequently" showed some of the dyspeptic symptoms previously noted and those who showed symptoms less frequently but also showed some alarming symptoms.
2. "Patients" with diagnoses of reflux were those who showed pyrosis and/or regurgitation occurring "always" or "frequently" during the last year.
Those who were asymptomatic or who had occasional symptoms of reflux or dyspepsia, but without alarming symptoms, were considered to be "healthy". Those identified as patients were contacted for clinic evaluation and upper endoscopy.
Zung questionnaires for anxiety and depression disorders are self administered instruments valid at both the national and international level. They allow identification of symptoms of anxious and depression disorders (7-9). According to the rating system of those questionnaires, corrected scores (SDS) greater than or equal to 50 were considered as indicating students with symptoms suggestive of anxiety disorder and depressive disorder. They were further sorted into three groups: slight severity (scores between 50 and 59), moderate severity (scores between 60 and 69), and severe (scores greater than 70).
An upper endoscopy was performed with an Olympus (GIF C) video endoscope. Biopsies were taken for urease tests and identification of Helicobacter pylori. In additional biopsies were taken from any lesions meriting them. Antrum and fundus biopsies were performed on patients who had received proton pump inhibitors or antibiotic therapy for any reason within two months of the study. All endoscopies were recorded. The endoscopy was interpreted as positive for a structural cause for any of the following diagnoses: gastric or duodenal ulcers, erosive duodenitis, gastric neoplasia or acute erosive gastritis. The minimum size guideline for the definition of erosions was (5 mm) (10). The endoscopy was considered to be negative if erythema, hyperemia and7or non-erosive inflammatory signs were found. Patients were considered to have different types of functional dyspepsia according to the predominant symptoms: dyspepsia due to ulcer if pain was the predominant symptom, dysmotility-like dyspepsia if distention or gastric fullness were the predominant symptoms, or non-specific dyspepsia if it was not possible to establish a predominant symptom according to ROMA II (11-14).
Statistical Methods
An Excel® data base was built and the information was processed in statistic pack SPSS version 14.0. Results were presented as proportions for discrete variables and as averages and standard deviations for continuous variables. The relation between variables was explored using the chi-square test and Students t for normal distributions and Fisher and Mann-Whitney for non-normal distributions. OR and 95% confidence intervals were calculated.
Results and Analysis of Results
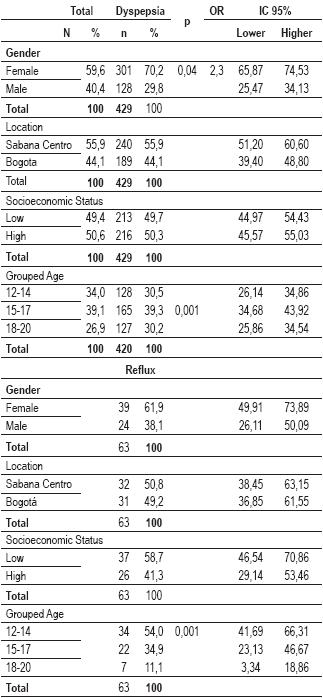
General aspects: Distributions of the sample for sex, age, location and socioeconomic strata of the educational institution are shown in Table 1.
Table 1. Dyspepsia and reflux according to socio-demographic variables.
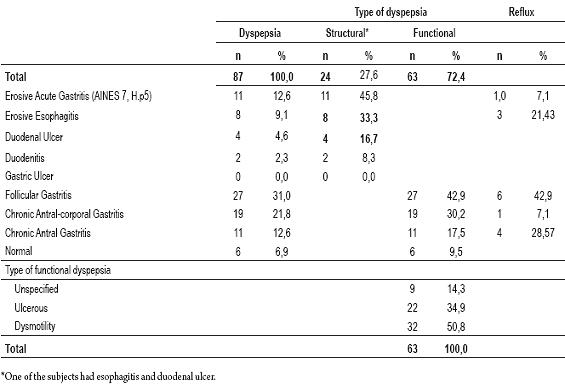
45.8% of the youths were diagnosed with "dyspepsia" and 6.7% with "reflux". 87 endoscopies for dyspepsia were performed, organic causes were found in 27.6% of those cases. Endoscopies were performed for 14 cases of reflux (Table 2) (4).
Tabla 2. Endoscopic findings in dyspepsia and reflux
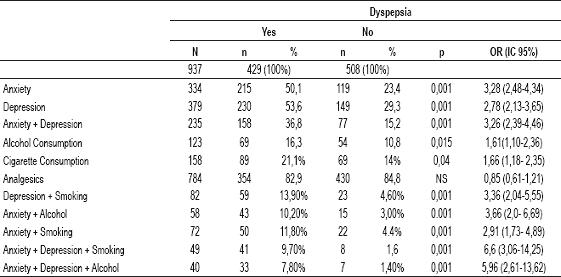
Cigarette, analgesics and alcohol consumption: 17.2% of the participants in the survey consumed cigarettes. Consumption was higher among men (25.9%) than among women (11.3%) p=0.001. It was also higher among participants of higher socioeconomic status (24.3%) than among participants of lower socioeconomic status (10.2%) p=0.001, and higher among those between 18 and 20 years of age (33.9%), p=0.001, than among younger participants. The use of cigarettes was statistically higher among those who have dyspepsia than among those who do not have dyspepsia or reflux (p=0.004) (Table 3).
Table 3. Dyspepsia in relation to consumption of cigarettes, alcohol, analgesics and emotional factors
Analgesic consumption was 83.9% among participants in the survey, with no association to the presence of dyspepsia. The most frequent causes for consumption of analgesics were dysmenorrhea and cephalea.
13.3% of survey participants consume alcohol. Consumption was higher among men (p=0.001), participants with higher socioeconomic status (p=0.001), and participants from 18 to 20 years of age (p=0.001). The statistically correlation with dyspepsia was significant (p=0.015).
Relationship with anxiety and depression
Corrected Zung questionnaire results for anxiety and depression (SDS) for the entire population studied (n=937) showed 35.6% with symptoms of emotional anxiety (slight 22.7%, moderate 8.3% and severe 4.6%), 40.3% with symptoms of depression (slight 30.4%, moderate 7.4% and severe 2.5%), and 25.1% with symptoms of both anxiety and depression.
50.1%, of the adolescents with dyspepsia had anxiety symptoms, 53.6% had symptoms of depression, and 36.8% had symptoms of both anxiety and depression. This is in contrast to healthy students, 29.3% of whom had anxiety symptoms, 23.4% of whom had symptoms of depression, and 15.2% of whom had symptoms of both (p=0.001)) (Table 3).
The frequency of dyspepsia was higher (p=0.001) among youth with anxiety and depression symptoms than among those without these emotional symptoms.
There were anxiety, depression and anxiety + depression symptoms in 61.9%, 46.8% and 41.3% of the youths with reflux compared with 33.8%, 33.9% and 23.9% in healthy students (p=0.001,NS and 0.002 respectively) (Table 4).
Table 4. Reflux in relation to consumption of cigarettes, alcohol, analgesics and emotional factors.
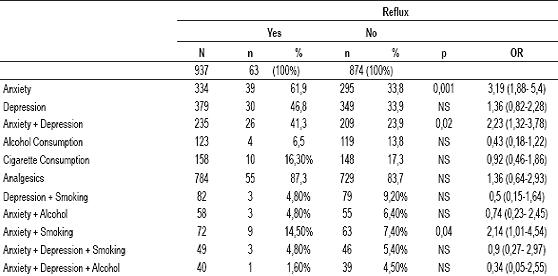
The association of anxiety and/or depression with consumption of cigarette and alcohol showed an increased risk of dyspepsia (Table 3). The presence of anxiety, anxiety plus depression and anxiety plus cigarette consumption showed an increased risk of reflux (Table 4).
No statistically significant differences were found between the frequencies of anxiety and depression among those suffering from organic dyspepsia and those suffering from functional dyspepsia, hence, anxiety and depression have been related to the presence of dyspepsia, but not broken down by type (i.e. organic or functional) (Table 5). Although a high OR was found in the comparison of organic dyspepsia with the presence of anxiety and depression, and with the presence of anxiety, depression and alcohol consumption, it was not enough to be statistically significant. This could be due to lack of association, or it could be due to insufficient sample size.
Table 5. Type of dyspepsia in relation to consumption of cigarettes, alcohol, analgesics and emotional factors.
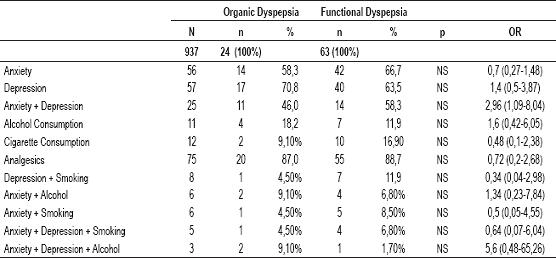
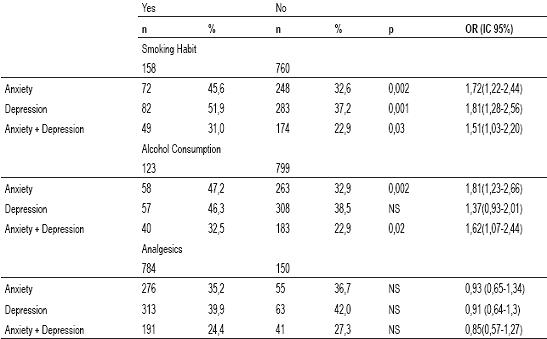
Cigarette consumption was found to be associated with anxiety; with depression; and with anxiety plus depression plus cigarette consumption. Alcohol consumption was found to be associated with anxiety and with anxiety plus depression, but not with depression alone. Analgesics consumption was not found to be associated in any statistically significant way with anxiety, depression or their combination (Table 6).
Table 6. Risk behaviors in relation to anxiety and depression.
Effect on education
Students were asked, "Have you had to stop attending school or university due to previous discomforts?" 40.1% of the youth with dyspepsia and 41.3% of the youth with reflux answered affirmatively.
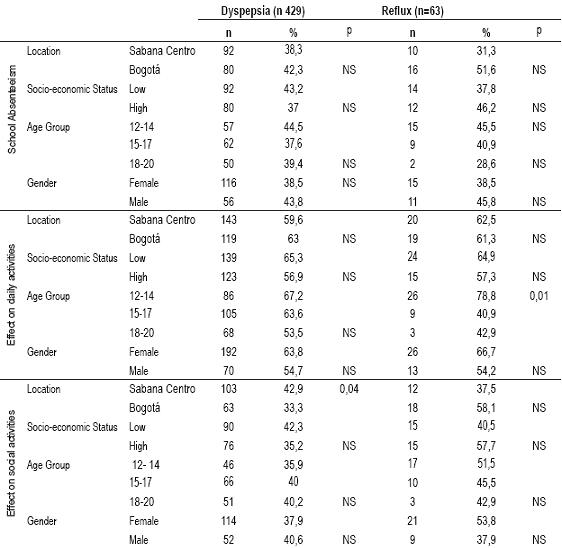
Comparing the absenteeism of adolescents diagnosed with "dyspepsia" and/or "reflux" with the absenteeism of youth with occasional symptoms there are statistically significant differences: p = 0.001 for dyspepsia and p= 0.02 for reflux. No statistically significant differences were found related to sex, age, socioeconomic status or location of the educational institution. There is no significant difference found between absenteeism associated with dyspepsia and that associated with reflux (p NS) (Table 7), nor were any significant differences found between absenteeism due to organic dyspepsia and that due to functional dyspepsia.
Table 7. Absenteeism from School and effects on social and daily activities among students with dyspepsia and reflux according to socio-demographic variables.
Effect on daily activities and social activity
The adolescents were asked, "Do you feel that the digestive symptoms you mentioned limit your daily activities?" and "Have you stopped going to parties and other social events due to the mentioned discomforts?"
We found that the associations between limitations on daily activities and dyspepsia and reflux were high and similar, 61.1% and 61.9%, respectively, with p=NS. There was a statistically significant difference between these limitations and those of youth who only had occasional symptoms (p = 0.001 for dyspepsia and 0.001 for reflux). No statistically significant differences were found relating to sex, age and location of the educational institution. However, youth from lower socioeconomic strata with dyspepsia had higher limitations in daily activities than did dyspeptic youth from higher socioeconomic strata (p = 0.001) (Table 7).
The presence of dyspepsia is associated with limitations of social activities (e.g. going to parties) in 38.7% of those affected, while the presence of reflux is associated with limitations of social activities 47.6% of those affected. There are statistically significant differences between these figures and those for youth who only had occasional symptoms (p = 0.001 for dyspepsia and 0.001 for reflux). No statistically significant difference was found in relation to this variable for sex, age or socioeconomic status (Table 7).
Discussion
Dyspepsia occurs frequently among both adults and adolescents (3, 4, 15, and 16). It entails high costs in health care services derived from primary and specialized medical care and diagnostic exams. Although its course is usually benign it can recur and interfere with individuals quality of life (7.8% severely, 4.8% slightly) (11).
Emotional factors such as anxiety and depression have been related to dyspepsia in children, adolescents and adults (3, 11, 17), but it is not clear if these factors are related to its physiopathology, its course of development, or to a predisposition to develop functional alterations (2).
In our previous publication we showed that 69.8% of the youth with reflux and 61.1% of the youth with dyspepsia relate the appearance of symptoms to alterations of emotional order. Most important are tests and academic difficulties, followed by family difficulties and relatives deaths. (4). Guz (21) reported frequencies of association of some psychiatric disorder in 44.7% and 50% of the people with or without an organic cause of dyspepsia, with no significant difference between the two groups (21).
Some studies report improvement in dyspeptic symptoms through various psychological interventions (15), although there is not enough evidence to recommend a specific treatment (19, 20).
Hyams considers that the biopsychosocial approximation should be used in the initial evaluation of children and adolescents with dyspepsia and recurrent abdominal pain (15, 22). This approach calls for a detailed medical history that not only includes questions about symptoms, but also asks about the psychological and social factors that surround the child or adolescent. The biopsychosocial model described for the pathogenesis of acid peptic disease proposes that high emotional stress, regardless of its cause, is related both to the origin and evolution of acid peptic disorders. This is due both to increases in the production of basal acid, and to the development of risky behaviors such as consumption of alcohol (9) and smoking of tobacco. Both decrease the speed of recovery for mucous injuries that involve lowering mucous defense mechanisms and facilitating infections and colonization of H pylori (6).
In this study of student populations 12 to 20 years of age, we found a high prevalence of symptoms suggestive of anxiety, depressive disorders, and combinations of the two (35.6%, 40.3%, and 25.1% respectively). In youth with dyspepsia these symptoms were even more frequent (p=0.001). In the case of reflux, the prevalence of symptoms of anxiety and a combination of anxiety and depression was significant. In Colombia, the national study of mental health in 2003 found a prevalence of anxiety at 19.3% and of depression at 8.6%. (23)
We found here that the symptoms of anxiety and/or depression increase the risk of smoking and consumption of alcohol, and that the consumption of cigarettes and alcohol is significantly more frequent among youth with dyspepsia. Furthermore we found that anxiety and/or depression alone and associated with consumption of cigarettes and alcohol show progressive increases in OR for dyspepsia (from 1.61 for cigarette consumption alone up to 6.6 for anxiety + depression + cigarette). In the case of reflux, only anxiety, anxiety plus depression and anxiety plus cigarette consumption showed significant differences.
We did not find significant differences in relation to the presence of anxiety, depression or cigarette and alcohol consumption with the type of dyspepsia. Although the OR for organic dyspepsia in anxiety + depression and anxiety + depression + alcohol are high, this result is related to the size of the sample and should be evaluated in specific clinical studies. This is especially true considering that anxiety and depression have been traditionally considered in relation to functional dyspepsia but not to organic dyspepsia (2, 12).
According the biopsychosocial model the presence of emotional factors are related to the development of risky behaviors that can cause a disease. This is supported by the evidence found in this study. We found that anxiety and depression are factors associated with consumption of cigarettes and alcohol and that the association between emotional factors and these habits increases the risk of dyspepsia.
Dyspepsia and reflux both have important impacts on adolescents when we consider their high frequency, their effects on school absenteeism, and their effects on the daily and social activities of these young people.
In this study we found that 40.1% of the students with dyspepsia and 41.3% of the students with reflux showed school absenteeism on some occasion due to these symptoms. We found that 38.7% of the youth with dyspepsia and 47.6% of the youth with reflux limited their social activities due to them, and that about 60% had their daily activities affected. In this study we found that 44.6% of the youth with reflux and 56.5% of the youth with dyspepsia had consulted a doctor for these conditions.
The reported prevalence in the literature on malignant pathologies for this age group is very low (4, 15, 22, 24). The frequency of duodenal ulcers and erosive esophagitis are both within the lower range of those reported for adults (4), but we can not forget that between a third and a half of adolescents with acid peptic disease may suffer melaenas or hematemesis, half of them after already having previous symptoms (25).
A proper evaluation, which considers all the factors involved and which searches for an integral approach to the adolescent with dyspepsia and his/her environment, will benefit his/her well being and the proper user of health resources. Close contact with the adolescent and his/her family core, the search for, and intervention into, associated emotional factors, proper monitoring and medical guidelines for identifying alarming signs and symptoms are essential to avoid serious complications and unnecessary studies.
Conclusions
1. The prevalence of dyspepsia and reflux is higher in adolescents with symptoms of anxiety and/or depression.
2. Anxiety and depression increase the risk of alcohol and cigarette consumption among adolescents and the association of these variables increases the risk of dyspepsia and reflux.
3. The quality of life of adolescents with reflux and dyspepsia is altered in important ways such as high absenteeism rates and adverse effects on the daily and social activities of these young people.
Acknowledgments
To the subcommittee of investigation of the Faculty of Medicine of Universidad de La Sabana and the patrimony fund for research in Universidad de La Sabana. To Dr. Rodolfo Dennis for his invaluable Epidemiologic support, to Dr. Jorge Lizarazo for his opportune appreciations and to all the students in the Faculty of Medicine and Social Communication who contributed in the different phases of this investigation.
References
1. Levenstein S. Stress and peptic ulcer: life beyond helicobacter. BMJ 1998; 316: 538-41.
2. Tack J, Talley N, Camillero M, et al. Functional gastrointestinal disorders. Gastroenterology 2006; 130: 1466-1479.
3. Rasquin A, Di Lorenzo C, Forbes D, et al. Childhood functional gastrointestinal disorders: Chil/adolescent. Gastroenterology 2006; 130: 1527-1537.
4. Jenny Molano Caro, Sandra Piñeros Ortiz, Clara López de Mesa Melo. Dispepsia y reflujo gastroesofágico en adolescentes escolarizados. Rev Col Gastroenterol 2008; 23: 46-56.
5. Levesnstein S. Psychologic predictors of duodenal ulcer healing. J Clin Gastroenterol 1996; 22: 84-89.
6. Holtmang G. Influence of stress in healing and relapse of duodenal Ulcers Scand J Gastroenterol 1992; 27: 917-923.
7. Zung WK. A rating instrument for anxiety disorders. Psychosomatics. 1971; 12: 371-379.
8. De La Cruz D, Mariano L. Prevalencia de síntomas depresivos en estudiantes de 11 del Colegio Comfenalco de Cartagena. Cartagena: Universidad Tecnológica de Cartagena. 2000.
9. Rodríguez DC, Dallos CM, González SJ, Sánchez Z, Martínez L, Rueda G, Campo-Arias A. Asociación entre síntomas depresivos y consumo abusivo de alcohol en estudiantes de Bucaramanga, Colombia. Cad Saúde Pública, Río de Janeiro 2005; 21 (5): 1402-1407.
10. Lichtenstein DR, Syngal S, Wolfe MM, Nonsteroidal antiinflammatory drugs and the gastrointestinal tract: the double-edged sword. Arthritis Rheum 1995; 38: 5-18.
11. Grupo de trabajo de la guía de práctica clínica sobre dispepsia. Manejo del paciente con dispepsia. Guía de práctica clínica. Barcelona: Asociación Española de Gastroenterología, Sociedad Española de Medicina de familia y comunitaria y centro Cochrane Iberoamericano, 2003, programa de elaboración de guías de práctica clínica de enfermedades digestivas desde la atención primaria especializada: Barcelona, febrero 2003. p. 1-92. http://www.cochrane.es
12. NJ Talley, V Stanghellini, R C Heading, K Koch, JR Malagelada, GN Tytgat. Functional gastroduodenal disorders. Gut 1999; 45(Suppl II): II37-II42.
13. Talley NJ, M Silverstein, et al. AGA technical review: evaluation of dyspepsia. American Gastroenterological association. Gastroenterology 1998; 114: 582-559.
14. Talley NJ, Dyspepsia: Management guidelines for the millennium. Gut 2002; 50 (S IV): 72- 78.
15. Hyams JS, Davis P, Sylvester FA, Zeiter DK, Justinich CJ, Lerer T. Dyspepsia in children and adolescents: a prospective study. J pediatr Gastroenterol Nutr 2000; 30: 413- 418.
16. Hyams JS, Hyman PE. Recurrent abdominal pain and irritable bowel syndrome in adolescents: A community based study. J Pediatr 1996; 129: 220-226.
17. Tack J, Talley N, Camilleri M, et al. Functional gastroduodenal disorders. Gastroenterology 2006; 130: 1466-1479.
18. Hamilton J, Guthrie E, Creed F, et al. A randomized controlled trial of psychotherapy in patients with chronic functional dyspepsia. Gastroenterology 2000; 119: 661-669.
19. Soo S, Forman D, Delaney B, et al. A systematic review of psychological therapies for nonulcer dyspepsia. Am J Gastroenterol 2004; 99: 1817-1822.
20. American Gastroenterological association technical review on evaluation of dyspepsia. Gastroenterology 2005; 129; 1756-1780.
21. Guz H, Tevfik A, Bektas A, Doganay Z. The frequency of the psychiatric symptoms in the patients with dyspepsia at a university hospital. General Hospital Psyquiatry 2008; 30: 252-256.
22. Hyams J, Hyman P. Recurrent abdominal pain and the biopsychosocial model of medical practice. J Pediatr 1998; 133: 473-478.
23. Posada J, Aguilar-Gaxiola S, Magaña C. Prevalencia de trastornos mentales y uso de servicios: Resultados preliminaries del estudio nacional de salud mental. Colombia 2003. Rev Colomb Psiquiatr 2004; 33: 241-62.
24. McGill TW, Downey EC, Westbrook J, Wade D, et al. Gastric carcinoma in children. J pediatr surg 1993; 28(12): 1620-1621.
25. Murphy MS, Easthman EJ, Jiménez M. Duodenal ulceration: Review of 110 cases. Arch Dis Child 1987; 62: 554.
1. Levenstein S. Stress and peptic ulcer: life beyond helicobacter. BMJ 1998; 316: 538-41. [ Links ]
2. Tack J, Talley N, Camillero M, et al. Functional gastrointestinal disorders. Gastroenterology 2006; 130: 1466-1479. [ Links ]
3. Rasquin A, Di Lorenzo C, Forbes D, et al. Childhood functional gastrointestinal disorders: Chil/adolescent. Gastroenterology 2006; 130: 1527-1537. [ Links ]
4. Jenny Molano Caro, Sandra Piñeros Ortiz, Clara López de Mesa Melo. Dispepsia y reflujo gastroesofágico en adolescentes escolarizados. Rev Col Gastroenterol 2008; 23: 46-56. [ Links ]
5. Levesnstein S. Psychologic predictors of duodenal ulcer healing. J Clin Gastroenterol 1996; 22: 84-89. [ Links ]
6. Holtmang G. Influence of stress in healing and relapse of duodenal Ulcers Scand J Gastroenterol 1992; 27: 917-923. [ Links ]
7. Zung WK. A rating instrument for anxiety disorders. Psychosomatics. 1971; 12: 371-379. [ Links ]
8. De La Cruz D, Mariano L. Prevalencia de síntomas depresivos en estudiantes de 11 del Colegio Comfenalco de Cartagena. Cartagena: Universidad Tecnológica de Cartagena. 2000. [ Links ]
9. Rodríguez DC, Dallos CM, González SJ, Sánchez Z, Martínez L, Rueda G, Campo-Arias A. Asociación entre síntomas depresivos y consumo abusivo de alcohol en estudiantes de Bucaramanga, Colombia. Cad Saúde Pública, Río de Janeiro 2005; 21 (5): 1402-1407. [ Links ]
10. Lichtenstein DR, Syngal S, Wolfe MM, Nonsteroidal antiinflammatory drugs and the gastrointestinal tract: the double-edged sword. Arthritis Rheum 1995; 38: 5-18. [ Links ]
11. Grupo de trabajo de la guía de práctica clínica sobre dispepsia. Manejo del paciente con dispepsia. Guía de práctica clínica. Barcelona: Asociación Española de Gastroenterología, Sociedad Española de Medicina de familia y comunitaria y centro Cochrane Iberoamericano, 2003, programa de elaboración de guías de práctica clínica de enfermedades digestivas desde la atención primaria especializada: Barcelona, febrero 2003. p. 1-92. www.cochrane.es [ Links ]
12. NJ Talley, V Stanghellini, R C Heading, K Koch, JR Malagelada, GN Tytgat. Functional gastroduodenal disorders. Gut 1999; 45(Suppl II): II37-II42. [ Links ]
13. Talley NJ, M Silverstein, et al. AGA technical review: evaluation of dyspepsia. American Gastroenterological association. Gastroenterology 1998; 114: 582-559. [ Links ]
14. Talley NJ, Dyspepsia: Management guidelines for the millennium. Gut 2002; 50 (S IV): 72- 78. [ Links ]
15. Hyams JS, Davis P, Sylvester FA, Zeiter DK, Justinich CJ, Lerer T. Dyspepsia in children and adolescents: a prospective study. J pediatr Gastroenterol Nutr 2000; 30: 413- 418. [ Links ]
16. Hyams JS, Hyman PE. Recurrent abdominal pain and irritable bowel syndrome in adolescents: A community – based study. J Pediatr 1996; 129: 220-226. [ Links ]
17. Tack J, Talley N, Camilleri M, et al. Functional gastroduodenal disorders. Gastroenterology 2006; 130: 1466-1479. [ Links ]
18. Hamilton J, Guthrie E, Creed F, et al. A randomized controlled trial of psychotherapy in patients with chronic functional dyspepsia. Gastroenterology 2000; 119: 661-669. [ Links ]
19. Soo S, Forman D, Delaney B, et al. A systematic review of psychological therapies for nonulcer dyspepsia. Am J Gastroenterol 2004; 99: 1817-1822. [ Links ]
20. American Gastroenterological association technical review on evaluation of dyspepsia. Gastroenterology 2005; 129; 1756-1780. [ Links ]
21. Guz H, Tevfik A, Bektas A, Doganay Z. The frequency of the psychiatric symptoms in the patients with dyspepsia at a university hospital. General Hospital Psyquiatry 2008; 30: 252-256. [ Links ]
22. Hyams J, Hyman P. Recurrent abdominal pain and the biopsychosocial model of medical practice. J Pediatr 1998; 133: 473-478. [ Links ]
23. Posada J, Aguilar-Gaxiola S, Magaña C. Prevalencia de trastornos mentales y uso de servicios: Resultados preliminaries del estudio nacional de salud mental. Colombia 2003. Rev Colomb Psiquiatr 2004; 33: 241-62. [ Links ]
24. McGill TW, Downey EC, Westbrook J, Wade D, et al. Gastric carcinoma in children. J pediatr surg 1993; 28(12): 1620-1621. [ Links ]
25. Murphy MS, Easthman EJ, Jiménez M. Duodenal ulceration: Review of 110 cases. Arch Dis Child 1987; 62: 554. [ Links ]

