











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink
Introduction
Arterial Hypertension (AH) is considered a serious health problem worldwide as it is the main modifiable risk factor for circulatory system diseases1 and, due to their high prevalence, especially in low and middle-income countries2 . Among these, Brazil experienced an increase in annual death rates reaching 21.4% of its population3 . Due to this morbidity and mortality, adherence to appropriate treatment, which is the primary mode for controlling the AH, is still a major challenge1 , 4 .
In 2003, the World Health Organization defined adherence as a person's commitment to maintaining medication and diet or changes in lifestyle habits, according to recommendations of a health professional5 . Therefore, adherence involves drug treatments or not.
Regarding drug adherence in people with AH, this is a complex and multifactorial process that may be influenced by factors related to lack of blood pressure control6 , to the socio-demographic profile, to the disease, to the patient, to the health professional, to the relationship between the health professional and the patient, to the treatment, to the health service, to the use of substances, to social problems7 and cultural aspects8 .
In this regard, researchers have emphasized the need for further studies on antihypertensive drug adherence that takes into account, among other factors, the culture 8 and the race9 . Thus, the development of these studies in the black population is urgent, since it is more affected by AH in relation to the other races10 .
In the national territory, the black ancestry population, which includes people who declared themselves black and mulattos11 , has a high AH prevalence12 . Among this population, the most prominent are the people living in quilombola communities that show, in addition to their own ethnic-racial identity13 , a significant level of social vulnerability14 , poor housing conditions15 and difficulties in accessing health services16 , which may compromise adherence to antihypertensive treatment.
In general, quilombola communities are located in rural areas and the few studies that involve the identification of their health conditions are concentrated in these localities14 , 17 . Therefore, studies aimed at investigating drug adherence and its associated factors in hypertensive quilombola people12 , are incipient, especially in the urban quilombola community.
The identification of drug adherence and associated factors is relevant, and its analysis in different regional contexts18 can provide subsidies for health professionals, researchers and managers in formulating public policies to reverse this health problem (AH) and in creating interventions that may come to promote the health of these people and increase the adherence rates4 .
Therefore, the study’s objective is to identify adherence to drug treatment and the associated factors, socio-demographic and health aspects, in hypertensive individuals, living in urban quilombola community.
Materials and methods
This is a analytical cross-sectional, community-based census study conducted in the community of Barro Preto, located in the urban area of Jequié-BA (Brazilian northeast), within the Family Health Strategy (FHS) scope area, where black and hypertensive people reside, and who are remaining quilombola people.
Data collect occurred between November 2017 and March 2018. Inclusion criteria were as it follows: being between 35 and 79 years old; self-declared as a quilombola resident, mulatto or black people; residing in the studied community; being enrolled in the FHS in their territory and have the medical AH diagnosis recorded in a medical record. People who were not located after three home visits at distinct days and times were excluded, those with incomplete questionnaire data, and that moved away from the community were also excluded.
In the FHS records there were 483 people registered in HiperDia. In order to carry out the survey on the people enrolled in the FHS of the studied quilombola community, a search was accomplished on Sheet A of the family history record, with 400 hypertensive people being foun that met the eligibility criteria. However, through home visits, 89 people were not found, 4 moved away and 5 had incomplete questionnaires, resulting in 302 people.
The interview technique was used for applying the instruments, starting with the AH form, that is routinely used in this FHS and containing the independent variables related to socio-demographic data (age, gender, marital/family status, schooling, race/color, occupation and family income) and health aspects (comorbidity, lifestyle and anthropometric index) evaluated in this study. The pilot test was not accomplished, since it is a standard form in the health service where the study was accomplished.
Then, to evaluate drug adherence, a variable dependent on this study, the participants responded to the Morisky Drug Adherence Scale (MMAS-8), validated19 , 20 and used in other Brazilian studies7 . The questionnaire contains eight questions and the possible answers are “yes” and “no”. For each “no” answer, 1 point is added. At the end of the summation, the adherence classification is obtained in three levels: high (score 8), mean (score 6 and 7) and low (score <6) values. In this study, those participants with scores equal to or greater than 6 in the MMAS-8 and non-adherent ones whose final score was less than 619 .
Data arising from the collect were tabulated in the software Statistical Package for the Social Sciences (SPSS) 21.0. The analysis was accomplished from descriptive statistics, using median (Q1-Q3) for continuous variables and absolute and relative frequency for the categorical variables. For the bivariate analyses of the categorical variables, the chi-square test was used and, for the continuous tests the Mann-Whitney test was used.
Variables that presented p <0.2 in the bivariate analyzes were included in a multivariate logical regression model, with a backward method. The results were then expressed in Odds Ratio (OR) and their respective 95% confidence intervals with and without adjustment. For all analyzes, the final level of significance was 5% (p<0.05).
This study complies with Resolution 466/2012 of the National Health Council, and is approved by the Research Ethics Committee of Faculdade Independente do Nordeste (FAINOR), with written opinion No. 2.015.327 and CAAE No.: 66705617.2.0000.5578. All the participants in this study were informed about the study by reading the Free and Informed Consent Term, and the research was accomplished only after their understanding, agreement and signature.
Results
Among the evaluated hypertensive individuals, the prevalence of adherence to drug treatment was 62.9%. Age ranged from 26 to 79 years old, with a median of 60 years old (Q1-Q3: 52.0-69.0). When evaluated between the groups (that is, adherent or non-adherent), the median age of the adherent group was 62 years old (55.0-71.0), while the non-adherent age was 55.5 years old (48.0-66.0), with differences between groups being statistically significant (p <0.001).
Regarding the socio-demographic variables, there was predominance among the female gender (67%). Regarding the educational level, it was verified that the participants with less than one year of schooling adhered more to antihypertensive drugs (70.6%). Regarding race/skin color, 63.4% of black hypertensive individuals (including mulattos) adhere to the medication. As for the marital and family situation, 91% of the people who adhere to the treatment live with a partner or with other relatives (consanguineous or not). It is observed that there was greater adherence in people receiving income less than or equal to one minimum wage (62.7%), retired (66.7%) and not working (65.4%). This characterization is found in Table 1 .
Table 1 Socio-demographic characteristics of hypertensive Afrodescendants resident in Quilombola community in relation to drug adherence. Jequié, BA, Brazil, 2018.
| Characteristics | Drug Adherence* | ||
|---|---|---|---|
|
|
|||
| No n (%) | Yes n (%) | P | |
| Gender (n= 302) | 0.002* | ||
| Male | 41 (47.1) | 46 (52.9) | |
| Female | 71 (33.0) | 144 (67.0) | |
| Schooling (n=302) | 0.062 | ||
| < 1 year of schooling | 37 (29.4) | 89 (70.6) | |
| From 1 to 8 years of schooling | 61 (42.4) | 83 (57.6) | |
| > 8 years of study | 14 (43.8) | 18 (56.3) | |
| Race/color (n=302) | 0.615 | ||
| Black people | 100 (36.6) | 173 (63.4) | |
| Not black people | 12 (41.4) | 17 (58.6) | |
| Marital/family status (n= 302) | 0.180 | ||
| Has a partner | 74 (41.3) | 105 (58.7) | |
| With other relatives Live alone | 30 (31.3) 8 (29.6) | 66 (68.8) 19 (70.4) | |
| Income (n=278) | 0.927 | ||
| < one wage | 82 (37.3) | 138 (62.7) | |
| > one wage | 22 (37.9) | 36 (62.1) | |
| Occupation (n=302) | |||
| Works | 76 (38.4) | 122 (61.6) | 0.934 |
| Does not work | 28 (34.6) | 53 (65.4) | |
| Retired | 3 (33.3) | 6 (66.7) | |
| Others | 5 (35.7) | 9 (64.3) | |
SOURCE: research data. *divergences between the totals of each category are due to non-responses
Regarding the health aspects, the median of systolic blood pressure (SBP) was 147mmHg, while diastolic blood pressure (DBP) 85mmHg. When comparing systolic SBP and DBP between the groups (adherent and non-adherent), both SBP and DBP in the non-adherent group were higher, as shown in figure 1 .
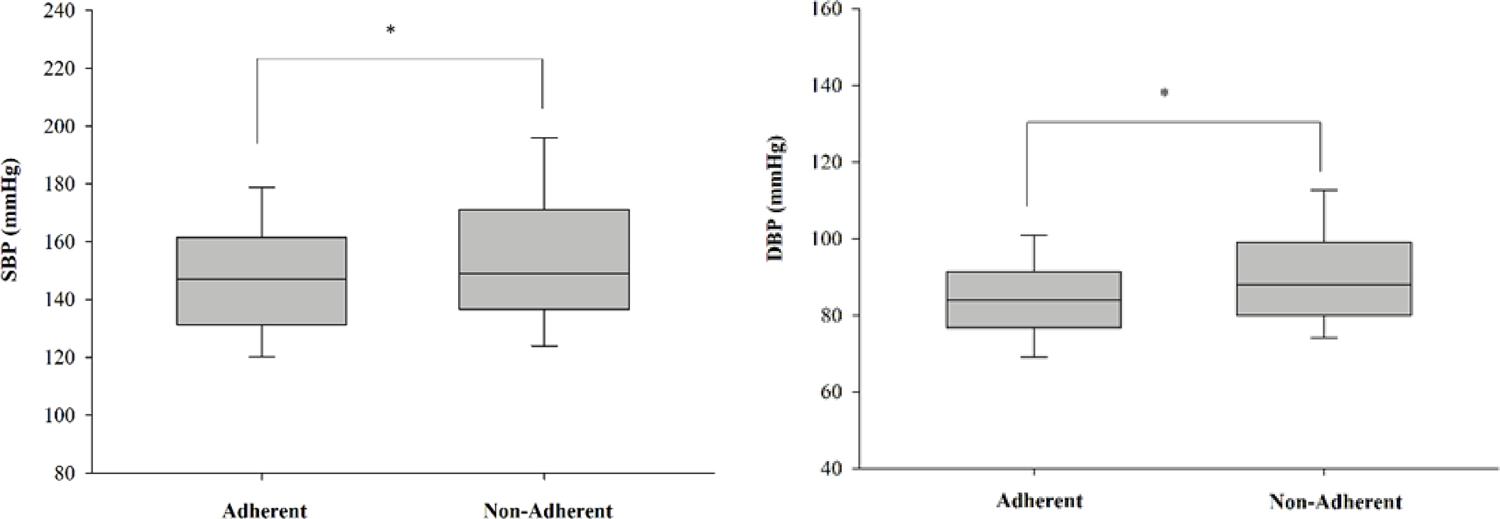
SOURCE: research data. *Statistically significant difference to SPB (p= 0,007) and DPB (p= 0,002).
Figure 1 Median and interquartile range of systolic (SBP) and diastolic (DBP) blood pressure between adherent and non-adherent individuals. Jequié, 2018.
Hypertensive drug users who reported type 2 diabetes (67.1%) and had a family history of cardiovascular disease (CVD), who did not smoke (63.7%) and did not practice physical activity (64, 7%) ( Table 2 ).
Table 2 Health aspects for hypertensive Afrodescendants resident in Quilombola community in relation to pharmacological adherence. Jequié, BA, Brazil, 2018.*
| Characteristics | Pharmacological adherence | |
|---|---|---|
|
|
||
| No n (%) | Yes n (%) | |
| CVD family history (n=271) | ||
| Yes | 55 (32.7) | 113 (67.3) |
| No | 42 (40.8) | 61 (59.2) |
| T2 diabetes (n=220) | ||
| Yes | 23 (32.9) | 47 (67.1) |
| No | 57 (38.0) | 93 (62.0) |
| Smoking (n=302) | ||
| Yes | 13 (46.4) | 15 (53.6) |
| No | 99 (36.1) | 175 (63.9) |
| Sedentary life-style (n=302) | ||
| Yes | 53 (34.9) | 99 (65.1) |
| No | 59 (39.3) | 91 (60.7) |
| Categories of BMI (n=298) | ||
| Not overweight | 24 (35.3) | 44 (64.7) |
| With overweight | 87 (37.8) | 143 (62.2) |
SOURCE: research data. BMI = Body Mass Index; CVD = Cardiovascular Disease. *divergences between the totals of each category are due to non-responses
The final logistic regression model is shown in Table 3 , and it was observed that age was a protective factor for adherence (that is, increased age improved adherence), as well as, the female gender. On the other hand, systolic pressure was shown to be a risk factor for adherence (that is, higher systolic pressure values imply worse adherence).
Table 3 – Odds Ratio (OR) with and without adjustment, and confidence interval 95% of final logistic regression model for pharmacological adherence. Jequie, BA, Brazil, 2018.
| Characteristics | OR (95% CI) | Adjusted OR* (95% CI) | ||
|---|---|---|---|---|
| Age | 0,962 (0.963-0.991) | 0.954 (0.933-0.975) | ||
| SBP | 1,000 (0.995-1.023) | 1.118 (1.003-1.023) | ||
| Female Gender | 0.504 (0.290-0.894) | 0.497 (0.292-0.846) | ||
SOURCE: research data. Systolic Blood Pressure. *Variables on saturated model were: SPB, DBP, Age, gender and schooling
Discussion
In the results of this study, being older and being female are factors associated with greater drug adherence, while increases in SBP are linked to poorer adherence, which highlights that biological and behavioral variables are involved in the therapeutic adherence model.
Drug adherence among hypertensive individuals in this study (62.9%) was lower than the Brazilian mean value (81.4%)21 . When comparing the adherence rate in our study with other national geographic scenarios, it is verified that other cities in the Northeast displayed lower results19 , 22 , with percentages varying from 19.7% in Maceió-AL to 26.75% in Teresina-PI. However, research in the Southeast23 , 24 and South regions25 have higher adherence rates: 90,7%, 70,7% and 65,7%. Probable explanations for the divergent percentages refer to using different drug adherence scales26 .
In other African black populations, such as those living in Ghana, Nigeria27 and Nedjo28 , there are lower adherence rates than those in our study, 33.3% and 31.4%, being related to the use of medicinal herbs (cultural factor), low knowledge about AH and access to drug treatment. Probably, the most frequent contact of hypertensive quilombola people in study with the urban community and the health service has reduced this cultural belief and increased the confidence and the attitudes in the drug treatment.
The majority in the studied population belongs to the female gender, as well as data from other studies developed in Brazil29 , 30 and abroad27 , which demonstrates a greater demand in this group for health services, thus facilitating AH diagnosis and treatment31 . In Brazil, this data may be related to the culture of larger female participation in the developed health actions, especially in the FHS.
Unlike previous searches24 , 29 , 32 , in this study the female gender displayed statistical association and it was shown as a protection factor, which contradicts the hypothesis of drug adherence not being influenced by the gender33 .
Regarding age, other studies are in agreement with the results found in this study, showing that drug adherence is associated with increased age, being more frequent in the elderly (age greater than or equal to 60 years old)18 , 27 , 34 in relation to people aged between 20 and 59 years old35 .
The concern with comorbidities or complications experienced by AH36 and the presence of a caregiver may favor the adherence in the elderly. In adults and young people, asymptomatology or little health concern may come to impair this adherence27 . Therefore, health education actions for the younger age group are imperious.
Other authors14 , 17 have already documented low schooling in quilombola hypertensive individuals, but did not associate it with drug adherence. In this study, although the results were not statistically significant, the hypertensive individuals who adhered to the treatment had lower educational level. This is an inverse relation to the other searches23 , 18 , who have identified the low schooling reflected in the lower drug adherence, since it is a limiting factor in understanding the disease and the prescribed treatment30 . The categorization of schooling adopted in this research (in schooling years) differs from the cited investigations regarding the cut-off point and other heterogeneous categorizations, thus requiring caution in the interpretations.
Regarding financial situation, the literature shows that higher income is associated with better pharmacological adherence24 , 35 , which reflects in reducing pressure-related levels. However, a systematic review has pointed out that isolated income analysis may not be the deciding factor for drug adherence37 .
Although the hypertensive individuals in this study have low income, a similar situation to other black quilombola populations14 or not27 , it is likely that other factors such as free drug accessibility and treatment sensitization may have overlapped the income’s variable influence, thus increasing pharmacological adherence in this population.
The World Health Organization defines hypertensive people as those with a systolic blood pressure (SBP) equal to or greater than 140 mmHg and/or diastolic blood pressure (DBP) equal to or greater than 90 mmHg.1 In this study there was a greater reduction in SBP and DBP in the group with greater drug adherence, culminating in controlling pressure levels, similar to other studies25 , 26 , 27 , 33 , 34 .
A national study on the politics in the black population in the state of Maranhão distinguishes that the main challenges faced in AH control correspond to the lack of training for the professionals, use of inadequate therapeutic protocols and irregular drug distribution by the Unified Health System38 .
On the other hand, an international survey showed that the increase in AH control was related to addressing these challenges, in addition to applying other measures such as case management in high-risk patients, regular annual consultation, health education, graduated professionals that perform an active search for non-adherent patients by encouraging them to make appointments at the doctor39 .
The measures cited in this study are foreseen in the planning and execution of the national health services in the basic units, except for the active search that is not accomplished by a qualified health professional. The orientation of these professionals, especially nurses, has been associated with greater drug adherence40 , 41 , whereas guidance from community health agents may increase the odds for non-adherence to antihypertensive medication by up to 2.21 times24 .
Regarding the race/skin color variable, this study’s outcomes identify that - although most of the hypertensive individuals are black and mulattos, which may be associated with the studied population group (quilombola people) - there was no significant association with the pharmacological adherence for this variable. An opposing result for this relationship was found in a national study conducted in Paraná-Santa Catarina42 , when identifying that the majority of hypertensive individuals, who were white (70%), displayed statistically significant results for a greater adherence.
The isolated association for the race/skin color variable on drug adherence has been little cited in studies in Brazil33 , 43 and abroad44 . Thus, a deepening in the studies about the relation of the race/skin color variable with drug adherence needs to be developed in order to set up a consensus among the researchers.
Regarding marital and family situation, the results of this research converge with other studies, showing that the motivation offered by cohabiting with a partner26 or other relatives33 favors drug adherence, and that there may be a significant positive association between these two variables (living with a partner and drug adherence)23 . In this way, the family can act as an agent facilitating drug adherence by encouraging self-care practices45 .
The relationship of drug adherence to previous diseases such as type 2 diabetes34 and family history of cardiovascular disease29 , has also been documented in other researches. Probably, the presence of other comorbidities, in addition to hypertension, induces health professionals to devote greater attention to this population, which may result in better rates of pharmacological adherence.
The group of retired and non-working hypertensive individuals displayed greater drug adherence, as already observed in other studies26 , 43 . Free time to participate in educational activities and consultations may have influenced this adherence. Among workers, low adherence may be related to compliance with labor standards, influencing them to give up health care, such as forgetting to take medications or delaying their administration46 and the inflexibility regarding operational hours for the basic health units47 . Therefore, it is essential to adapt schedules, both in the functioning of health services, and in drug prescription.
The variables related to lifestyle were smoking and sedentarism. Among the adherents, those hypertensive people who do not smoke or are ex-smokers prevail, similarly to other studies29 , 43 , 46 . The actions of health education, personal aspects or complications in the clinical setting may have influenced the abandonment or non-initiation of the addiction.
Regarding sedentarsim, our results converge with other studies when identifying that hypertensive individuals with sedentary behavior adhere more to the pharmacological treatment34 , 43 , which may be related to the challenge in changing life habits48 and the difficulty for beginning regular physical activity practices. This data reinforces the importance of health interventions and actions to stimulate the adoption of a healthy lifestyle6 . The combination of physical exercise and pharmacological treatment can improve blood pressure levels49 , 50 and quality of life for hypertensive people.
In this study, greater pharmacological adherence was observed among eutrophic hypertensive individuals, culminating with a better blood pressure level34 . An opposing result was found in the Northeast region by showing that people with AH who adhered to the drug therapy were dystrophic51 . The divergence of this result can be related to household activities and manual work practiced by quilombola women and men, causing caloric and BMI reduction.
This research has limitations related to the absence of a control group and to the selection bias, since most information was self-reported, which does not allow us to make generalizations regarding adherence to the treatment of quilombola hypertensive individuals registered in other services or geographic areas.
The adherence to treatment of chronic conditions is a major challenge for public health and health workers, especially nurses. In this way, this study’s results show that health professionals need to design educational actions and interventions that help people living in the urban quilombola community to improve their adherence to drug therapy, aligning it with non-drug therapy, such as adopting healthy life habits that, therefore, promote greater control for blood pressure levels.
Conclusions
This study verified that adherence to drug treatment was lower when compared to the national average, although it was superior to other cities in the Northeast region of Brazil.
The profile og the users that adhered to hypertension treatment was characterized as being female, median age of 60 years old, having less than one year of schooling, living with someone (partner or other relatives), having a family income less than or equal to a one minimum wage, having type 2 diabetes and a CVD family history, not smoking, being sedentary, not overweight and having a controlled SBP. Of these variables, those with a statistically significant effect as protection factor were females and the increase of age and as, a risk factor, the increased levels of SBP in the non-adherent group.
The data demonstrated in this study is positive regarding drug adherence of black people to hypertension in the Northeast, which shows a modest increase in the participation of this population in public health programs. However, more investment is required in AH public control policies so that the adherence of this population may match the national average.
The results also reinforce the importance of incorporating motivational and diversified strategies focused on stimulating self-care to unify non-pharmacological treatment, such as physical activity practices, to pharmacological therapy. In addition, health promotion and prevention actions should consider the family core, social and cultural aspects, and encourage the empowerment of these people as active subjects for the change in their own reality.

