










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkInvestigación y Educación en Enfermería
versão impressa ISSN 0120-5307
Invest. educ. enferm vol.31 no.1 Medellín jan./abr. 2013
ORIGINAL ARTICLE / ARTÍCULO ORIGINAL/ ARTIGO ORIGINAL
Nursing work in care practice at Emergency Care Units in Porto Alegre/RS
Trabajo del enfermero en la producción del cuidado en Unidades de Urgencias de Porto Alegre-RS
Graciela Cabreira Gehlen1; Maria Alice Dias da Silva Lima2
1 RN, Ph.D., Professor. Instituto Federal do Paraná (IFPR), Brazil. email: graciela.gehlen@ifpr.edu.br.
2 RN, Ph.D., Professor. Universidade Federal do Rio Grande do Sul, Brazil. email: malice@enf.ufrgs.br.
Receipt date: June 22nd 2012. Approval date: September 19th 2012.
Article associated with the research: Technological Organization of Nursing Work in Care Practice at Emergency Care Units in Porto Alegre/RS.
Conflicts of interest: None.
How to cite this article: Gehlen GC, Lima MADS. Nursing work in care practice at Emergency Care Units in Porto Alegre/RS. Invest Educ Enferm. 2013;31(1): 26-35.
ABSTRACT
Objective. To characterize nurses' work process in care practice at Emergency Care Units. Methodology. The research technique used was mixed-method research. In the quantitative phase, a questionnaire was applied to 47 nurses; in the qualitative phase, a sample of events was observed at an emergency unit. Results. The activities the nurses most frequently developed were: a) care: risk assessment and classification (66%) and registering of clinical data (62%); b) management: task distribution (62%), shift organization (40%) data processing (36%), and material provision (28%). The nurses highlighted the users' forwarding to appropriate care levels as the goal of their work (70%). The work instruments most frequently used were clinical decision-making (87%), listening and monitoring (83%) and the risk assessment protocol (68%). Conclusion. Nurses' work at Emergency Units is predominantly focused on care, with a great burden of management activities related to resource planning and provision for care practice.
Key words: nursing services; emergency medical services; emergency relief; prehospital care; health services.
RESUMEN
Objetivo. Caracterizar el proceso de trabajo del enfermero en la producción del cuidado en Unidades de Emergencias. Metodología. La técnica investigativa utilizada fue la investigación de métodos mixtos. En la etapa cuantitativa se aplicó un cuestionario a 47 enfermeros; en la cualitativa, se realizó observación por muestreo de eventos en una unidad de emergencias. Resultados. Las actividades desarrolladas con mayor frecuencia por los enfermeros fueron: a) asistenciales: evaluación y clasificación del riesgo (66%) y el registro de datos clínicos (62%); b) gestión: distribución de tareas (62%), organización de cuadro de turnos (40%) diligenciamiento de datos (36%), y provisión de materiales (28%). La derivación de usuarios a niveles adecuados de atención fue resaltada por los enfermeros como finalidad de su trabajo (70%). Los instrumentos de trabajo más frecuentemente utilizados fueron la toma de decisiones clínicas (87%), la escucha y el acompañamiento (83%) y el protocolo de evaluación de riesgo (68%). Conclusión. El trabajo de los enfermeros en Unidades de Emergencias es predominantemente asistencial, pero tiene una gran carga de actividades de gestión relacionadas con la previsión y provisión de recursos para la producción del cuidado.
Palabras clave: servicios de enfermería; servicios médicos de urgencia; socorro de urgencia; atención prehospitalaria; servicios de salud.
INTRODUCTION
The Emergency Care Units (UPAs) are part of the health care system in Brazil, performing an important role as one of the immediate gateways for service users, through provision of initial treatment to clinical, surgical or trauma cases. Their purpose is to contribute in organizing the integral care networks for emergencies, which are responsible for caring for acute patients or acute chronic patients, with or without immediate risk of death, as defined by the National Policy on Emergency Care (PNAU).1 The purpose of these nurses' work, in conjunction with these units' health teams, is to stabilize the service users' clinical situation, carry out the initial diagnostic evaluation, and define the need (or not) for referral to more complex hospital services, as well as to receive non-urgent cases, proceeding to establish basic or specialized existing outpatient services in the healthcare network.1 In services which attend emergency situations, the nurses' work is related to the maintenance of the unit and participation in attending the service users, as well as coordinating the nursing team and assisting other health professionals.2 The nurses' work is interlinked with workers from the interdisciplinary team, sectors and services; they act in all the work fronts, in coordinating nursing activities, in linking, supervising and controlling the dynamics of the work in the service, in addition to identifying service users at higher risk.3 Nurses' work in these services has stood out as a consequence of the advance in their functioning, due as much to their knowledge and practice as to the space which this occupies in the production of care and organization of work. This results from the nursing actions being directly anchored in their underlying technical knowledge, and the striking presence of technical-scientific knowledge in the constitution of their practices, and in the organization of the work.
The nurses' technical-scientific knowledge and the uniqueness of each situation in these Emergency Care Units contribute effectively in the reorganization of the patient flow, establishing priority criteria with the aim of assisting all the service users in an integral way, within the possibilities of action/intervention. Bearing in mind the complexity and quality of the care given to the service users, this research sought to contextualize the technological organization of the nurses' work process in these units, considering the knowledge used for the carrying-out of the care. The study has as its guiding principle the theoretical interpretations identified in the literature concerning the work process in health and nursing,4,5 based on the understanding of what each element constituting the work process becomes: the object, the aim, the instruments and the knowledge which allow the operationalization of these instruments for the production of care. It is understood that the transformation of a specified object into a product occurs in the work process, through the intervention of the agent, who uses instruments to do so.6
Some authors have in common the interpretation that the nursing work process is characterized by being constituted by two inseparable dimensions: the carrying-out of nursing care actions, which represents the care dimension, and the actions directed at the agents of the work, the environment and the institution, which constitute the managerial dimension.7,8 The nurses are therefore involved in the management of the care, this referring to the managerial actions focused on the services' users or patients, that is, managerial actions linked to the care activities.7 Using this theoretical perspective, this article aims to characterize the nurses' work process in the production of care in Emergency Care Units.
METHODOLOGY
As its methodological strategy, this research used mixed methods, of the sequential explanatory type. Mixed methods research associates the quantitative and qualitative approaches, so that the study's general strength should be greater than that of qualitative or quantitative research in isolation.9 It is characterized by the collection and analysis of quantitative data through a questionnaire, followed by the phase of collection and analysis of qualitative data through event sampling observation. The quantitative approach permitted the analysis of the characteristics of the nurses' work process, and the qualitative approach made it possible to grasp the context and understand this work.
The study was undertaken in the four Emergency Care Units in Porto Alegre, which make up the Service Network dealing with emergencies in the municipality. The questionnaire was composed of 104 variables, structured in two parts: the first with 10 qualitative variables, identifying the profile of the subjects under study; and the second with 94 quantitative variables about the care activities and activities of prevention of harm to health, the care activities which contribute to the work of the team in emergency situations, and the management activities which shape the nurses' work. There were also questions about the purpose of the work, the instruments used in carrying out the work, the results of the work identified by the nurses, and the main difficulties in accomplishing the nurses' work in the Emergency Care Units. The questions required numerical (quantitative) responses, with alternatives structured by a Likert scale with pre-established priorities.10 Two scales were used for answers, expressing frequency and agreement, according to each question's content.
The questionnaire was prepared by the researcher, due to the non-availability of collection instruments validated for this object of study in the Brazilian and international literature. In order to prepare the questionnaire, a literature review was undertaken considering nurses' work in the emergency care services, including the aspects covered in the National Policy on Emergency Care1 and the elements that make up the work process. A pre-test was undertaken with four nurses from an Emergency Care Unit in another municipality in order to validate the questionnaire and ensure its internal consistency. The evaluation of the pre-test included the analysis of the proportion of responses which had not been understood by the respondents and the identification of answers shown to be difficult, ambiguous or badly-formulated, as well as important comments made by the respondents concerning the absence or excess of specific issues. Shortly afterwards, the questionnaire was revised and adjustments were made.
47 nurses responded to the questionnaire, representing 87.03% of the population under study; the questionnaire was administered between June and September 2010. The event sampling observation was undertaken in an Emergency Care Unit, selected in an intentional fashion, as its characteristics were compatible with the physical and organizational aspects and the aspect of the health services offered, proposed by the National Policy on Emergency Care. The observation was made between October and December 2010, shortly after the administration of the questionnaires. The nurses' activities were observed over a period of 58 hours, divided into 10 periods, recorded in a field diary.
The quantitative data was analyzed with descriptive statistics, using frequency tables. The program Statistical Package for the Social Sciences (SPSS) version 16.0 was used for the analyses, with the results being presented as absolute numbers, accompanied by the percentages. The qualitative data was treated using the technique of thematic content analysis,11 so as to identify the presence of specific issues which made up the record of the observations, and to interpret their meanings. In this way, the qualitative data was used to complement the understanding of the quantitative data, with the aim of combining the two approaches, given that the methodological structure adopted proposes the sequential format of data collection and analysis.
The ethical precepts referent to research involving human beings - established by Resolution 196/96 of the National Health Council -12 were taken into account, and were approved by the Research Ethics Committee of the Porto Alegre Municipal Health Secretariat. The people involved, and the units to which they belonged, were not identified, so as to preserve anonymity. All participants signed the Terms of Free and Informed Consent.
RESULTS
The quantitative and qualitative data were grouped, thus supplementing the data, and organized into four centers: the care dimension of the nurses' work; the managerial dimension of the nurses' work; the aim of the work; and, nurses' work instruments in the Emergency Care services.
The care dimension of the nurses' work in the emergency care units
The care activities cited by the nurses as most frequent in their work process were the reception with evaluation, and risk classification (31-66%) and the recording of clinical data in patient records (29-61.7%). In sequence, there is the verification of vital signs data and the testing of capillary blood glucose levels (24-51%). The carrying out of anamnesis and clinical evaluation of service users was evidenced at the same frequency (24-51.1%) followed by administration of medication (18-38.3%), the records of the care provision (18-38.3%) and the undertaking of an electrocardiogram test (17- 36.2%).
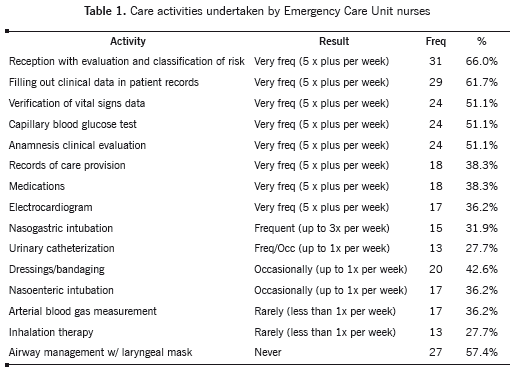
The significant presence of nurses' activity related to reception with risk evaluation and classification was confirmed by information obtained through observation of the events. Soon after filling out the initial attendance form at reception, the nurse attends a child accompanied by her mother, in the risk classification. The mother is questioned about the child's symptoms, and after the clinical evaluation, low oxygen saturation and signs of subclavicular depression were shown. The child was immediately referred to inhalation therapy, with a place being found for the mother and for the child to be while this was on-going. The classification - yellow - means that the child must only wait a few minutes to be attended. (OBS 10).
It was determined that the nurses from the emergency care units receive the service users, evaluating their complaints and needs and classifying the users according to the problems' level of seriousness. The nurse technician alerts the nurse that the classification of pediatric risk was behind schedule and that they should 'speed up' the process! The nurse started not to examine the service users, undertaking only the checking of vital signs and asking them why they had come to the service, with little dialog but plenty of technical ability (OBS9). Most of the time, however, during the episodes of observation of the work in this emergency care unit, it was identified that the nurses do not have the time to make a more detailed clinical evaluation, or to record it.
The managerial dimension of the nurses' work in the emergency care units
In the managerial dimension, it was identified that the activities of task distribution among the nursing team (29-61.7%), daily hours (23-48.9%), organization of nurse shift scheduling (19-40.4%) and filling out of reports referent to their work (17-36.2%) are undertaken with high frequency (more than five times per week) by the nurses in the Emergency Unit. The activities for provision of materials in the unit (13-27.7%) are carried out with a frequency of up to three times per week (Table 2).
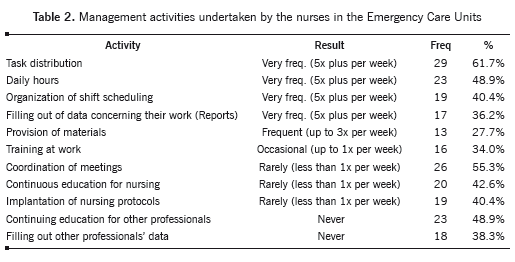
The observations demonstrate that the nurses use most of their time on task distribution activities, highlighted in Table 2: The nurse actions the SAMU service (SAMU: Mobile Emergency Service) to take some service users waiting for a space to be hospitalized. After the same have left, the nurse organizes the work of the unit's technicians, requesting the beds to be cleaned and disinfected, and organizing her team's activities regarding the other material and equipment to be organized in the unit (OBS6). It is identified that the care management actions indicated with frequency by the nurses - such as task distribution, daily staff hours, organization of monthly work shifts and provision of materials - are directed at the prediction and provision of resources for the production of care, through the organization and division of the nursing team's work.
The purpose of the work in the emergency care units in the conception of the nurses
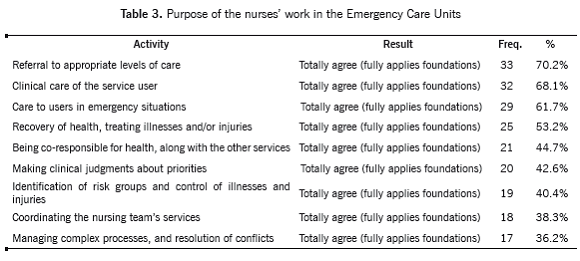
All the options offered as responses for the purpose of the work were indicated with full agreement by the nurses, with differing percentages. The nurses agree totally that the care given aims to refer the users on to appropriate levels of care, referent to referring within the service itself and to other services in the network (33-70%) as the main aim of their work in the emergency care units. In sequence, there is the clinical care of the service user (32-68.1%), care to users in emergency situations (29-61.7%), recovery of health through treating illnesses and/or injuries (25-53.2%), co-responsibility for people's health, in conjunction with the other services (21-44.7%), making clinical judgments about priorities (20-42.6%), identification of risk groups and control of illnesses and injuries (19-40.4%), coordinating the nursing team's services (18-38.3%) and managing complex processes and conflicts (17-36.2%) (Table 3).
During the observations, it was possible to identify a significant number of service users with acute complaints, who were attended and discharged, with the care being based on the needs brought by the service users, which are already modeled by the services offered at the unit. The service users are attended and are discharged or referred to other services for investigation or more complex actions, or further, to primary care services: The nurse responsible for the observation rooms, along with the unit's general coordinating nurse, seeks hospital bed spaces from the municipality's bed management center. She comments on the difficulty of finding beds, and emphasizes that there are service users in the observation room who have been waiting for over a week (OBS4). It was also identified that the nurses in the emergency care units use the factors related to the health needs - morbidity and seriousness -
for attending and assisting the service users, as the service they offer is emergency care.
The nurses' work instruments in the emergency care units
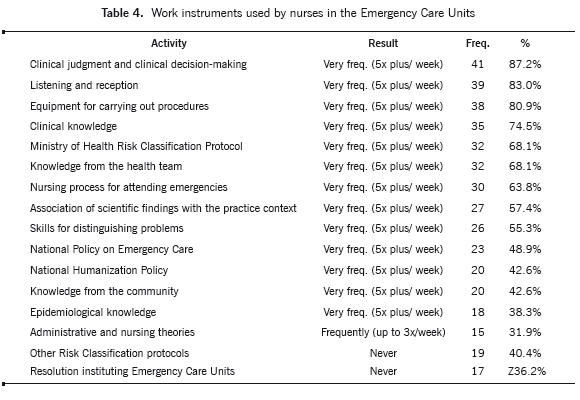
Clinical judgment and decision-making (41-87.2%) are the instruments used most frequently by the nurses, followed by listening and reception (39-83%); equipment for carrying out procedures (38-80.9%), clinical knowledge (35-74.5%), the protocol which guides the Ministry of Health's Risk Classification (32-68.1%), knowledge from the health team (32-68.1%), the nursing process for attending emergencies (30-63.8%), the association of scientific findings arising from studies with the practice context (27-57.4%) and the skills for distinguishing problems and identifying risks and injuries (26-55.3%). Moreover, among the instruments used very frequently are the guidelines of the National Policy on Emergency Care (23-48.9%), the National Humanization Policy (20-42.6%), knowledge from the community (20-42.6%) and epidemiological knowledge (18-38.3%) (Table 4).
The passages below describe the use of these instruments in everyday work: During a risk classification attendance, the nurse classifies a child with respiratory distress and fever as 'green' [meaning that the patient shall be seen in order of arrival]. Soon after, the nurse was called to the waiting area to see to the same child, who had progressed to compromising of the airways, it being necessary to move the child to the emergency room, due to the risk of respiratory arrest (OBS4).
The observations describe the magnitude of the nurses' decisions in the undertaking of teamwork in the emergency care. It is verified that the nurse's clinical judgment is alert to the team's procedures, and seeks to resolve the problems diagnosed, through referrals based in clinical decision-making, directing the patient flow within the service.
DISCUSSION
The commitment to clinical evaluation in reception, with the evaluation and classification of risk, for prioritization of attendance according to the clinical presentation, coincides with the results reported in the literature. The reception with evaluation and classification of risk is considered by the nurses to be a new model for reorganizing the service, consisting of attending the service users, assessing their complaints and needs, and classifying them for attendance according to the degree of severity.13 According to the results obtained, however, it is noteworthy that it was strictly the clinical needs that were identified, showing an association exclusively with the biomedical needs, as the nurse's decision for risk classification is based in the body's biological dysfunctions, with unease and anxiety not being considered as urgent demands. It is ascertained that the nurses are attentive to the people who go to the services, with the aim of prioritizing attendance according to clinical indication, the degree of suffering and the potential for risk of death.
The nurse stands out as the professional who is most skilled in carrying out risk classification, as she has theoretical-practical knowledge and greater experience with signs and symptoms, but not with diagnosis, and in addition is involved with the public policies and with the organization of the workplace.13 The functioning of the nurse in the job of reception and risk classification permits better management of emergency services, as it contributes to ensuring the patient's access, reducing the waiting times, reducing risk, and improving the quality of the care.14 The structure of the reception with risk assessment is one of the strategies for qualifying attendance in emergency units, establishing a balance between patient demands and the resources available for meeting their needs through the classification of the cases.15 Evaluation with risk classification aims not only to order the attendance to the service users, but also to avoid health problems being worsened if the attendance is delayed.13
The results indicate that the nurses in the emergency care units are challenged by a demand which exceeds that which the services are organized to recognize and intervene in. Authors stress that the organization is not restricted to material, technological and staff conditions, but that it includes equally how the work processes used in these services are organized and managed.16
The care management actions indicated are aimed at the prediction and provision of resources for producing care, through the organization and division of the nursing team's work, the object of the managerial work being the organization of the work and the nursing human resources. The managerial dimension is considered as a 'means' activity for an 'ends' activity, which is the care, such that management of the care is characterized by the articulation between the care dimension and the managerial dimension, so as to meet the patients' care needs and the institution's and nursing team's objectives.6,7
The results obtained in the present investigation are contributed to by the results of other studies,17 highlighting that the principal managerial practices of the nurses in the emergency services are the elaboration of the employees' monthly timetable and the undertaking of the daily allocation of the employees.
The issue of the dimensioning of nursing personnel has been addressed by nurses over the years, as they constantly identify and evaluate the existing resources in the face of the service users' needs, so as to provide nursing care, directly intervening in the efficiency, quality and cost of the care.18 Thus, the management, configured as an instrument of the care process, may be understood as a specific work process, based on its constituent elements as the object of work, which are human resources and the organization of the work, the end purpose being qualified human resources and organized work, so as to obtain the appropriate care and work conditions.19
The purpose of the nurses' work in the emergency care unit seeks to guarantee access to the service, based on the identification of the priorities for the attendance, according to each service user's clinical health needs, by means of the reception with risk assessment and classification. The knowledge and the work instruments configure the nurses' practices for identifying the service user's risk/vulnerability, considering the biological dimensions of falling ill and promoting the guidance and referrals necessary for the resolution of the problem which is demanded. In these terms, the emphasis on knowledge and work instruments allowed the analysis that clinical judgment is considered an essential skill for the resolution of problems. Associated with clinical judgment there is decision-making, inherent to the nurse's daily work. It refers to care, organization and management actions. The process of decision-making in the emergency care service is incisively influenced by the organizational structure. This influence occurs because health organizations are shaped by the beliefs and values of those who constitute them, who create and express their opinions and establish norms that delineate their structures and manuals of techniques and procedures.20
Listening and reception also stood out, with the intention of interacting with the service users in the classification of risk, in listening to their complaints, the use of equipment for carrying out procedures and the relevancy of the clinical knowledge in the nurses' work in emergency care. The nurses, being responsible for the gateway, direct the users' movement through the Emergency Care services, contributing to the improvement of the clinical prognosis of the users attended and reorganizing the work team's work processes. In the technological organization of the work in the Emergency Care Units, the nurses seek to enrich their conduct, widening the care beyond the initial clinical complaint in an attempt to break with the logic of the biomedical model of care, although still in an incipient form within the logic of a service which aims for nursing interventions with an instrumental character.
Conclusion. The activities of the nurses in the Emergency Care Units use technical knowledge in the resolution of routine problems, ensuring the infrastructure and maintenance of the care. Thus, the nurses' work in the emergency care setting shapes the health team's other work processes, as well as organizing the demands seeking the service through the use of specific technological knowledge. The need is indicated for widening of the discussions about the challenges to nurses' work in emergency care units, where the demand must be responded to with speed and, at the same time, must be preceded by a decision-making process with qualified listening and a development of the clinical judgment of the complaints.
REFERENCES
1. Brasil. Ministério da Saúde. Institui a Política Nacional de Atenção às Urgências, a ser implantada em todas as unidades federadas, respeitadas as competências das três esferas de gestão. Portaria n° 1863 (Sept. 29, 2003). [ Links ]
2. Furtado BMASM. O trabalho do enfermeiro em emergência: representação social, comprometimento, satisfação e condições de trabalho - O caso do Hospital da Restauração [Dissertation]. Recife: Fundação Oswaldo Cruz; 2009. [ Links ]
3. Marques GQ, Lima MADS. Demandas de usuários a um serviço de pronto atendimento e seu acolhimento ao sistema de saúde. Rev Latino-am Enfermagem. 2007; 15(1)13-9. [ Links ]
4. Mendes Gonçalves RB. Práticas de saúde: processo de trabalho e necessidades. São Paulo: Centro de Formação dos Trabalhadores em Saúde da Secretaria Municipal de Saúde; 1992. [ Links ]
5. Almeida MCP. O trabalho de enfermagem. São Paulo: Cortez; 1997. [ Links ]
6. Hausmann M, Peduzzi M. Articulação entre as dimensões gerencial e assistencial do Processo de Trabalho do Enfermeiro. Texto Contexto Enferm. 2009; 18(2):258-65. [ Links ]
7. Rossi FR, Silva MADS. Fundamentos para processos gerenciais na prática do cuidado. Rev Esc Enferm USP. 2005; 39(4):.460-8. [ Links ]
8. Silva AM. Processo de trabalho e atividades educativas de trabalhadores de enfermagem em hospitais públicos [Dissertation]. São Paulo: Escola de Enfermagem da USP. Universidade de São Paulo; 2010. [ Links ]
9. Creswell JW. Projeto de pesquisa: métodos qualitativos, quantitativo e misto. 3rd ed. Trad: Magda Lopes. Porto Alegre: Artmed; 2010. [ Links ]
10. Vieira S. Como elaborar questionários. São Paulo: Atlas; 2009. [ Links ]
11. Minayo MCS. O desafio do conhecimento: pesquisa qualitativa em saúde. 12nd. ed. São Paulo: Hucitec; 2010. [ Links ]
12. Brasil. Ministério da Saúde. Conselho Nacional de Saúde. Resolução 196. Diretrizes e normas regulamentadoras de pesquisa envolvendo seres humanos. (Oct. 10, 1996). [ Links ]
13. Shiroma LMB, Pires DEP. Classificação de risco em emergência - um desafio para as/os enfermeiras/os. Rev Enferm Foco. 2011; 2(1):14-7. [ Links ]
14. Pires PS. Tradução para o português e validação de instrumento para triagem de pacientes em serviço de emergência: 'Canadian Triage and Acuity Scale' (CTAS) [Mestrado em Enfermagem]. São Paulo: Escola de Enfermagem da USP. Universidade de São Paulo; 2003. [ Links ]
15. Garlet ER, Lima MADS, Santos JLG, Marques GQ. Organização do trabalho de uma equipe de saúde no atendimento ao usuário em situações de urgência e emergência. Texto Contexto Enferm. 2009; 18(2):266-72. [ Links ]
16. Sá MC, Carreteiro TC, Fernandes MIA. Limites do cuidado: representações e processos inconscientes sobre a população na porta de entrada de um hospital de emergência. Cad Saude Publica. 2008; 24(6):1334-43. [ Links ]
17. Santos JLG, Lima MADS. Gerenciamento do cuidado: ações dos enfermeiros em um serviço hospitalar de emergência. Rev Gaucha Enferm. 2011; 32(4):695-702. [ Links ]
18. Gaidzinski RR, Fugulin FMT. Castilho V. Dimensionamento de Pessoal de Enfermagem em Instituições de Saúde. In: Kurcgant P. (Org.) Gerenciamento em enfermagem. São Paulo: Guanabara Koogan; 2005. [ Links ]
19. Peres AM, Ciampone MHT. Gerência e competências gerais do enfermeiro. Texto Contexto Enferm. 2006; 15(3): 492-9. [ Links ]
20. Brusamolin L, Montezeli JH, Peres AM. Use of the managerial abilities by nurses of a ready attendance hospital. Rev Enferm UFPE. 2010; 4(2):818-24. [ Links ]
