Report of cases
Lower Gastrointestinal Bleeding Due to Rectal Dieulafoy’s Lesion: A Case Report
1 Second-Year Resident in Internal Medicine, Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado. Mexicali, Baja California, México.
2 General Surgeon with Advanced Specialization in Gastrointestinal Endoscopy, affiliated with the Gastrointestinal Endoscopy Service, Hospital General 5 de Diciembre, Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado. Mexicali, Baja California, México.
3 Internist with Specialty in Gastroenterology and Gastrointestinal Endoscopy, affiliated with the Gastroenterology Service, Hospital General 5 de Diciembre, Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado. Mexicali, Baja California, México.
4 Second-Year Resident in General Surgery, Hospital General 5 de Diciembre, Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado. Mexicali, Baja California, México.
Abstract
Dieulafoy’s lesion is a 1-3 mm vascular lesion in the submucosa and represents 1-2% of total GI bleeding; 80% are located in the stomach and 15% in the duodenum, while its finding in the rest of the GI tract is <5%. This work presents the case of a 79-year-old male patient who went into hypovolemic shock due to GI bleeding secondary to a rectal Dieulafoy’s lesion with endoscopic and subsequent surgical management.
Keywords: Dieulafoy’s lesion; hemoclip; lower gastrointestinal bleeding
Resumen
La lesión de Dieulafoy es una lesión vascular de 1-3 mm en la submucosa y representa del 1%-2% del total de hemorragias digestivas; 80% se localiza en el estómago y 15% en el duodeno, mientras que su hallazgo en el resto del tubo digestivo representa < 5%. En el siguiente trabajo se presenta el caso de un paciente masculino de 79 años que presentó choque hipovolémico por sangrado de tubo digestivo secundario a lesión de Dieulafoy rectal con manejo endoscópico inicial y posteriormente quirúrgico.
Palabras clave: Lesión de Dieulafoy; hemoclip; sangrado de tubo digestivo bajo
Introduction
First identified in 1989 by Paul Dieulafoy within a cohort of patients experiencing gastrointestinal bleeding in the absence of ulcerations, lower gastrointestinal bleeding caused by rectal Dieulafoy’s lesion is characterized as a winding or aberrant artery of small diameter located in the submucosa1. This condition is an infrequent cause of gastrointestinal bleeding, predominantly occurring in the lesser curvature owing to the dense vascular supply and significant diameter of the arteries in that region2. Its occurrence in the lower segments of the gastrointestinal tract is rare. Diagnosis necessitates the fulfillment of the following criteria:
Active arterial micropulsatile flow or jetting from a mucosal defect smaller than three millimeter or through intact mucosa;
The observation of a blood vessel, with or without recent bleeding signs, protruding through a minor mucosal defect or intact mucosa;
The presence of a freshly adherent clot over a minimal mucosal defect or on mucosa that appears normal3.
This condition is associated with significant morbidity and mortality due to blood loss, ranging from 8% to 10%4, making timely diagnosis and intervention crucial. Given its rarity, the risk factors and therapeutic approaches for this disease are not well-defined. Nevertheless, several descriptive studies5,6 have outlined potential risk factors (Table 1). This paper aims to report a patient case featuring an uncommon presentation of Dieulafoy’s lesion, notably due to its location in the lower gastrointestinal tract.
Table 1 Risk Factors Associated with Dieulafoy’s Lesion
| Male |
| Prior NSAID use |
| Chronic kidney disease |
| Major burns |
| Median age at presentation: 52 years |
| Type 2 diabetes |
| Systemic arterial hypertension |
| Chronic alcohol consumption |
NSAID: Non-Steroidal Anti-Inflammatory Drug. Author’s own research.
Case presentation
The subject of this case is a 79-year-old male, a diabetic and hypertensive individual with a history of renal cancer treated via nephrectomy, who presented with a week-long episode of diarrhea followed by bright red transrectal bleeding 48 hours before admission. Upon arrival at the emergency department, laboratory findings revealed severe normocytic normochromic anemia with a hemoglobin level of 6.1 g/dL, prompting the transfusion of four units of red blood cells and his subsequent admission to internal medicine for a priority colonoscopy. This decision was informed by signs of hypovolemic shock secondary to 2.5 liters of bright red stool, necessitating an urgent bowel preparation with polyethylene glycol administered over 3 hours at a total volume of 3 liters, achieving a bowel preparation described as Boston 7. The colonoscopy withdrawal time was recorded at 17 minutes.
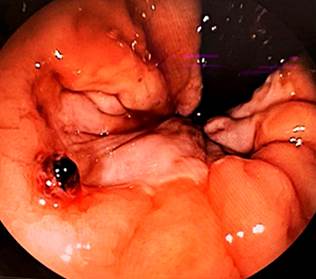
Endoscopic examination revealed blood remnants primarily in the left colon and non-significant findings of descending diverticular disease, not accounting for the substantial decrease in hemoglobin. Rectal retroflexion 1 cm from the dentate line exposed a pulsatile vessel of 2 mm diameter in otherwise normal mucosa, with minimal adjacent fibrin and an adherent clot at its tip (Figure 1).
An endoscopic intervention employing a hemoclip was selected; however, the lesion’s location prevented achieving an adequate angle for perpendicular mucosal placement, leading to the clip being applied with pressure at its base. The lesion’s diameter, suboptimal hemoclip positioning, and proximity to the anal canal necessitated a consultation with the coloproctology service for assessing definitive treatment. A spontaneous active bleeding event occurred 72 hours later, warranting surgical intervention. The procedure entailed a rectoscopy followed by the cross transfixation suture ligation of the vessel and two Lembert stitches over the previous area, aimed at minimizing friction against the aberrant vessel to lower future bleeding risks.
Conclusion
Surgical intervention for Dieulafoy’s lesion is typically reserved for scenarios where endoscopic methods, such as adrenaline injections, hemoclips, argon plasma coagulation7-9, embolization treatment failures, or instances of massive hemorrhage with hypovolemic shock, prove ineffective. Options include wide wedge resection, complete segmental resection, or the suture ligature of the lesion with transfixation of stitches10,11. In this particular case, the lesion’s suboptimal position and anatomical location limited the effectiveness of endoscopic treatment. While some literature suggests angiography as an alternative when endoscopic approaches fail or are not viable12, surgical management was deemed definitive in this instance, leading to a successful outcome without subsequent rebleeding. Despite its rarity, this lesion’s presence in such a unique location underscores the importance of considering it among the differential diagnoses for patients presenting with obscure gastrointestinal bleeding.
Referencias
1. Nguyen DC, Jackson CS. The Dieulafoy’s Lesion. J Clin Gastroenterol. 2015;49(7):541-9. https://doi.org/10.1097/MCG.0000000000000321
[ Links ]
2. Enns R. Dieulafoy’s Lesions of the Rectum: A Rare Cause of Lower Gastrointestinal Bleeding. Can J Gastroenterol. 2001;15(8):541-5. https://doi.org/10.1155/2001/851354
[ Links ]
3. Baxter M, Aly E. Dieulafoy’s lesion: current trends in diagnosis and management. Ann R Coll Surg Engl. 2010;92(7):548-54. https://doi.org/10.1308/003588410X12699663905311
[ Links ]
4. Gallo Arriaga B, Nieto Saucedo J, Gallo Chico B, Ibarra Rodríguez J, Santibáñez Bedolla K, Hidalgo Valadez C. Lesión de Dieulafoy rectal: una causa rara, pero potencialmente mortal de hemorragia del tubo digestivo bajo. Acta Médica Grupo Ángeles. 2020;18(3):302-5. https://doi.org/10.35366/95409
[ Links ]
5. Nadhem, O. N., Salh, O. A., & Bazzaz, O. H. (2017). Lower gastrointestinal bleeding due to rectal Dieulafoy’s lesion. SAGE Open Med Case Rep. 2017:5:2050313X17744982. https://doi.org/10.1177/2050313X17744982
[ Links ]
6. Massinha P, Cunha I, Tomé L. Dieulafoy Lesion: Predictive Factors of Early Relapse and Long-Term Follow-Up. GE Port J Gastroenterol. 2020;27(4):237-243. https://doi.org/10.1159/000504720
[ Links ]
7. Franko E, Chardavoyne R, Wise L. Massive rectal bleeding from a Dieulafoy’s type ulcer of the rectum: a review of this unusual disease. Am J Gastroenterol. 1991;86(10):1545-7.
[ Links ]
8. Kasapidis P, Georgopoulos P, Delis V, Balatsos V, Konstantinidis A, Skandalis N. Endoscopic management and long-term follow-up of Dieulafoy’s lesions in the upper GI tract. Gastrointest Endosc. 2002;55(4):527-31. https://doi.org/10.1067/mge.2002.122652
[ Links ]
9. Dogan U, Gomceli I, Koc U, Habibi M, Bulbuller N. Rectal Dieulafoy Lesions: A Rare Etiology of Chronic Lower Gastrointestinal Bleeding. Case Rep Med. 2014;2014:180230. https://doi.org/10.1155/2014/180230
[ Links ]
10. Wang M, Bu X, Zhang J, Zhu S, Zheng Y, Tantai X, et al. Dieulafoy’s lesion of the rectum: a case report and review of the literature. Endoscopy International Open [Internet]. 2017;5(9):E939-42. https://doi.org/10.1055/s-0043-114661
[ Links ]
11. Berkeşoğlu M, Olmez A, Aydin M, Türkmenoğlu M, Çolak T. Dieulafoy›s Lesion in the Anal Canal: A Rare Cause of Massive Gastointestinal Hemorrhage. Turkish Journal of Colorectal Disease. 2016;26:53-5.
[ Links ]
12. Inayat F, Hussain A, Yahya S, Weissman S, Sarfraz N, Faisal MS, et al. Rectal Dieulafoy’s lesion: a comprehensive review of patient characteristics, presentation patterns, diagnosis, management, and clinical outcomes. Transl Gastroenterol Hepatol. 2022;7:10. https://doi.org/10.21037/tgh.2020.02.17
[ Links ]












 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink