











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink
Introduction
Newborns with low birth weight and those born prematurely are at risk of various life-threatening conditions, including neurological deficits, heart disease, and infection 1. Preterm infants are at high risk of neurological disorders as they have suboptimal neurodevelopment compared to full-term infants. This is compounded by the need to place them in neonatal intensive care, which is highly stressful for the infant due to the premature separation from their mother and the inability to breastfeed while in an incubator. Moreover, the concurrent risk of other health conditions elevates the risk of neurological disorders 2.
The neurological risks faced by premature infants can be classified as high, medium, or low. Those with higher neurological risks suffer from higher mortality rates and are more prone to cognitive, linguistic, sensorineural, and motor impairments. Although the survival rates of preterm infants have increased due to advances in neonatology, this has led to an increased incidence of disability in those that may not previously have survived 1,3.
Many of the conditions associated with neurological risk involve language deficits and deficient motor development. The latter can cause atypical movements and prevent the acquisition of basic motor functions and functionality. Cognitive deficits and learning disabilities usually become apparent during the first five years, Cerebral Palsy (CP) is the condition most strongly associated with premature birth. The degree of dysfunction arising from CP can vary. The condition is particularly likely among infants weighing less than 3 lbs. 5 oz and born earlier than 28 weeks into the pregnancy 4,5.
Early diagnosis of such conditions is vital for timely and proper intervention. Assessments and screenings for neurodevelopmental disorders are key aspects of this process. Hence, standardized instruments for the assessment of infant motor performance are paramount; and the Test of Infant Motor Performance (TIMP) is internationally recognized. The TIMP has been used to evaluate motor performance in infants between week 34 of gestation and four months of age 6-9. Changes in scores are measured every two weeks and scores are compared to the developmental norms for the infant's current age. High levels of motor impairment found on the TIMP can be indicative of several possible conditions, including CP 10.
In the field of physiotherapy, there has been increased interest in the translation and cross-cultural adaptation of medical assessment instruments in recent years. The Mapi Research Institute states that the linguistic validation of an instrument for a target culture involves its conceptual and linguistic adaptation to the context in which it will be used. The authors of the current study followed the assessment translation and validation guidelines of Beaton et al., Escobar Bravo, Balluerka et al., Muñiz et al., Valdelamar-Jiménez et al., and Garcimartin et al. 11-16.
Translation and cross-cultural adaptation are considered in this study from communicative and functional perspectives in which translators become linguistic and cultural mediators through their production of an instrument equivalent to the original. This requires collaboration between translators and field experts and rigorous methodology that is focused on obtaining a linguistically, culturally, and disciplinarily reliable final version 17.
When the original instrument comprises distinct discursive, terminological, and conceptual conditions, the cross-cultural adaptation must comply with such conditions. In this regard, the Communicative Theory of Terminology was utilized in this research as a theoretical basis from which to comprehensively address concepts and terms 18. This theory allows for the study of specialized discourse concerning its conditions of production and reception.
This paper describes the translation and cross-cultural adaptation of the TIMP from us English to Colombian Spanish to obtain an appropriate Colombian scale for the assessment of motor performance and identification of neurological risk in infants from birth to four months.
Materials and methods
Cross-cultural adaptation has been widely used in healthcare due to the great number of instruments that medical practitioners use to assess and evaluate their patients, which are usually in English, originally. This provides opportunities for researchers to conduct cross-cultural studies that benefit health professionals and their patients. Cross-cultural adaptation is an essential aspect of the translation process but the task is neither simple nor literal and requires the amalgamation of different knowledge and skills.
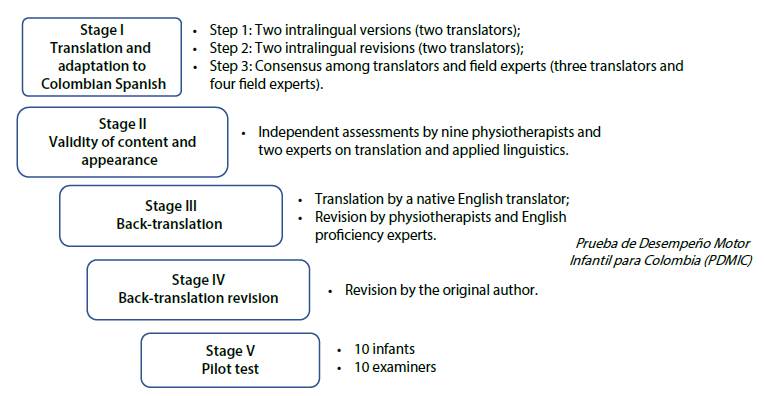
Figure 1 Stages in the Translation and Cross-Cultural Adaptation of the Test of Infant Motor Performance (TIMP)
We were granted permission to translate and adapt the TIMP to Colombian Spanish by both its original authors, Campbell et al., and by Echevarría, who generated a Spanish version for Spain 6,19.
The process consisted of five stages. These were translation and adaptation of the TIMP to Colombian Spanish; validation of the Spanish content and appearance; back-translation revision; review by the original author; and a pilot test.
This study was approved by the Bioethics Committee of the Universidad Autónoma de Manizales (act 088, 2019) and by the Research Ethics Subcommittee of the Faculty of Nursing and Rehabilitation of the Universidad de La Sabana (Code Enf-23-2017, 2017).
Instrument
The TIMP was developed by a team of researchers from the University of Chicago to assess infants from 34 weeks post-conception (born prematurely) to four months from birth. Although the original instrument states that it can be used for infants from 32 weeks post-conception, it provides a more accurate assessment from 34 weeks post-conception 6. The test consists of 42 items; 13 of which assess spontaneous movements through observation, and 29 items of which are elicited by the examiner to assess developmental behaviors such as rolling over and pulling up to sit. The test follows a standardized protocol for assessment procedures and recording responses. Observational items are scored as one or zero based on the presence or absence, respectively, of the expected motor response. Elicited items are scored between zero and six, with higher scores for better motor responses. Gross scores are the sum of all values obtained. Z-scores are used to indicate the standard deviation from the mean. These are calculated based on preestablished normative values, allowing an infant's motor development to be described as typical (z-scores >-0.5) or atypical (z-scores <-0.5) 20.
The TIMP has been tested by its original authors and by Spittle et al., both of whom found excellent correlation indices for reliability and validity, with scores of 0.98-0.99 for inter-rater reliability class correlation coefficient (CCI), with scores of 0.95 intra-rater reliability class correlation coefficient for cci, 0.89 for test-retest reliability cci, and r = 0.85 for construct validity 6,21. The Alberta Infant Motor Scale (AIMS) is a well-established and proven measure of infant motor skills that can be used at any time during the child's first year. Therefore, the TIMP was compared to the AIMS in tests of three-month-old babies. The TIMP showed high concurrent validity (r = 0.64) in this comparison 22. Scores on the TIMP have also demonstrated strong correlations with the findings of fMRI scans of the basal ganglia and white matter of preterm infants at 40 weeks chronological age, and 12 weeks corrected age 23.
Campbell and Hedeker found AIMS to have high sensitivity (92%) and specificity (76%) and Campbell et al. reported sensitivity of 92% and specificity of 76% (24,7). They further found that AIMS tests of three-month-old (corrected age) infants had a negative predictive value of 98% for a diagnosis of motor delayed motor development at 12 months of age.
The methodological procedures used in this study for translation and cross-cultural adaptation were developed in accordance with international standards that have been established to ensure equivalence between original measures and linguistically revised adaptations. The procedure comprised five stages. These are described below.
Stage I: Translation and Cross-Cultural Adaptation
The first stage comprised an intralingual translation of the TIMP from Castilian Spanish to Colombian Spanish. For this purpose, two versions were created by two independent translators, both of whose mother tongue is Colombian Spanish. The purpose of this was to produce two preliminary versions that conceptually and linguistically replicated the original instrument. Although Spain and Colombia share the same official language, the social and cultural contexts differ, thus adjustments regarding cultural, idiomatic and conceptual were made. Neither translator had academic or practical experience in physical therapy. After this, two different translators independently reviewed both initial translations. To minimize errors, three translators and four experts in physiotherapy and with experience treating newborns met to discuss the two translations and develop a common version. This involved triangulation of the original English version, the two intralingual versions, and the target context in which the instrument would be utilized. The conceptual (disciplinary field), semantic (meaning), and pragmatic (linguistic, experiential, and contextual) dimensions of each item were analyzed and classified. The conceptual dimension was assessed by physiotherapists because of their expert knowledge. The Colombian Spanish grammar and conventions appropriate to this kind of writing and the adequacy and precision of the terminology used were considered as aspects of the semantic and pragmatic dimensions. In terms of experiential equivalence, those expressions relevant to the daily lives and cultural experiences of test users were adapted to express the same meaning in a more relevant manner within the target context. A written report was produced to document all stages of this process. The final amalgamation of the two translations, agreed upon during this meeting and discussion, was the preliminary version of the instrument in Colombian Spanish: Prueba de Desempeño Motor Infantil para-Colombia (PDMIC).
Stage II: Validation of Content and Appearance
A team of nine expert judges with a requisite post-graduate education, teaching and research experience, and neurodevelopmental training; three translators; and two applied linguists, with in-depth knowledge of English and Spanish, judged this preliminary version. Preestablished criteria were used to ensure all elements were fully assessed, and each criterion was judged through the selection of a score on a Likert scale.
Each expert conducted their quantitative and qualitative assessments independently. The criteria upon which each item was assessed were relevance, adequacy, clarity, observability, starting positions, and procedures. The rating scale for each ranged from one to four (1: totally disagree, 2: disagree, 3: agree and 4: totally agree) (see Table 1).
Table 1 Criteria Used by Expert Judges to Evaluate our Colombian Spanish Translation of the Test of Infant Motor Performance (TIMP)
| Criterion to be evaluated | Suggested question |
|---|---|
| Relevance: Whether the item and its qualification are important for the evaluation of motor development in Colombian infants aged 0-4 months. | Do you think that this item and its qualification are important for the evaluation of motor development in Colombian infants aged 0-4 months? |
| Adequacy: The capacity of each item and its qualification to properly evaluate motor development in Colombian infants aged 0-4 months. | Do you believe that the item and its qualification are sufficient to evaluate this aspect of motor development in Colombian infants aged 0-4 months? |
| Clarity: Whether the item and its qualification are accurate and understandable for use in the evaluation of motor development in Colombian infants aged 0-4 months. | Do you believe this item and its measurement would be clear and understandable to an evaluator? |
| Observability: Whether the elements assessed by the item could be observed by an external evaluator in Colombian infants aged 0-4 months (the external evaluator being a healthcare professional such as a physiotherapist or occupational therapist). | Do you think that the elements to be evaluated by this item and its qualification could be observed by an external evaluator in Colombian infants aged 0-4 months? |
The means (M), standard deviations (SD), and coefficients of variation (cv) for the criteria listed above were used to determine where alterations were required, according to the following rules:
If an item achieved high average scores (M ≥3.0) and low variability (SD <1.0) on a given criterion, it was deemed to require few, or no, adjustments.
Different scores from the prior ones demanded item adjustment.
If an item had a cv ≥0.4 in relation to its standard deviation and mean for a given criterion, it was judged to require adjustments.
The qualitative assessments consisted of additional notes and comments from the judges. The revisions made in response to the judges' evaluations resulted in the penultimate version of the Prueba de Desempeño Motor Infantil para-Colombia (PDMIC).
Stages III & IV: Back-Translation and Revision by the Original Author
Back-translation of a translated instrument consists of translating the revised measure back to its original language to ensure no meaning or important elements have been lost. This was initially conducted by one English translator native to England, with no background in physical therapy. The resulting version was reviewed by two bilingual physical therapy experts, who evaluated the appropriateness of its terminology and its semantic coherence. The final form of the back-translated instrument was achieved once the latter were satisfied with the resulting English version of the TIMP/PDMIC. This was then sent to the original author, who assessed the back-translation to determine its concordance with the original. Dr. Campbell approved the version as a conceptually and linguistically sound, purpose-appropriate Colombian Spanish adaptation of the original instrument.
Stage V: Pilot Test
A pilot test was conducted with a group of ten physiotherapists with experience and training in neurodevelopment, neurorehabilitation, and child development. These were representative of the target population who will use the test. The purpose of the pilot was to empirically verify the instrument's equivalence, clarity, feasibility, and acceptability.
Probing techniques were used to test all items according to the following five criteria: (a) understanding of the instructions, (b) understanding of the items, (c) understanding of the scoring options, (d) time taken to administer the test and administration difficulties. For the first four criteria, the participant physiotherapists rated the adequacy of the test on a scale from 1 to 4: 1 for very inadequate, 2 for inadequate, 3 for adequate, and 4 for very adequate. Difficulty levels were also rated from 1 to 4: 1 for very difficult, 2 for fairly difficult, 3 for mildly difficult, and 4 for not difficult. A meeting among researchers and linguists was held for consensus.
Results
During the first stage of translation and adaptation, the authors conducted a comprehensive analysis and classification of the items on the TIMP from both a linguistic and a disciplinary perspective; considering the semantic, idiomatic, experiential, and conceptual components of the test. Most changes were relatively minor conceptual and contextual aspects due to cultural differences in the use of terminology and professional practice in the field of neurodevelopment in Colombia. The items were then deemed equivalent to the original.
The majority of adjustments to items were for semantic equivalence, followed by conceptual and experiential equivalence. Adjustments to various aspects were sometimes necessary to achieve equivalence in the same item. This was the case for the elicited items 15, 16, 22, 23/34, 38/39, which required adjustments for three types of equivalence. After this first stage, the authors tested for the Colombian context to ensure there were no uncertainties or ambivalence in the reading, monitoring, and execution of procedures when the test was administered (Table 2).
Table 2 Example Items from the Test of Infant Motor Performance (TIMP) Translated and Adapted to Colombian Spanish, with English-Spanish Correspondences
| Item | Item in English | Item translated and adapted to Colombian Spanish | Equivalence type |
|---|---|---|---|
| Observed item 5 | Touches objects or surfaces to the left | Toca objetos o superficies con la mano izquierda | Semantic and conceptual correspondence |
| Elicited item 15 | Head control -supported sitting | control cefálico - sedente con apoyo | Semantic, conceptual, and experiential correspondence |
| Elicited item 19/20 | Inhibition of neonatal neck righting | Integración de la reacción de enderezamiento cervical | Semantic and conceptual correspondence |
| Elicited item 28/29 | Rolling: elicited using the legs | Rolado: movimiento provocado desde los miembros inferiores | Semantic and conceptual correspondence |
| Elicited item 36 | Head lifting while prone | Control cefálico en decúbito prono | Conceptual correspondence |
| Elicited item 38/39 | Head turning while prone in response to sound | Seguimiento auditivo en decúbito prono | Semantic, conceptual, and experiential correspondence |
The second stage involved quantitative and qualitative evaluation. The former was measured using judges' scores of each item on several criteria. Scoring was on a Likert scale, ranging from 1 to 4. The scores were assessed for central tendencies and dispersion, resulting in adaptations and changes to the items. These results were satisfactory, with the criteria of relevance, sufficiency, and observability obtaining the expected results in their median, SD, and cv. Clarity was the only criterion with results outside of the expected range. Specifically SD >1.0 and cv >4.0. This was primarily for elicited items (Table 3). These items were reviewed by the researchers and their adjustments requirements analyzed.
Table 3 Quantitative Evaluation of the Clarity Criterion of the FDMIC by Expert Judges
| Item | Criterion: clarity | |
|---|---|---|
| Standard deviation | Coefficient of variation | |
| Observed item 5 | 1.0 | Adequate |
| Observed item 12 | 1.0 | Adequate |
| Elicited items 19/20 | 1.0 | Adequate |
| Elicited item 25 | 1.1 | Adequate |
| Elicited item 26 | 1.3 | 0.4 |
| Elicited item 34 | 1.0 | Adequate |
| Elicited item 37 | 1.0 | Adequate |
| Elicited item 40 | 1.0 | Adequate |
A qualitative evaluation was performed for each item and comments and suggestions were made. The researchers then met to identify, and agree upon, the adjustments required. The suggestions were mainly related to the use of prepositions, punctuation marks, the decimal metric system, and the correct use of terminology relating to morphology and anatomy and the clinical field, including language referring to evaluation and neurodevelopmental interventions in the Colombian context. Each item was assessed through consideration of the statement, the starting position, the procedure, and the rating scale. Finally, after following the judges' recommendations, a consensus was reached on the wording of each item. Thus, the penultimate version of the PDMIC was obtained. Examples of items modified based on the qualitative evaluations of expert judges are depicted in Table 4.
Table 4 Example Items from the Test of Infant Motor Performance (TIMP) after Adaptation and Adjustment to Colombian Spanish and Qualitative Evaluation
| Item | Item in english | Item translated and adapted to Colombian Spanish after judge consensus | Item translated and adapted to Colombian Spanish: pre-final version |
|---|---|---|---|
| Observed item 9 | Reciprocal Kicking: demonstrates reciprocal kicking with both legs off the support surface | Pataleo recíproco - realiza pataleo recíproco con ambas extremidades inferiores separadas de la superficie de apoyo | Pataleo recíproco - realiza pataleo recíproco con ambos miembros inferiores separadas de la superficie de apoyo |
| Observed item 12 | Oscillation of arm or leg during movement: more or less regularly fluctuating movements which are observed most in the extended arms. A movement cycle lasts .5-1an average of 0.51 sec (slower than a tremor). | Oscilación de la extremidad superior o la inferior durante el movimiento - realiza movimientos fluctuantes más o menos regulares que son observados principalmente con las extremidades superiores extendidas. Un ciclo de movimiento dura entre 0.5 y 1 segundo (más lento que el temblor) | Oscilación del miembro superior o inferior durante el movimiento - realiza movimientos fluctuantes más o menos regulares que son observados principalmente con los miembros superiores extendidos. Un ciclo de movimiento dura entre 0,5 y 1 segundo (más lento que el temblor) |
| Elicited item 15 | Head control - supported sitting | Control cefálico: sentado con apoyo | Control cefálico: sedente con apoyo |
| Elicited item 18 | Head control - lowered from sitting | Control cefálico: sentado a supino | Control cefálico: desde sedente a decúbito supino |
| Elicited item 33 | Lateral straightening of the head and body with arm support | Enderezamiento lateral de la cabeza y el cuerpo con ayuda de la extremidad superior | Enderezamiento lateral de la cabeza y el cuerpo con soporte del miembro superior |
Our back-translation of the PDMIC in the third stage demonstrated that following international standards for this process had produced a successful cross-cultural adaptation of the assessment instrument.
The pilot test consisted of training professionals in the use of the assessment and their subsequent evaluation of the instrument. All of the criteria used in earlier stages were rated on scales of 1-4. Most average ratings for the various criteria were higher than 3.2/4.0, with the majority ≥3.8. Overall, the evaluators found the test easy to understand with no ambiguity in the instructions, items, or scoring system. The language was seen as appropriate to the target population, and administration times were sufficient for assessing neuromotor development in children under five months of age.
Discussion
This study describes the translation and cross-cultural adaptation of the TIMP for the Colombian context, which was undertaken because of the lack of existing adapted instruments for assessing the development of infant motor skills. A standardized instrument is required to accurately assess indicators of neurological compromise displayed in motor performance for early diagnosis and timely referral to health and rehabilitation specialists.
The TIMP, the Bayley Scales of Infant Development-Psychomotor Development Index ed. I (BSIDPDI-I) 6,25; the Bayley Scales of Infant Development-Psychomotor Development Index ed. II (BSID-PDI-II) 26; the Bayley Scales of Infant and Toddler Development-Total Motor Quotient ed. III (BSITD-III) 27; the Griffiths Locomotor Subscale, the AIMS, and the Peabody Developmental Motor Scales eds. I and II are among the tests used to assess this population but, unfortunately, these were originally developed in English 28-30. Therefore, studies such as this are vital for the dissemination of these tools to all of the countries that require them.
Early diagnosis and timely intervention are paramount, particularly for preterm infants, who have a high prevalence of developmental and motor development disorders, including CP 31. For this reason, guidelines have been published to assist relevant professionals in early detection 9. This includes the evaluation of motor performance in infants under five months. This cutoff is based on the established high risk period for the development of CP between three and four months 6,7,9. Within such assessments are criteria able to predict a 95% probability of developing CP in the following years. These guidelines emphasize the necessity for motor assessment scales applicable during this period such as the TIMP, the General Movements Assessment, and the Hammersmith Infant Neurological Examination 9,32,33.
The usefulness and sensitivity of the TIMP in the evaluation of motor performance in both full-term and premature infants has been extensively studied 23,34. It has demonstrated excellent discriminative and predictive capacities for the identification of infants at risk of delayed motor development 9. Evidence suggests that the TIMP is particularly sensitive in the prediction of CP, the risk of which becomes apparent when TIMP scores are lower on items that require action against gravity and the balanced use of extension and flexion muscle activity patterns 28-35.
The TIMP can also be used in infants with type I spinal muscular atrophy and Down's syndrome as these infants show greater difficulties with early postural control and activities that require speed and balance 20,36,37. Although the TIMP has sufficient reliability across the age range for which it is designed, it is also sensitive to the effects of neurodevelopmental intervention programs in infants from the 34th postconceptional week in a special care environment. This can aid in interventional development since the test can detect differences in motor performance between infants receiving the intervention and untreated control children. Thus, its construct validity for the detection of changes in motor performance has been demonstrated, as has its sensitivity to the effects of early intervention 37.
The above demonstrates the need for a translation and cross-cultural adaptation of the TIMP for use in the Colombian context for evaluation and clinical characterization of the target population. It can also contribute to the development of epidemiological profiles of infant motor functioning in their first months of life, affecting the health of a broad demographic of children with potential national benefits in terms of disability.
This proposal also demonstrates that the process of adapting an instrument is not just literal translation. In this case, an intralingual translation was performed because of the availability of a previous version.
The process described herein demonstrates the value of interdisciplinarity collaboration to a successful translation and adaptation of an assessment tool. The involvement of disciplinary experts utilizes their professional interest in ensuring the accuracy of the assessment. The quantitative validity of the PDMIC was excellent, with only eight of the 42 items obtaining values outside of the expected range for their SD (<3.0) and cv (≥1.0). In all instances, these were for the clarity criterion.
The TIMP has previously been translated and adapted into Portuguese. The Brazilian version was obtained from a validity and reliability study with 20 health professionals and 655 infants. The results evidenced adequate content validity due to the high levels of agreement between expert evaluations of the clarity and relevance of the items and the language used. These were determined using the content validity coefficient and Gwet's coefficient of agreement, respectively, and achieved achieving higher values than expected. There were also satisfactory results for inter-evaluator reliability (>0.65), intra-evaluator reliability (>0.97), internal consistency (Cronbach's alpha >0.71), and the discriminant and predictive validity of the test to identify and predict those at risk of delayed motor development 38.
Finally, we were not restricted by limitations caused by lack of authorization from the original author or the availability of translators, expert judges, and a native translator for back-translation. This allowed us to work expediently through the stages described. It is noteworthy that an instrument such as the TIMP was not previously available in Colombian Spanish. We hope that our adaptation will assist health professionals who evaluate infant motor performance and match up to the standards of the original. The appropriate evaluation of children, timely detection of motor development disorders, early diagnosis of neuromotor pathologies, and prompt interventions can now be achieved, with potentially widespread benefits for the epidemiological profiles of health and disability in Colombia.
Conclusion
The process of translation and cross-cultural adaptation of the TIMP to Colombian Spanish for the assessment of infants aged 0-4 months was successfully achieved using validated methodological standards. The PDMIC maintains idiomatic, cultural, and semantic equivalence to the original and has received positive endorsement by the primary original author. The outcome is an instrument that can be used to assess infant motor performance and identify neurological risks. The content validity has been verified, ensuring a clear and adequate structure for ease of administration. Further research will aim at determining the metric properties of validity and reliability among the Colombian infant population.

