











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink
Starting in March 2020, the world suffered from a public health crisis because of the COVID-19 pandemic. In Colombia, the first confirmed case of COVID-19 was on March 6 after a citizen from Milan, Italy, attended the health services in Bogotá, Colombia, due to COVID-19 symptoms (Ministerio de Salud y Protección Social [MinSalud], 2020a). On March 11, there were nine confirmed cases of COVID-19 in the country (MinSalud, 2020b); the next day, the president of Colombia declared a health emergency (MinSalud, 2020c) where the events hosting more than 500 people were banned. The number of people allowed to gather at events was later reduced to 50 people, also bars and nightclubs in the whole country were closed (MinSalud, 2020d); by March 24, a mandatory national quarantine was established (Pinilla & Ramírez, 2020a). Prevention and quarantine measures were gradually lifted starting June 2020 and were specially opened by February/ March 2021 when vaccination massively arrived in Colombia. So far, by the end of January 2023, in Colombia, 6.357.200 cases of COVID-19 and 142.544 deaths were confirmed (Instituto Nacional de Salud [INS], 2023). International health authorities developed many strategies to limit the spread of this pandemic, mainly based on adopting new behaviours, such as social distancing or using a face mask (World Health Organization [WHO], 2020). These were taken as the only way to limit the pandemic’s human and economic consequences waiting for massive vaccinations to start at the beginning of 2021 (Harvard Medical School, 2021). Governments worldwide, including Colombia, recommended the adoption of these behaviours as a public health strategy for COVID-19 containment (Minsalud, 2020e).
Sadly, these behaviours’ effectiveness compared to their perceived costs was the subject of public discussion even in the face of scientific evidence (Ragonnet-Cronin et al., 2021), making its consistent adoption difficult. Hence, motivating citizens to adopt these prevention behaviours consistently is paramount. Moreover, given the political and practical difficulties in adopting policing strategies to embrace behaviour change, countries must rely on persuasive public communication instead. Finally, despite COVID-19 apparently becoming an endemic disease, we believe our insights can help communicate about possible future pandemics, such as Monkeypox and combating newer strains of COVID-19.
Because of the pressing social need following the COVID-19 pandemic, the scientific community quickly started numerous research projects to restrain its effects. Scientific literature aiming at adopting prevention behaviours has taken two distinct views. Some have been interested in these behaviours from a health promotion stance and have been mainly interested in risk perception and risk communication to motivate people to adopt prevention behaviours (Gerhold, 2020). Others frame these behaviours as ways to mitigate harm to the self and others and therefore have tried to change these behaviours based on norm communication (Everett et al., 2020). Based on a large-scale dataset from the Colombian Association of Psychology Faculties (ASCOFAPSI) and the Universidad Autónoma de Barcelona (UNAB) (Sanabria-Mazo et al., 2021), we aim to unify these views for determining how to effectively motivate consistent adoption of prevention behaviours in the face of the COVID-19 pandemic using risk and norm messages and perceived behavioural control.
From the beginning of the pandemic, numerous research teams have tried to explain the effective adoption of prevention behaviours (Dong et al., 2020; Gerhold, 2020; Hume et al., 2020; Van Bavel et al., 2020a). Since COVID-19 implies a personal risk of death or permanent injury, researchers have viewed this as a risk communication problem (Abrams & Greenhawt, 2020; Zhang et al., 2020). Research on the effect of risk perceptions on adopting prevention behaviours shows mixed results. Some suggest a positive correlation between perceived vulnerability and seriousness of COVID-19 and the intent to adopt prevention behaviours among healthcare workers and older people (Barakat & Kasemy, 2020; Irigoyen-Camacho et al., 2020). Other studies failed to find this correlation between perceived severity and intent to adopt prevention behaviours (Yildirim & Güler, 2020) or found a negative correlation, whereby the more people associate COVID-19 with death, the less likely they are to adopt prevention behaviours (Jiménez et al., 2020). A study by Trifiletti et al. (2021) even found that risk perception has a significant correlation with some behaviours, like social distancing, while having no effect on other preventive behaviours, like hand washing. Suggesting that different factors underlie the effective adoption of different behaviours. These apparently contradictory results could be explained by unknown mediator variables such as belonging to at-risk groups (Falco & Zaccagni, 2020; Irigoyen-Camacho et al., 2020; Lekamwasam & Lekamwasam, 2020) and political preferences (Barrios & Hochberg, 2020; Byrd & Bialek, 2021), among others applying differently to different target behaviours. While these variables may have observable effects on the intent to carry out prevention behaviours, effective public communication can hardly be targeted based on them. Therefore, we are interested in variables that could be directly implemented in broad communication efforts by health authorities aimed at diverse population segments.
On a different view, the proliferation of the COVID-19 pandemic has direct implications for health, particularly for fragile populations such as the elderly or chronically ill people. For example, in Colombia, people in the lower socioeconomic classes have ten times more chances of dying from COVID-19 than those in the highest socioeconomic stratum (Grupo de Investigación en Macroeconomía, 2020b). Hence, researchers have also viewed prevention behaviours adoption as social and moral issues hinging on protecting vulnerable members of society (Drury et al., 2020). Results from this perspective also suggest mixed results. People find messages highlighting individual rights and duties more motivating than messages highlighting the number of saved people or what a morally good person would do. Surprisingly, when asked which of these messages they expect to be more effective, people expected consequentialist messages to be more effective (Everett et al., 2020). These results hint that carefully designed, morally framed messaging could effectively motivate people to adopt prevention behaviours (Byrd & Bialek, 2021; Graso et al., 2021). Morally charged messages appear to be especially effective given the effect of empathy and motivation to protect family and friends as a driver to adopt prevention behaviours (Christner et al., 2020; Pfattheicher et al., 2020). Similar conclusions suggest that social norms or identifiable victim messages are more effective at behavioural change compared to purely informational messages (Hume et al., 2020). To maximise their impact, these messages can be complemented with other manipulations, such as framing effects (Gantiva et al., 2021). While these results offer fruitful avenues for effective communication, they fail to consider the eventual effects of perceived or actual behavioural control and to try to unify different variables into a coherent, theoretically driven model.
The Theory of Planned Behaviour (TPB) is a dispositional approach to predicting human behaviour in cases where self-regulation is determinant to follow dietary restrictions or medicine intake. According to the TPB, these behaviours are mainly predicted by intentions. Intentions, in turn, are bound to three determinants: attitude towards the target behaviour, subjective norms about the target behaviour and perceived behavioural control over it (Ajzen, 1991, 2006, 2011). Attitudes toward the behaviour correspond to whether a person thinks positively or negatively about the considered action. Subjective norms are the amount of social pressure a person feels about a given action and are directly linked to attitudes and actions perceived to be held by others. Finally, perceived behavioural control is the sum of perceived obstacles or facilitators and perceived self-efficacy to carry out the considered action. This framework has been successfully used to predict intent to carry out prevention behaviours in the face of the COVID-19 pandemic (Fischer & Karl, 2020). It has been proven to predict some COVID-19 preventive behaviours better than other theories of health behaviours (Sieverding et al., 2022). Moreover, the TPB has been used to explain and promote adherence to health behaviours outside the COVID-19 pandemic, such as dietary patterns, adherence to medication, exercise, and stress management (McDermott et al., 2015) as well as different “self-care activities” related to chronic illnesses like diabetes, chronic insomnia, and hypertension (Rich et al., 2015). The TPB has proven useful in promoting the intention to vaccinate and reducing vaccine hesitancy (Xiao & Wong, 2020).
Concerning COVID-19 protective behaviours, many studies showed the effectiveness of the TPB in explaining the adoption of behaviours crucial to reduce the COVID-19 spread. Namely, three components (social norms, perceived behavioural control and attitudes) have a significant relationship with the intention of hand washing (Trifiletti et al., 2021; Wollast et al., 2021), social distancing (Trifiletti et al., 2021) and limiting social interaction (Wollast et al., 2021). Also, mask use was significantly related to perceiving a situation as easy to carry out (Fikriana et al., 2021). The relation between the intention to perform the behaviours mentioned and the reported behaviour was significant in all cases. Moreover, a meta-analysis by Fischer & Karl (2020) compared 335 effect sizes from 83 articles that studied the relation between the TPB components with reported behaviour and behavioural intentions relevant to the COVID-19 pandemic. It was found that, of all three components, Perceived Behavioural Control had a stronger correlation with behavioural intentions and behaviours. In some cases, people with high self-efficacy were four times more likely to adopt preventive behaviours than those with low self-efficacy (Mao et al., 2021), highlighting TPB’s relevance to effective interventions that foster preventive behaviours in the face of COVID-19 and similar pandemics. Based on available variables in the analysed dataset, we selected all variables reflecting all three determinants proposed by TPB (Ajzen, 1991, 2006, 2011).
Methods
Database
The database was collected by ASCOFAPSI using snowball sampling from May 20th to June 20th, 2020, and data using a questionnaire designed by ASCOFAPSI and the University of Barcelona, measuring 118 variables. The database was offered to research teams from institutions associated with ASCOFAPSI in an open public call. Ours was one of the selected projects of this call.1 Methods are described in the original article (Sanabria-Mazo et al., 2021); hence further details about sampling and data collection procedures are consigned.
Participants
The complete database provided by ASCOFAPSI to us contains data from 926 participants. We excluded from the analysis 7 participants who either did not accept the online informed consent, did not claim to live in Colombia or claimed to be younger than 18 years old. The final dataset included 919 participants -708 women, three people who did not self-identify with either men or women, mean age = 32.4 ± 12.4- (Table 1).
Table 1 Sociodemographic Characteristics of Participants
| Demographics | Full sample | ||
|---|---|---|---|
| n | % | ||
| Gender | |||
| Female | 703 | 76.5 | |
| Male | 216 | 23.5 | |
| Age | |||
| 18-40 years old | 570 | 62 | |
| Over 40 years old | 349 | 38 | |
| Colombian nationality | 919 | 100 | |
| Region Urban | 850 | 92.5 | |
| Rural | 69 | 7.5 | |
| Employment | |||
| Student | 334 | 36.3 | |
| Employed | 445 | 48.4 | |
| Unemployed | 140 | 15.3 | |
| Income | |||
| Low | 255 | 27.8 | |
| Middle | 584 | 63.3 | |
| High | 80 | 8.7 |
Materials
The complete survey measured 118 variables including previously published and ad hoc scales constructed by the original research team. Excepting demographic questions, all questions are 4- or 5-point Likert scales. Further details about the construction of the questionnaire and the sources of the scales used can be found in Sanabria-Mazo et al. (2021).
Out of all 118 collected variables, we selected 85 variables theoretically compatible with our research question. These were chosen because they could theoretically fit within the TPB framework or were directly related to risk. In addition, we use Exploratory Factor Analysis (EFA) over these 85 variables as a dimensionality reduction technique to determine whether conceptually similar variables could be taken as distinct or ought to be unified. Once these EFA models were run to reduce the number of variables, based on TPB and research on risk perception on COVID-19, we ran a multiple mediation model with each prevention behaviour as a dependent variable mediated by intent and with all other variables as independent variables (Figures 1-5).
Data Management
This project is based on analysing data priorly collected by ASCOFAPSI and the Universidad Autónoma de Barcelona (Sanabria-Mazo et al., 2021) to answer a novel research question. Therefore, we defer from the original article to sufficiently describe data collection methods and scale choice rationale and decisions. Here, we only describe the data analysis strategy. ASCOFAPSI sent a raw data file to the research team for analysis. First, we excluded from the analysis all variables dealing with emotional reactions to COVID-19 and stable personality traits. While important, these variables are not easily manipulated in public communication and therefore are not of primary interest to our project.
Next, we applied the EFAs with varimax rotation as a data reduction technique to determine whether different items could be justifiably unified into a single measure or were better analysed as separate concepts (see the Variable Reduction Section and table 2 for details on each EFA and conclusions derived from them).
After data reduction, we ran one SEM model for each dependent variable. SEM model was used to test the predicted multiple mediation model described above derived from TPB and Risk perception literature, not to derive emerging patterns from data. The complete data analysis script is available on this manuscript’s OSF page.
Ethical Aspects
Since our analysis is conducted over secondary data, we were not responsible for the ethical aspects of data collection. The survey used to collect the data was approved by the Animal and Human Experimentation Ethics Committee of the Autono- mous University of Barcelona (CEEAH-5197) by the ethical committee of the Colombian Association of Psychologists (COLPSIC). This survey contained informed consent, and our analysis only con- sidered data from participants who accepted it.
Results
Variable Reduction: Exploratory Factor Analysis
We ran eight EFA over sets of variables thematically grouped in the original database. All EFAs were run with varimax rotation complemented by Cronbach’s Alpha and McDonald’s Omega. EFAs were run as a variable reduction technique to have a manageable number of variables to be used in multiple mediation models described below. Cronbach’s Alpha assumes the uni-dimensionality of the observed scale and uncorrelated errors. Since we are precisely trying to determine uni- or multidimensionality, we complemented this analysis with McDonald’s Omega, a reliability measure that does not assume uni-dimensionality or uncorrelated errors (Goodboy & Martin, 2020).
Reported Prevention Behaviours
We fitted an EFA with all reported prevention behaviours (using a face mask, washing hands, avoiding touching the face, social distancing and asking others to adopt prevention behaviours). We excluded reports of wearing gloves since international and national health authorities recommend it (WHO, 2020). This EFA suggested a 4-factor solution (Explained Variance = 100 %, RMSR = 0.8; Χ² = 11.75; p < 0.001). This, coupled with a relatively low Cronbach’s Alpha and McDonald’s Omega (Alpha = 0.614; IC (95 %) = [0.567; 0.657]; Omega = 0.61; IC (95 %) = [0.57; 0.66]) suggests that each behaviour ought to be analysed separately. In what follows, we will take each behaviour as separate dependent variables.
Intent to Implement Prevention Behaviours
As with reported prevention behaviours, we fitted an EFA with all variables dealing with intent to carry out prevention behaviours -i.e., intent to use a face mask, intent to wash hands, intent to avoid touching the face, intent to keep social distance, intent to ask others adopt prevention behaviours-. As before, we excluded the intent to wear gloves. Results resemble reported behaviours (Explained variance of a 4-factor solution = 71.7 %, RMSR = 0.079, Χ² = 105; p < 0.001; Cronbach’s Alpha = 0.694; IC (95 %) = [0.664; 0.722]; Omega = 0.78; IC (95 %) = [0.74; 0.81]). Hence, we conclude that intent variables ought also to be taken as separate rather than a single construct. We will consider the intent to carry out each prevention behaviour as a separate mediator variable.
Different Motivations to Implement Behaviours
We ran an EFA with all variables dealing with protecting the self and others from contagion and avoiding conflicts with others and the authorities. EFA suggests a bi-factorial solution wherein motivation to protect the self and others from contagion are unified in a single factor, whereas motivation to avoid conflicts with others and with the authorities are in another (Explained variance of two-factor solutions = 79.1 %, RMSR = 0.122, Χ² = 21.1; p < 0.001). These conclusions seem compatible with a relatively low Cronbach alpha for all four variables (Alpha = 0.606; IC (95 %) = [0.562; 0.649]; Omega = 0.69; IC (95 %) = [0.41; 0.73]). Hence, we averaged across protect the self and protect others to create a single variable called motivation to protect to be used as a single independent variable reflecting the motivation to protect self and others from COVID-19. The same procedure was followed with the motivation to avoid conflicts with others and with the authorities’ variables, creating the motivation to avoid conflict variable to be used as a single independent variable reflecting the motivation to prevent problems due to not implementing prevention behaviours.
Expected Effectiveness of the Prevention Behaviours Perceived by the Self2
Surprisingly, the EFA of expected effectiveness of prevention behaviours exhibited a uni-factorial solution (Explained variance of a 2-factor solution = 68.1 %, RMSR = 0.08, X² = 34.4, p < 0.001) where all variables strongly loaded into a single factor. This was confirmed by high Cronbach’s alpha and McDonald’s Omega (Alpha = 0.890; IC (95 %) = [0.877; 0.901]; Omega = 0.79; IC (95 %) = [0.75; 0.82]). Hence, we averaged across all these variables to create a single expected effectiveness of the prevention behaviour as perceived by the self variable. This variable will be used as an independent variable reflecting the extent to which participants believed all prevention behaviours actually protect them from COVID-19.
Expected Effectiveness of the Prevention Behaviour Perceived by Others
As before, EFAs suggest a unifactorial solution for all expected effectiveness as perceived by others variables. Results were confirmed by relatively high Cronbach’s Alpha and McDonald’s Omega (Explained variance of a 2-factor solution = 71.8 %, RMSR = 0.06, X² = 20.5 p < 0.001; Alpha = 0.851; IC (95 %) = [0.829; 0.871]; Omega = 0.86; IC (95 %) = [0.84; 0.87]). Hence, we averaged all these variables into one variable: the expected effectiveness of the prevention behaviour perceived by others. As before, this variable reflects the second order belief that others think all prevention behaviours actually prevent COVID-19. This variable will also be used as an independent variable.
Perceived Opinions and Barriers
EFA suggests a bi-factorial solution distinguishing opinions by others from perceived barriers about prevention behaviours. Opinions factor includes perceived opinions by others, experts, social media and family and friends. The second factor only included the perceived barriers to carrying out target behaviours variable (Explained variance of a 2-factor solution = 69 %, RMSR = 0.124, X² = 39.3 p < 0.001; Alpha = 0.772; IC (95 %) = [0.743; 0.798]; Omega = 0.76; IC (95 %) = [0.73; 0.78]). Hence, we averaged opinion by others by experts, in social media and by family and friends into a single opinions variable. This variable reflects whether participants perceive others -social media, family, friends or experts- as having positive or negative attitudes towards protection behaviours. On the contrary, the single-item barriers variable deals with whether participants perceived more general barriers preventing them from carrying out prevention behaviours, such as difficulty accessing face masks or running water. The averaged variable and the single-item perceived barriers to carrying out target behaviours will be separate independent variables.
Self-Efficacy and Capacity
As before, EFA suggests a bi-factorial solution. The first factor deals with perceived self-efficacy, the ability to surmount challenging situations. On the other hand, the second deals with capacity, the perception of being capable of actually implementing prevention behaviours, as opposed to more abstract challenging situations (Explained variance of a 2-factor solution = 50.4 %, RMSR = 0.082, X² = 90.9, p < 0.001; Alpha = 0.815; IC (95 %) = [0.795; 0.834]; Omega = 0.73; IC (95 %) = [0.7; 0.76]). Hence, we averaged across self-efficacy items to create a single self-efficacy variable. We also averaged across capacity items to create a single capacity variable. Both variables will be used as independent variables.
Trust
EFA suggests that every trust variable (i.e., trust in others, in the national and regional government, scientists and healthcare workers) load into distinct factors (Explained variance of a 2-factor solution = 55.4 %, RMSR = 0.181, X² = 83.1 p < 0.001; Alpha = 0.484; IC (95 %) = [0.427; 0.535]; Omega = 0.68; IC (95 %) = [0.63; 0.71]). Hence, every trust variable will be used as singleitem independent variables.
Risk
Following the classic economic theory, exploratory factor analysis suggests a bi-factorial solution to different aspects of risk. The first factor is the perceived probability of the self and others’ likelihood of contracting COVID-19. In contrast, the second factor is composed of the perceived seriousness of the symptoms of COVID-19 for the self and others (Explained variance of a 2-factor solution = 774.3 %, RMSR = 0.179, X² = 48.6 p < 0.001; Alpha = 0.687; IC (95 %) = [0.643; 0.726]; Omega = 0.69; IC (95 %) = [0.63; 0.73]). Therefore, we created two distinct variables reflecting perceived risk. First, the probability variable, resulting from averaging the perceived probability of COVID-19 infection for the self and others and seriousness, averages across how dangerous participants expect a COVID-19 infection to be for them and others. Both probability and seriousness variables will be used as independent variables separately.
Presented EFA allowed us to reduce the number of variables that could be related to the TPB to a more manageable, empirically justified, number to be used in the next step of analysis.3 See table 2 for a summary of original and final variables and how they relate to TPB.
Table 2 Variables Used in All Multiple Mediation Models and Their Place within TPB and Risk Perception Theory
| Original item | Final variable | Role within model |
|---|---|---|
| To what extent have you used a face mask? (4-point scale) | Reported use of face mask | |
| To what extent have you washed your hands for at least 40 seconds? (4-point scale) | Reported hand washing | |
| To what extent do you avoid touching your face, especially your eyes, mouth or nose? (4-point scale) | Reported avoidance of touching the face | Behaviour |
| To what extent do you avoid going outside? (4-point scale) | Reported social distancing | |
| To what extent have you asked others to implement prevention behaviours? (4-point scale) | Report of asking others to follow prevention behaviours | |
| To what extent do you intend to use a face mask? (4-point scale) | Intention of using a mask | |
| To what extent do you intend to wash your hands for at least 40 seconds? (4-point scale) | Intention of hand washing | Intention |
| To what extent do you intend to avoid touching your face, especially your eyes, mouth and nose? (4-point scale) | Intention of avoid touching the face | |
| To what extent do you intend to avoid going outside? (4-point scale) | Intention of social distancing | |
| To what extent do you intend to ask others to implement prevention behaviours? (4-point scale) | Intention of asking others to follow prevention behaviours | |
| To what extent do your friends and family think the following behaviours are useful to prevent covid-19? Use a face mask/ wash their hands for at least 40 seconds; avoid touching their faces, especially eyes, mouth or nose; avoid going outside and Asking others to implement prevention behaviours. (4-point scale per behaviour) | Perceived effectiveness of prevention behaviours as perceived by others | Social norms |
| How much do you trust scientists? (4-point scale) | Trust in science | |
| How much do you trust the national government? (4-point scale) | Trust in the national government | |
| How much do you trust people in general? (4-point scale) | Trust in people in general | |
| How much do you trust the local government? (4-point scale) | Trust in the local government | |
| How much do you trust healthcare professionals? (4-point scale) | Trust in healthcare professionals | |
| Why are you implementing prevention behaviours? Is it to avoid conflicts with others or conflicts with the law (fines, detention…)? (4-point scale per motivation) | Motivation to avoid conflicts | |
| Why are you implementing prevention behaviours? Is it to avoid being sick or getting other people sick (4-point scale per motivation) | Motivation to prevent contagion in general | |
| To what extent do you think the following behaviours are useful in preventing covid-19? Use a face mask/ wash their hands for at least 40 seconds; avoid touching their faces, especially eyes, mouth or nose; avoid going outside and asking others to implement prevention behaviours. (4-point scale per behaviour) | Perceived effectiveness of prevention behaviours as perceived by the self | Attitudes |
| To what extent do you feel capable of carrying out the following actions? Use a face mask/ wash their hands for at least 40 seconds; avoid touching their faces, especially eyes, mouth or nose; avoid going outside and asking others to implement prevention behaviours. (4-point scale per behaviour) | Perceived capacity to carry out a prevention behaviour | |
| To what extent do you feel capable of recovering after a severe illness or difficulties or adjusting to changes? (4-point scale per behaviour) | Self-efficacy: perceived ability to bear major problems in general | Perceived Behavioural Control |
| To what extent do you consider the following as barriers to carry out prevention behaviours: Accessibility to masks, others’ attitudes towards prevention behaviours, information or advice by the authorities, information or advice in social media, and family and friends’ attitudes? (4-point scale per aspect) | Perceived barriers to access | |
| How severe do you think your symptoms will be if you/ your loved ones were to catch covid-19 in the future? (5-point scale per group) | Perceived severity of covid-19 contagion | Risk |
| How likely is it that you/ your loved ones will catch covid-19 in the future (5-point scale per group) | Perceived probability of covid-19 contagion |
Multiple mediation analysis4
Following TPB, we fitted several structural equations models to test the hypothesized multiple mediations, namely, that the link between Social Norms and Attitudes and reported behaviour is mediated by intent to carry out the considered behaviour while the link between Perceived Behavioural Control and reported behaviour is only partially mediated by intent. Also, following specific results on risk perception about COVID-19 (Trifiletti et al., 2021), we included risk variables as directly relating to reported behaviour rather than being mediated by intent. We fit identical models for every prevention behaviour: washing hands, avoiding touching the face, wearing a face mask, social distancing and asking others to adopt prevention behaviours (figures 1-5). For all models, we report observed coefficients of the relationship between variables and overall goodness-of-fit measures. Literature suggests that acceptable goodness-of-fit measures are CFI > 0.9; TLI > 0.9 and RMSEA < 0.08 (Crede & Harms, 2019; Kyriazos, 2018). All assumptions checks are freely available on the OSF page of this project (see above).

Wearing a Face Mask
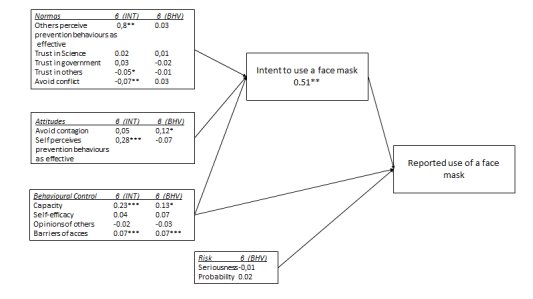
The Structural Equation Model for the reported use of a face mask suggests a partial mediation effect of intent on capacity (ADE = 0.13; IC (95 %) = [0.008; 0.256]; p = 0.04; ACME = 0.233; IC (95 %) = [0.151; 0.316]; p < 0.001), being motivated to prevent contagion (ADE = 0.12; IC (95 %) = [0.019; 0.231]; p = 0.002; ACME = 0.206; IC (95 %) = [0.138; 275]; p < 0.001), whether others perceive prevention behaviours as effective (ADE = 0.08; IC (95 %) = [0.024; 0.256]; p = 0.139; ACME = 0.082; IC (95 %) = [0.024; 0.140]; p = 0.01) and perceived barriers (ADE = 0.13; IC (95 %) = [0.022; 0.116]; p < 0.001; ACME = 0.073; IC (95 %) = [0.043; 0.104]; p < 0.001). Overall goodness-of-fit measures sug- gest a good fit to the data (X (2) = 1.662; p = 0.43; CFI = 1; TLI = 1.008; RMSEA < 0.001).
Washing Hands
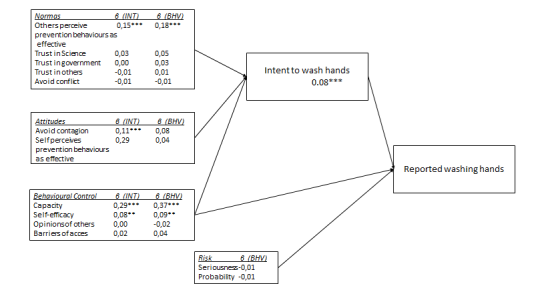
The Structural Equation Model for the reported handwashing also suggests partial mediations for capacity (ADE = 0.582; IC (95 %) = [0.476; 0.698]; p < 0.001; ACME = 0.286; IC (95%) = [0.206; 0.376]; p < 0.001), self-efficacy (ADE = 0.092; IC (95%) = [0.003; 0.181]; p = 0.043; ACME = 0.081; IC (95 %) = [0.019; 0.143]; p < 0.001), motivation to avoid conflicts (ADE = -0.062; IC (95%) = [-0.110; -0.016]; p = 0.009; ACME = -0.043; IC (95%) = [-0.077; -0.011]; p = 0.009) and whether others believe prevention measures are effective (ADE = 0.18; IC (95 %) = [0.1; 0.261]; p < 0.001; ACME = 0.149; IC (95 %) = [0.092; 0.206], p < 0.001). Overall goodness-of-fit measures suggest a relatively poor fit of the whole model to the data (X (3) = 144; p < 0.001; CFI = 0.835; TLI = 0.591; RMSEA = 0.225).
Avoiding Touching the Face
The Structural Equation Model for the report- ed avoidance of touching the face suggests partial mediation for both capacity (ADE = 0.789; IC (95 %) = [0.659; 0.919]; p < 0.001; ACME = 0.433; IC (95 %) = [0.338; 0.529]; p < 0.001) and whether others believe prevention behaviours are effective (ADE = 0.098; IC (95 %) = [0.007; 0.188]; p = 0.034; ACME = 0.102; IC (95 %) = [0.035; 0.170]; p = 0.003). Overall goodness- of-fit measures suggest an acceptable fit to the data (X (3) = 67.3; p < 0.01; CFI = 0.909; TLI = 0.124; RMSEA = 0.152).
Social Distancing
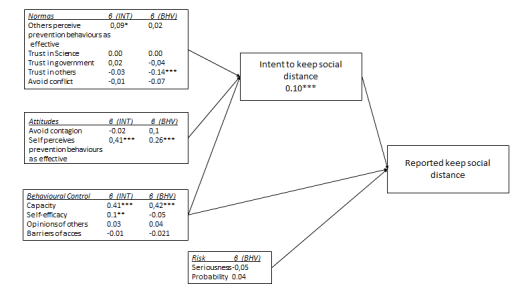
As before, the structural Equation model for social distancing suggests a partial mediation for capacity (ADE = 0.424; IC (95 %) = [0.294; 0.555]; p < 0.001; ACME = 0.407; IC (95 %) = [0.307; 0.508]; p < 0.001) and whether others believe prevention behaviours are effective (ADE = 0.26; IC (95 %) = [0.120; 0.399]; p = 0.034; ACME = 0.014; IC (95 %) = [0.017; 0.159]; p = 0.003). Overall goodness-of-fit measures suggest a good fit to the data (X (3) = 22.18; p < 0.001; CFI = 0.965; TLI = 0.665; RMSEA = 0.083).
Asking Others to Adopt Prevention Behaviours
Finally, the Structural Equation model for reports of asking others to adopt prevention behaviours suggests a partial mediation for capacity (ADE = 0.565; IC (95 %) = [0.437; 0.692]; p < 0.001; ACME = 0.468; IC (95 %) = [357; 579]; p < 0.001), opinions of others around (ADE = 0.137; IC (95 %) = [0.059; 0.214]; p < 0.001; ACME = 0.173; IC (95 %) = [0.105; 0.242]; p < 0.001) and whether the self perceives prevention behaviours as effective (ADE = 0.326; IC (95 %) = [0.219; 0.433]; p < 0.001; ACME = 0.444; IC (95 %)= [0.325; 0.563]; p < 0.001). Surprisingly, the model also shows a direct effect of motivation to avoid infection without mediating intention (ADE = 0.326; IC (95 %) = [0.219; 0.433]; p < 0.001; ACME = 0.055; IC (95 %) = [-0.037; 0.148]; p = 0.238). Overall goodness-of-fit measures suggest a good fit to the data (X (3) = 13.12; p = 0.004; CFI = 0.998; TLI = 0.884; RMSEA = 0.06).

Discussion
Here, we analysed the link between variables predicted by the TPB and the intent to adopt prevention behaviours against the COVID-19 pandemic. Prior research shows inconsistent results regarding the effect of risk perception on prevention behaviours (Barakat & Kasemy, 2020; Falco & Zaccagni, 2020; Irigoyen-Camacho et al., 2020; Yildirim & Güler, 2020). Similarly, there are mixed results about what kind of motivations (e.g., protecting others or oneself, a sense of duty or avoiding sanctions) are more effective in motivating the adoption of prevention behaviours (Everett et al., 2020; Hume et al., 2020).
First, we conducted EFAs (Exploratory Factor Analysis) to check the validity of grouping conceptually similar variables into distinct, independent and mediator variables. These EFAs lead us to believe that we cannot assume the existence of a general intention to adopt the prevention behaviours but rather that each intention is a single variable having its own specific set of causes. This conclusion was further supported by the fact that each prevention behaviour exhibited a specific pattern of partially mediated independent variables, which strongly suggests that trying to impact every behaviour with a single intervention is not fruitful. Instead, it is necessary to understand how each behaviour is affected by different factors to intervene effectively. This was a central rationale for our multiple mediation analysis and can guide future intervention designs.
Also, exploratory factor analyses indicated that trust in others is not a single factor but rather distinguished across different (mis)trusted groups. This implies that communications from specifically trusted groups could be effectively used to motivate the adoption of varying prevention behaviours. In addition, motivations to adopt prevention behaviours were divided into motivations to avoid infection and conflicts caused by not implementing prevention behaviours, with the latter seldom being linked to any prevention behaviour. This suggests that punitive policies or fostering interpersonal conflict around COVID-19 is ineffective compared to positive, protection-centred messages (Krpan & Dolan, 2021).
Multiple mediation analyses suggest that there is not a particular pattern of explanatory variables for all prevention behaviours. Rather, each one is predicted by a different set of variables (figures 1-5). First, the intention to wear a face mask is explained by capacity, motivation to avoid contagion and whether others perceive prevention behaviours as effective, which are partially mediated by intent to wear a face mask. Second, the intention to wash hands frequently is positively linked to believing that others consider prevention behaviours effective and capacity, self-efficacy, and motivation to avoid conflicts. These relations are partially mediated by intent. Third, intention to avoid touching the face was explained by capacity and whether others believe prevention behaviours are effective, partially mediated by intent. Fourth, keeping social distance was predicted by capacity and whether others believe prevention behaviours are effective, partially mediated by intent. Finally, asking others for prevention behaviours was predicted by capacity, effectiveness of prevention behaviours perceived by the self and others independently and the motivation to avoid contagion. All variables were partially mediated by intent except for motivation to prevent infection, which was not mediated at all. To our knowledge, prior studies have not directly examined behavioural determinants of different behaviours, implicitly assuming that variables related to a single prevention behaviour apply to all others. Contrary to these, we suggest that public communication should be specifically tailored to specific behaviours based on which ones are more effective or more easily implemented in specific socioeconomic or cultural contexts and on what considerations are more influential in carrying out particular behaviours.
Indeed, while we observed that capacity, whether people feel capable of carrying out prevention behaviours, is linked to all considered behaviours, no other variables were significantly linked to all behaviours. This suggests that while assuring the capacity to carry out desired prevention behaviours is paramount, it is insufficient to ensure widespread adoption. This is highlighted by the fact that some behaviours (i.e., avoiding touching the face or keeping social distance) appear to rely on a limited form of cooperation with others, while other behaviours (i.e., asking others to engage in prevention behaviours) are actually linked to personal belief on the effectiveness of these behaviours irrespective of other’s beliefs.
Also, we observe several surprising non-significant effects. Contrary to classic economic theory but echoing prior results (e.g., Yildirim & Güler, 2020), we failed to find significant correlations between risk and the intent to adopt any prevention behaviours. This is consistent with prior findings where variables measuring risk perception did not significantly correlate with the intention of maintaining the lockdown in a Mexican sample. Still, variables taken from TPB did have a significant correlation (Padilla-Bautista & Galindo-Aldana, 2022). A possible explanation of these results deals with our sample’s sociodemographic characteristics. Most of our participants were healthcare professionals with high educational degrees and socioeconomic status (Table 1). Therefore, they may ignore the risks of serious symptoms.
On the contrary, limiting infections for others, for instance elderly parents, might be more motivating to this sample. This interpretation follows from results suggesting that risk is linked to prevention behaviours only in an older people sample (Irigoyen-Camacho et al., 2020), perceived to be more at risk for COVID-19 (Lekamwasam & Lekamwasam, 2020). This reinforces the notion that a one-size-fits-all communication strategy is not effective. Rather, public communication ought to be tailored to specific behaviours and subsets of the general population whose motivations or possibilities of action can systematically differ in relevant ways.
Another unexpected null result is the limited effect of trust in different groups. Prior studies suggest that trust in the central government is positively linked to recommended and excessive prevention behaviours (Min et al., 2020). However, trust in any group was not linked to any prevention behaviour in our sample. This may be related to low institutional trust in Colombia (Alcaldía Mayor de Bogotá, 2020; Ali et al., 2021; Edelman Foundation, 2021). In this sense, our results could be opposed to prior research showing that national identity and other political variables significantly predict adopting prevention behaviours (Van Bavel et al., 2020b), making regional or family identities more relevant in this context.
Interestingly, these null findings do not deal with others’ perceptions of effectiveness, which were linked to several prevention behaviours. Participants did not require social cohesion or trust in others to adopt prevention behaviours but rather simply the second-order belief that others think prevention behaviours are effective irrespective of whether they trusted others. It appears that COVID-19 prevention is not an issue of group identity and cohesion rather of simple instrumental coordination of empirical beliefs (i.e., whether prevention behaviours are effective) in this sample. This may not foster long-standing cooperation but, optimistically, might be more readily manipulated to combat future pandemics.
Overall, our results imply significant consequences to designing public communications around COVID-19. First, the necessity of having a differential approach to the different prevention behaviours. Following TPB, our study indicates that it is possible to achieve behaviour change by correctly understanding how the intention to adopt each behaviour is associated with a different set of variables, including perceptions of self-control, different motivations and perceived norms. Second, we found partial mediation effects of capacity for all considered behaviours, which indicates that proper public policy minimally requires ensuring people are able to carry out desired behaviours, for instance, through the free distribution of face masks or universal access to clean water. In this sense, our results echo prior meta-analyses highlighting the importance of perceived control on the intent to implement prevention behaviours (Fischer & Karl, 2020). Finally, communication-based on risk or public trust is, at best, useless since these variables are unrelated to any reported prevention behaviours. We hope that these results directly impact public communication around COVID-19. Behavioural sciences interventions using communication strategies have been successful in changing behaviours when they are based on diagnoses that precisely identify motivational factors of these behaviours (Jordan et al., 2012; Keller & Brown, 2002; La Ferrara et al., 2008; Paluck, 2009; Schultz et al., 2007). In this context, we hope our results directly impact public communication around COVID-19. This impact should be measurable in terms of actual change in behaviours. Hence, this article is accompanied by a policy brief intended to inform public policy in an easier-to-grasp format (see online supplementary material).
We consider that our results can be used to inform public policy aiming at increasing adherence to prevention behaviours in the contention and management of COVID-19 and future pandemics. Future interventions should aim separately at each target health behaviour and what motivates its compliance the most (e.g., self-efficacy vs subjective norms vs attitudes towards the behaviour). For instance, our results suggest that the use of a face mask is mainly influenced by perceptions of effectiveness of prevention behaviours as perceived by the self and by others (Figure 1), whereas washing hands is much more linked to the motivation to avoid contagion and whether others (not the self) perceive this as effective to prevent COVID-19 (Figure 2). In this sense, public communication aiming specifically at mask use ought to highlight both that it is an effective way to prevent COVID-19 (effectiveness as perceived by the self) and that others think so (effectiveness as perceived by others). On the contrary, communications aimed at washing hands ought only to focus on washing hands to prevent COVID-19 (effectiveness as perceived by the self), not whether others agree with this.
As mentioned, our results are limited by a relatively homogeneous and non-representative sample. Even though our results cannot be generalized to the general population, they reflect a subset of great importance in the context of the pandemic. That is, the segment of the population targeted by the economic reactivation and who are more at risk. We believe the results presented above can be helpful in guiding effective communication to motivate people to adopt prevention behaviours consistently. Our data and results were obtained in a sample of participants. Most of them had basic economic and educational conditions to access prevention behaviours, as shown in Table 1. However, these socio-economic conditions must be considered while designing possible interventions, as our conclusions may not apply to less favoured groups. Any intervention based on our results ought to carefully consider cultural or group differences especially pertaining to access to different prevention behaviours (e.g., whether the target group actually has access to running water and soap to wash their hands regularly) as well as cultural practices or beliefs that may help or hinder the effective acquisition of these behaviours. In addition, we reiterate the importance of minimizing systematic barriers that prevent the achievement of different health behaviours. We warn that motivating different population segments, such as teenagers or less educated people, may require different communication strategies and ought to be based on careful analysis of these specific populations. We believe that relatively poor goodness-of-fit measures for all considered multiple mediation models can be interpreted considering this limitation. Indeed, we observe two contrasting findings. First, there is an empirically robust relation between considered TPB variables and reported adoption of prevention behaviour. This follows the expected results from the reviewed literature on TPB and health behaviours (Armitage & Conner, 2001; Fischer & Karl, 2022). On the other hand, theoretically driven models consistently offered relatively poor goodness-of-fit measures. We interpret these apparently incompatible results as reflecting several unobserved variables that may explain the reported adoption of health behaviours but were not considered in collected data and, therefore, unobserved. Future studies should explore these variables, for instance, neuropsychological constructs (Nurse et al., 2022; Xie et al., 2020), personality (Pfattheicher et al., 2020) or sociodemographic variables (Barrios & Hochberg, 2020; Jennings et al., 2021).
It is worth mentioning that collected data is not longitudinal or experimental so we cannot unequivocally affirm directional causal relations between variables. Tested directional claims are solely based on theoretical grounds (Ajzen, 1991, 2006, 2011) pending experimental or longitudinal research. This was partially answered by the longitudinal research made by Padilla-Bautista and Galindo-Aldana (2022) , showing that the behavioural intention to maintain the lockdown remained significant 46 days after the first assessment only in people with positive attitudes towards the lockdown and with high behavioural control. Finally, we believe that our findings may be relevant for public communication due to the great difficulty of obtaining these data and the pressing need for scientifically informed public policy. Nevertheless, these communications and their actual impact on COVID-19 and future pandemics ought to be rigorously evaluated and adapted to limit the disease’s progression and save count-less lives.

