










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Facultad de Odontología Universidad de Antioquia
versão impressa ISSN 0121-246X
Rev Fac Odontol Univ Antioq v.22 n.1 Medellín jul./dez. 2010
ARTÍCULOS ORIGINALES DERIVADOS DE INVESTIGACIÓN
A retrospective characterization study on patients with oral clefts in Medellín, Colombia, South America1
Un estudio retrospectivo de caracterización en pacientes con fisuras orales en Medellín, Colombia, Suramérica
Ana María Cerón Zapata2; Ana María López Palacio3; Gloria María Aristizábal Puerta 4; Carolina Uribe Álvarez5
1 This article was written in partial fulfillment of the requirements for the degree of Especialista clínico en Odontología Integral del Niño y Ortopedia Maxilar
2 D.D.S. Pediatric Dentist. Assistant professor and researcher at the Facultad de Odontología, Universidad de Antioquia, Medellín city, Colombia, South America
3 D.D.S. Pediatric dentist. Assistant professor and researcher at the Facultad de Odontología, Universidad de Antioquia, Medellín city, Colombia, South America
4 D.D.S. Pediatric dentist, Universidad de Antioquia
5 D.D.S. Pediatric dentist, Universidad de Antioquia
ABSTRACT
INTRODUCTION: the objective of this study was to make a clinical and epidemiological characterization of the patients with cleft lip and/or palate (CLP) who consulted at the Childrens Hospital Clínica Noel Foundation of Medellín, Colombia, South America, between 1985 and 2003.
METHODS: 919 clinical records were evaluated for a descriptive, longitudinal, retrospective study. A univariate statistical analysis was used for the qualitative variables, and descriptive measures for the quantitative ones. A two-variate statistical analysis was performed in order to determine the association among the qualitative variables with a significance level of 5%.
RESULTS: 50.3% of the cases were classified as unilateral and 19.8% as bilateral. Among the unilateral ones, 59.0% were located at the left side and 41.3% at the right side. 3.4% presented cleft lip, 12.4% presented cleft palate, and 12.8% presented cleft soft palate. 1.2% of the sample did not present pathology classification. In terms of gender, males represented 48.0% and females 38.1%; no data was found in 13.9% of the cases. Concerning location, 87.3% of the patients came from the State of Antioquia. As for age at the time of admission to the institution, 44.3% of the children were less than thirty days old. Most parents were between nineteen and thirty years old. Most medical records did not show reports on the father or mothers family history, diseases during pregnancy or tobacco and alcohol consumption during pregnancy.
CONCLUSIONS: this study evaluated the clinical records used at the Clínica Noel Foundation. As a result, we recommend to homogenize the professionals who fill in the records and to standardize the instruments in order to generate reliable databases for future research.
Key words: cleft lip and palate, epidemiological characterization.
RESUMEN
INTRODUCCIÓN: el objetivo de este estudio consistió en caracterizar clínica y epidemiológicamente pacientes con labio y/o paladar hendido (LPH) que consultaron el Hospital Infantil Clínica Noel de Medellín, Colombia, entre 1985 y 2003.
MÉTODOS: se evaluaron 919 historias clínicas, para un estudio de tipo descriptivo, longitudinal y retrospectivo. Se realizó un análisis univariado para las variables cualitativas, y medidas descriptivas para las variables cuantitativas. Se realizó análisis bivariado para determinar la asociación entre las variables cualitativas con un nivel de significancia del 5%.
RESULTADOS: 50,3% de los casos fueron clasificados como unilaterales y 19,8% como bilaterales. Dentro de los unilaterales, el 59,0% se presentaron al lado izquierdo y el 41,3% al lado derecho. El 3,4% presentó labio hendido, el 12,4% presentó paladar duro hendido, y el 12,8% presentó paladar blando hendido. El 1,2% de la muestra no incluía clasificación de la patología. En cuanto al sexo, los hombres representaron 48,0% y las mujeres 38,1%; no se encontraron datos en el 13,9%. El 87,3% de los pacientes provenían del departamento de Antioquia. La edad predominante de ingreso a la Fundación fue antes de treinta días de nacido. La mayoría de los padres estaban entre diecinueve y 30 años de edad. La mayoría de las historias clínicas no tenían reporte acerca de historia familiar de la madre y el padre, enfermedades sufridas durante el embarazo o consumo de cigarrillo y bebidas alcohólicas durante el embarazo.
CONCLUSIONES: este estudio permitió evaluar la historia clínica usada en la Fundación Clínica Noel. Se sugiere calibrar los profesionales que diligencian los registros, y estandarizar los instrumentos para generar una base de datos confiable para futuras investigaciones.
Palabras clave: labio y paladar hendido, caracterización epidemiológica.
INTRODUCCIÓN
The nasal-labial-alveolar-palatal clefts are congenital cranial facial anomalies, produced by embryologic defects in face formation, affecting the upper lip, the pre-maxilla, the hard palate and/or the floor of the nasal cavity. The cleft lip with or without cleft palate is the most common of the oral facial congenital anomalies in new born babies.1, 2 A prevalence has been reported varying from 0.19 to 2.69 per 1000 new born babies in different parts of the world.3 The prevalence is affected by gender, type of fissure, and race.4 Besides, the estimates in prevalence and incidence vary. There is no efficient universal single registration system accepted for oral fissures.5
An incidence of 0.55-2.50:1000 births for the Mongolian race has been reported, as well as 1.65- 2,71:1000 for the Japanese, 0,69-2.35:1000 for the Caucasian, and 0.18-0.82:1000 for Blacks.6 In Latin America, 0,87:1000 births have been reported with cleft lip with or without cleft palate, and 0,13:1000 with cleft palate.7
In the different clinical studies reported, the etiological factors of cleft lip, with or without cleft palate, cannot be determined exactly; therefore, we limit our study to classifying them as multi-factor hereditary dependant on multiple genes with an established family tendency. Recent literature has reported a complex etiology with multiple loci, genetic and environmental factors influencing individual susceptibility.8
There are several teratogenic agents and factors during pregnancy associated with formation of CLP, such as cortisone, anticonvulsants, salicylate, vitamin A, aminopterin, busalfan, organic solvents, maternal smoking, maternal hypoxia, maternal rubella, maternal diabetes mellitus, hypobaric hypoxia, and low social economical status. Other related variables include increased paternal and maternal age.9, 10
Due to the complexity of the anatomical and functional alterations of patients with CLP, a multidisciplinary group treatment is required since the very first days of birth.11
The Childrens Hospital Clínica Noel Foundation, located in the city of Medellín, Colombia, South America, treats patients with CLP under the supervision of a multi-disciplinary team since 1977, and since 1985 the Pediatric Dentistry Section makes part of this group. The institution seeks a comprehensive management in order to rehabilitate the patients.
The objective of this study was to clinically and epidemiologically characterize the patients with cleft lip and/or palate who consulted the Clínica Noel Foundation of Medellín, during the period 1985-2003.
MATERIALES Y MÉTODO
This study was conducted in Medellín, a Colombian city with a population of about 4.000.000 people. All the cases included in this study were collected from the medical and dental records of Clínica Noel Foundation, where Universidad de Antioquia has worked with Pediatric Dentistry residents since 1985.
Data Collection
A total of 919 non-syndromic cleft lip and palate patients medical and dental records from 1985 to 2003 were retrospectively analyzed according to the following variables: type of cleft, gender, state of origin, age at admission to the Clinic, mothers age, fathers age, mothers family history of CLP, fathers family history of CLP, mothers diseases during pregnancy, and tobacco and alcohol consumption by the mother during pregnancy.
This is a descriptive, longitudinal, retrospective type of study. The clinical records were examined consecutively and in alphabetical order, and all of them were registered, even those lacking data. The records were in the active files of the institution, and they all were double screened.
Statistical Analysis
The database of patients was entirely transferred to a Window-based personal computer, and statistical analysis was carried out using the Statistical Package for the Social Sciences (SPSS Inc, version 14.0, Chicago IL). The database was made under EPI INFO 6.04.A univariate statistical analysis was performed, allowing the characterization of patients with CLP, and it was confirmed by means of frequency tables with their respective percentages for the qualitative variables and descriptive measurements, such as averages, standard deviations, and medians for the quantitative variables. Additionally, a bivariate analysis was performed in order to determine association among the qualitative variables through the Chi-square test for independent variables. A 5% statistical level of significance was used.
RESULTADOS
1. Type of cleft
Unilateral cleft lip and palate: 50.3% of the cases were classified as unilateral; of these, 59.0% were located on the left side and 41.3% on the right side. There was a 0.7% without classification of the side affected.
Bilateral cleft lip and palate: 19.8% of the cases presented bilateral cleft.
Cleft lip: 3.4% presented cleft lip.
Cleft palate: 12.4% presented cleft hard palate.
Soft palate: 12.8% presented cleft soft palate.
1.2% of the clinical records had no classification.
2. Gender ratio among cases
441 (48.0%) patients were males and 350 (38.1%) were females. 128 medical records had no gender data, which corresponds to 13.9% of the total.
3. States of origin
The patients were from several Colombian states, as shown in (table 1).
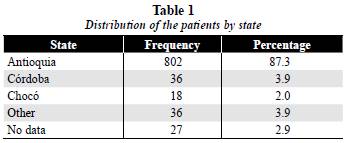
Note that 87.3% of the patients were from Antioquia, the state where the Foundation is located.
4. Age at the time of admission to the Clinic
The analysis was carried out by age groups, taking into account the surgical protocol used in the Clinic (table 2).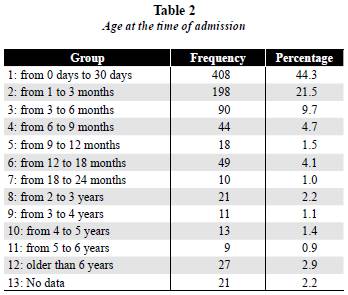
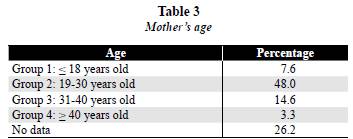
5. Mothers age
Five groups were classified by age. Group 1, mothers under eighteen years of age; group 2, mothers from nineteen to thirty years old; group 3, mothers from thirty one to forty years old; group 4, mothers older than forty, and group 5 with no data in the clinical record.
The mothers between nineteen and thirty years of age presented the highest frequency, 48.0%. The next group was the one of mothers between thirtyone and forty years of age, 14.6%. Mothers under eighteen showed a percentage of 7.6%, and mothers older than forty, a percentage of 3.3%. Those with no data in the clinical record, 26.2%. The average age was 26.40 ± 7.0 (N.D.) (table 3).
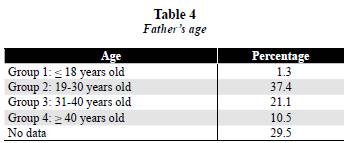
6. Fathers age
The same age groups for the mothers were established for the fathers. Fathers between nineteen and thirty years of age presented the highest frequency, 37.4%. The next group is the one of fathers between thirtyone and forty years of age, with a percentage of 21.1%. Fathers under eighteen years of age showed a percentage of 1.3%, and fathers older than forty presented a percentage of 10.5%. Those with no data in the clinical records, 29.5%. The average age was 31.27 ± 8.0 (N.D.) (table 4).
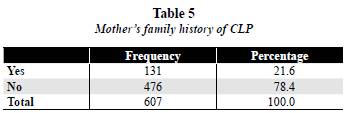
7. Mothers family history of CLP
The family history was positive in 21.6% and negative in 78.4% of the cases. 33.9% of the medical records did not have this information (table 5).
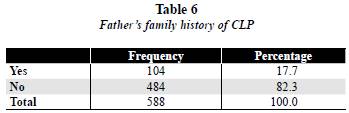
8. Fathers family history of CLP
The family history was positive in 17.7% and negative in 82.3% of the cases. 36.0% of the medical records did not have this information (table 6).
9. Diseases suffered by the mother during pregnancy
The diseases associated with pathologies were taken into account, and the following results were obtained:
No diseases: 355 mothers (38.6%).
Chicken Pox: 5 mothers (0.5%).
Toxoplasmosis: 2 mothers (0.2%).
Syphilis: 4 mothers (0.4%).
Rubella: 3 mothers (0.3%).
Other diseases: 63 mothers (6.9%). Out, of these, the most common was urinary infection with 6 cases reported.
No data: 487 clinical records (53.0%).
10. Tobacco consumption by the mother
There was no registration of this information in the clinical records of 839 patients (91.3%). There was no tobacco consumption in 70 patients (7.6%).
There was tobacco consumption in 10 patients (1.1%).
11. Alcohol consumption by the mother
No information was found in 844 clinical records (91.8%).
There was no alcohol consumption in 71 patients (7.7%).
There was alcohol consumption in 4 patients (0.4%).
DISCUSIÓN
There has been no reliable information about the incidence of oral clefts in Colombia, S.A., due to the lack of a well established and continuous national registration system. The cases described in this study were collected from the clinical records of Clínica Noel Foundation in Medellín, Colombia, S.A. This institution is considered one of the main reference centers for patients with CLP in the State of Antioquia, which is the second one in population density in the country. It receives patients from many nearby provinces with a low socio-economical level. The institution counts on a multidisciplinary group for the treatment of CLP patients; it has been in service for the past twenty-five years.
After making the clinical and epidemiological characterization of the patients with cleft palate and/or lip that attended Clínica Noel Foundation in Medellín during the period of 1985 to 2003, it was found out that left cleft lip and palate is the most common type of cleft, with 59%, thus corroborating the reports by Rajabian and Sherkat, Hagberg et al., and Meng et al.9, 12, 13
Regarding the presence of the alteration in terms of gender, it is observed that it predominates in males, confirming what has been reported by several studies of different geographical regions and ethnical groups.7, 9, 12, 14, 15
It was observed that the State of Antioquia presented the highest number of cases. This is due to the fact that access to the clinic is easy, since it is located in the main city of the state, and health institutions in the area recognize the Clínica Noel as a reference center for the treatment of this alteration.
It was also noticed that the patients with this alteration came to the clinic at an early age (less than one month: 44.3%) to begin all the diagnostic and treatment procedures, which improved the prognosis of comprehensive rehabilitation. Weil, Mishima, Grayson and Cutting reported a functional and anatomical improvement in those patients in which orthopedic appliances were installed at an early age, preferable at 48 hours after birth or during the first days of life.16-18
The mothers age has been widely studied as a risk factor for oral clefts, but the results have been contradictory. This study, even though 26.2 and 29.5% of the information regarding mothers and fathers age respectively was not registered on the clinical records, found out that the population group with mothers and fathers whose age ranged from nineteen to thirty years were the most frequent. Viera et al reported in a meta-analysis that there is no association between a higher mothers age and the presence of isolated forms of cleft palate and/or lip. González- López et al presented that the average mothers age in a Mexican population was twenty-seven years. Regarding paternal age, Bille et al. reported an association between a higher paternal age and higher risk of cleft palate. González-López et al presented that the average age in a Mexican population was 29.5 years.19-21
Marazita et al, Moreno et al, and Christensen reported a genetic association as a risk factor for patients with CLP. Multi generation studies have found out that this recurrence is associated with dominant autosome inheritance. This study did not find familial aggregation; however, it is not possible to get to a conclusion, due to the lack of information in the clinical records.8, 22, 23
Several authors have reported some teratogenic agents and factors during pregnancy that could lead to the presence of a cleft; also, the use of cortisone, anticonvulsants, tobacco, and alcohol, as well as diseases such as diabetes mellitus and epilepsy, and external factors like hyperthermia and infections, could be of risk. However, this study did not find information on the clinical records that could allow us to conclude this relationship.12, 20, 24-28
CONCLUSIONES
The retrospective studies in which the main objective is to characterize the population attending the CLP clinical patients centers are difficult. One of the main difficulties is to obtain precise and well processed data. This particular study reviewed the clinical records of patients with this pathology. Data such as family history, alcohol and tobacco consumption, and exposure to pesticides by mothers were not always included in the anamnesis of the clinical records.
Ideally, epidemiological studies should be carried out with a prospective methodology, in a way that includes all the information required by this type of analysis. Whenever possible, there must be a control group in the study design.
It is important that the centers treating this kind of patients in our country generate reliable epidemiological data under the same criteria, allowing comparison between our population and that of other countries.
In summary, this study evaluated the clinical records used during 18 years at Clínica Noel Foundation. It is suggested then to standardize the practitioners who fill in these records and to calibrate and systematize the instruments. This will allow an improvement of treatment guidelines. It will also strengthen the comprehensive treatment of patients, identify the risk factors, and generate a database for future research. The Clinical Records Board of the Clínica Noel Foundation has received the recommendations and they will be evaluated in ten years.
REFERENCIAS
1. Derijcke A, Eerens A, Carels C. The incidence of oral clefts: a review. Br J Oral Maxillofac Surg 1996; 34: 488-494. [ Links ]
2. Tolarova MM, Cervenka J. Classification and birth prevalence of orofacial clefts. Am J Med Genet 1998; 75: 126-137. [ Links ]
3. Loffredo Monteiro L, Freitas JA, Grigolli AA. Prevalence of oral clefts from 1975 to 1994, Brazil. Rev Saude Publica 2001; 35: 571-575. [ Links ]
4. Vanderas AP. Incidence of cleft lip, cleft palate and cleft lip and palate among races: a review. Cleft Palate Craneofac J 1987; 24: 216-225. [ Links ]
5. Schwartz S, Papal JT, Rajchgot H, Roberts GL. Accurate and systematic numerical recording system for the identification of various types of lip and maxillary clefts (RPL system). Cleft Palate Craniofac J 1993; 30(3): 330-332. [ Links ]
6. Gundlach KKH, Maus C. Epidemiological studies on the frequency of clefts in Europe and world-wide. J Craniomaxillofac Surg 2006, 34 Supl S2: 1-2. [ Links ]
7. Menegotto BG, Salzano FM. Epidemiology of oral clefts in a large South American sample. Cleft Palate Craniofac J 1991; 28(4): 373-376. [ Links ]
8. Marazita ML, Murray JC, Lidral AC, Arcos-Burgos M, Cooper ME, Goldstein T et al. Meta-analysis genome scans reveals multiple cleft lip/palate genes with novel loci on 9q21 and 2q32-35. Am J Hum Genet 2004; 75: 161-173. [ Links ]
9. Rajabian MH, Sherkat M. An epidemiological study of oral clefts in Iran: analysis of 1669 cases. Cleft Palate Craniofac J 2000; 37: 191-196. [ Links ]
10. Polenta FA, Castilla EE, Orioli IM, López-Camelo JS. Regional analysis on the occurrence of oral clefts in South America. Am J Med Genet 2007; 143 A: 3216-3227. [ Links ]
11. Strauss RP. The organization and delivery of craniofacial health services: the state of the art. Cleft Palate Craniofac J 1999; 36(3): 189-195. [ Links ]
12. Hagberg C, Larson O, Milerad J. Incidence of cleft lip and palate and risk of additional malformation. Cleft Palate Craniofac J 1997; 35: 40-45. [ Links ]
13. Meng T, Shi B, Zheng Q, Wang Y, Li S. Clinical and epidemiologic studies on nonsyndromic cleft lip and palate in China. Analysis of 4268 cases. Ann Plast Surg 2006; 57: 264-269. [ Links ]
14. Cooper ME, Stone RA, Liu Y, Hu DN, Melnick M, Marazita ML. Descriptive epidemiology of nonsyndromic cleft lip with or without cleft palate in Shanghai, China, from 1980 to 1989. Cleft Palate Craniofac J 2000; 37: 274-280. [ Links ]
15. Zhou Q, Shi B, Shi Z, Zheng Q, Wang Y. Survey of the patients with cleft lip and palate in China who were funded for surgery by the Smile Train program from 2000 to 2002. Chin Med J 2006; 119: 1695-1700. [ Links ]
16. Weil J. Orthopaedic growth guidance and stimulation for patients with cleft lip and palate. Scand J Plast Reconstr Surg 1987; 21: 57-63. [ Links ]
17. Mishima K, Sugahara T, Yoshihide M, Sakuda M. Threedimensional comparison between the palatal forms in complete unilateral cleft lip and palate with and without Hotz Plate from Cheiloplasty to palatoplasty. Cleft Palate Craniofac J 1996; 33: 312-317. [ Links ]
18. Grayson BH, Cutting CB. Presurgical nasoalveolar orthopedic molding in primary correction of the nose, lip, and alveolus of infants born with unilateral and bilateral clefts. Cleft Palate Craniofac J 2000; 38: 193-198. [ Links ]
19. Vieira AR, Orioli IM, Murria JC. Maternal age and oral clefts: a reappraisal. Oral Surg Oral Med Oral Pathol Radiol Endod 2002; 94: 530-535. [ Links ]
20. González BS, López ML, Rico MA, Garduño F. Oral clefts: a retrospective study of prevalence and predisposal factors in the State of México. J Oral Sci 2008; 50: 123-129. [ Links ]
21. Bille C, Skytthe A, Vach W, Knudsen LB, Andersen AM, Murray JC et al. Parents age and the risk of oral clefts. Epidemiology 2005; 16: 311-316. [ Links ]
22. Christensen K. The 20th century Danish facial cleft population-epidemiological and genetic-epidemiological studies. Cleft Palate Craniofac J 1999; 36: 96-104. [ Links ]
23. Moreno LM, Arcos-Burgos M, Marazita ML, Krahn K, Maher BS, Cooper ME et al. Genetic analysis of candidate loci in non-syndromic cleft lip families from Antioquia- Colombia and Ohio. Am J Med Genet 2004; 125: 135-144. [ Links ]
24. Peterka M, Tvdek M, Likovsky A, Peterková R, Fára M. Maternal hyperthermia and infection as one of possible causes of orofacial clefts. Acta Chir Plast 1994; 36: 114-118. [ Links ]
25. Chung KC, Kwalski CP, Kim HM, Buchman SR. Maternal cigarette smoking during pregnancy and the risk of having a child with cleft lip/palate. Plast Reconstr Surg 2000; 105: 485-491. [ Links ]
26. Spilson SV, Kim HJ, Cheng KC. Association between maternal diabetes mellitus and newborn oral cleft. Ann Plast Surg 2001; 47: 477-481. [ Links ]
27. Lorente C, Cordier S, Bergeret A, De Walle HE, Goujard J, Ayme S et al. Maternal occupational risk factors for oral clefts. Occupational exposure and congenital malformation working group. Scand J Work Environ Health 2000; 26: 137-145. [ Links ]
28. Natsume N, Kawai T, Ogi N, Yoshida W. Maternal risk factors in cleft lip and palate: case control study. Br J Oral Maxillofac Surg 2000; 38: 23-25. [ Links ]
RECIBIDO: AGOSTO 13/2010 - ACEPTADO: SEPTIEMBRE 21/2010
CORRESPONDENCIA
Ana María Cerón Zapata Address: Calle 64 N.º 52-59, Medellín, Colombia, South America Telephone number: (57 4) 219 53 30 Fax number: (57 4) 219 53 32 Email address: anamceron@odontologia.udea.edu.co
Cerón AM, López AM, Aristizábal GM, Uribe C. A retrospective characterization study on patients with oral clefts in Medellín, Colombia, South America. Rev Fac Odontol Univ Antioq 2010; 22(1): 81-87.
Cerón AM, López AM, Aristizábal GM, Uribe C. Un estudio retrospectivo de caracterización en pacientes con fisuras orales en Medellín, Colombia, Suramérica. Rev Fac Odontol Univ Antioq 2010; 22(1): 81-87.

