











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink
Introduction
Chest trauma is one of the most common causes of death, accounting for 20 to 25% of cases1. It can be due to blunt or penetrating trauma. Most patients (85%), can be treated with just a closed chest drainage, and only 10 to 15% of these patients will need an emergency thoracotomy2.
Cardiac hernia is a rare clinical condition, diagnosis based on clinical findings, and even through suggestive signs on computed tomography is very difficult, and can be neglected in the preoperative period very easy3.
Our objective in this case report is to present an example of how to perform a challenging thoracic drainage in a patient with cardiac hernia diagnosed preoperatively, based on computed tomography findings.
Case report
A 45-year-old male was brought to our emergency service by the emergency medical service - SAMU, immobilized on a rigid board and cervical collar. The patient fell down from a 7-meter-high lamppost hitting the ground on his back.
On arrival he was complaining of shortness of breath, confused, with blood pressure (BP) of 110/70 mmHg, heart rate of 115 beats/min, respiratory rate of 25 breaths/min, and oxygen saturation of 97%.
The physical examination revealed:
a. Pervious airways, without neck pain;
b. Swollen chest; on palpation a subcutaneous emphysema throughout the anterior chest wall was observed; breath sounds slightly decreased bilaterally;
c. Flat and flaccid abdomen, negative FAST in all three abdominal regions, the cardiac site was unable to visualize due to subcutaneous emphysema; pelvis stable, with no signs of external bleeding;
d. Glasgow 14 (lost point in verbal response); isochoric pupils and photo reactive;
e. No deformities in the upper and lower limbs, clear on his back, and no sensitivity or movements below the navel line.
Supplemental oxygen was indicated through a mask with an oxygen reservoir, 500 ml of warm crystalloids were administered, and blood samples for hemoglobin/hematocrit and blood typing were collected. After the evaluation and initial care, the patient showed signs of improvement with a reduction in his heart and respiratory rate to normal values.
As the patient became stable, was taken to the imaging suite to perform a CT scan to look which side of the chest was the source of the pneumothorax and subcutaneous emphysema.
Computed tomography revealed a pericardial rupture with only the right pericardial circumference intact, hernia of the heart to the left pleural space, bilateral pneumothorax, small hemothorax on the right, and a subcutaneous emphysema around the entire chest (Figures 1-2).
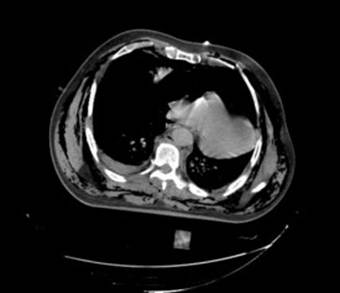
Figure 1. Right hemothorax, cardiac herniation to the left pleural space and right branch of pericardium intact.
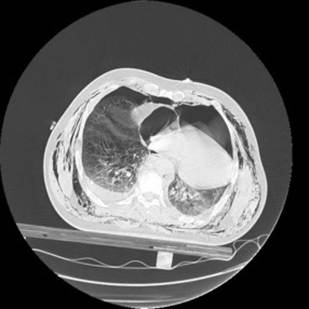
Figure 2. Bilateral pneumothorax, cardiac herniation to the left pleural space, and subcutaneous emphysema.
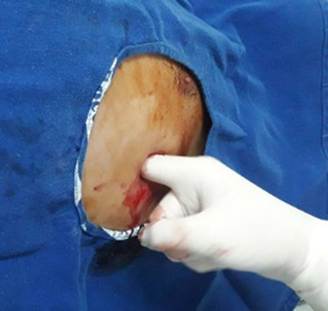
Which surgical technique should the team use to drain both pleural cavities? It was decided to perform the chest drainage by blunt dissection as it is a safer technique. During the procedure on the left side it was possible to feel the “impressions” of the coronary arteries and the right ventricle, the tube was carefully passed in the posterior and superior direction. Air outlet was observed (Figure 3). On the right side there was an outflow of air and 300 ml of bloody output.
Then the patient was transferred to the department of thoracic surgery and neurosurgey. He underwent left thoracotomy and was diagnosed with paraplegia. Recovery well after thoracic surgery.
Discussion
There are a variety of techniques to perform a chest drainage, based on the insertion method, such as the Seldinger technique and trocar insertion, which is faster, smaller incision, and there is a minimal tissue dissection resulting in less pain, as smaller drains’ caliber are used, with even better aesthetic results4.
The Seldinger technique is used by several services for draining both small liquid and gaseous collections. The main disadvantage is the inability to digitally palpate the pleural cavity and the difficulty of correctly directing the position of the chest tube5.
The trocar insertion technique is performed with a wire passed inside the chest drain, a small incision is made in the skin and the trocar/drain set is inserted towards the pleural cavity. Although several authors considered a very simple technique, we do not recommend it due to the risk of lesion of the lung and adjacent organs6,7.
Cardiac injury can happen during the thoracic drainage but is very rare and a catastrophic complication. Most of these injuries are related to anatomical distortion of the thoracic organs, as after pneumonectomy, extreme kyphoscoliosis, and cardiomegaly7,8,9.
One of these iatrogenic cardiac injuries was related to cardiomegaly and the procedure was performed using the Seldinger technique10.
In the case presented, was preferred the blunt dissection technique, as the team was facing an anatomical distortion of the heart (cardiac hernia) due to thoracic trauma, as it is the safest method and has the advantage of palpating the pleural cavity during the procedure.
Some of these patients with small or moderate traumatic pneumothorax, in the absence of other significant injuries or need for positive pressure, could be treated conservatively. This was the opposite in our patient that had cardiac herniation to the left pleural space and hemothorax in the right side11.
Thoracic drainage is a simple and the most used procedure in thoracic surgery. Blunt dissection is the oldest technique; it is considered very painful, and some authors report that 50% of patients report pain in 9 out of 10 on a scale of 10 12.
This is still the only technique that allows palpation of the pleural cavity, to assess the presence of loculations, adequate drain position, palpation of adjacent organs in situations of anatomical distortion and especially when vital organs in the chest could not be confirmed before the drain insertion with imaging methods13.
Conclusion
Learning the correct technique, the right indication, recognizing possible complications that may occur, and how to deal with these complications is essential for doctors working in urgent and emergency services. We present a case of challenging thoracic drainage in which the anatomic distortion of the heart caused by a cardiac herniation to left pleural space could be diagnosed before the insertion of the chest tube.

