










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista colombiana de Gastroenterología
versão impressa ISSN 0120-9957versão On-line ISSN 2500-7440
Rev Col Gastroenterol v.24 n.4 Bogotá dez. 2009
Cholestatic hepatitis induced by flutamida. Presentation of a case
Fernando García del Risco, MD. (1), Juan Manuel Camargo, MD. (2), Harold España Arrieta, MD.(3)
(1) Gastroenterologist. IV Associate Professor. Head of Gastroenterology Section. Medicine Department, Universidad de Cartagena (University of Cartagena), Colombia.
(2) Internist. Cartagena University. Emergency Room Internist. Hospital universitario de Cartagena (University Hospital of Cartagena) Cartagena, Colombia.
(3) Resident level III, Internal medicine, University of Cartagena. Cartagena, Colombia.
Received: 03-08-09 Accepted: 21-10-09
Abstract
Flutamide is a nonsteroidal antiandrogen, used like therapy a long term for the prostate cancer. Between the indirects effects the hepatic toxicity is included, which is very rarely reported. The case of an adult of 71 years old with prostate cancer appears that develops episode of cholestatic hepatitis during treatment with flutamide. After to suspend flutamide the patient it recovers progressively his hepatic function, but he presented a recurrence more severely upon reintroduction of the drug.
The resumption of the treatment after a first episode of toxic hepatitis is not justified and is necessary to consider the hepatic toxicity of the drug, when it is decided to indicate it like treatment.
Key words
Flutamide, hepatotoxicity, cholestatic hepatitis, prostate cancer.
Introduction
Hepatotoxicity induced by medications accounts for between 2% and 5% of cases hospitalized because of jaundice, including 40% of patients older than 50 years of age with hepatitis. Sgro et. al. found an annual incidence of 13.9% per 100,000 habitants. They also found that it is the main cause of fulminant hepatic failure. It can be the result of any one of several medications, including flutamide (1, 2).
Flutamide is a nonsteroidal antiandrogen prescribed for the treatment of advanced prostate cancer, hirsutism (3, 4) and in benign prostatic hyperplasia (4-6). The effect is developed through an active metabolite, 2-Hidroxy-flutamide. It competitively inhibits capture and/or union of androgens in target tissues, but it also inhibits liberation of gonadotropins from hypophysis (3, 7-9). After administration, it is well absorbed and circulates almost exclusively in the active form. It reaches maximum levels in 2 to 4 hours, and has an average life of 5 to 6 hours. It is metabolized in the liver and eliminated in urine (9).
Even though Flutamide is a safe and well-tolerated medication, it is not exempt from adverse effects. The most frequent (>10%) are:
- Endocrinological and metabolic diseases: galactorrhea and gynecomastia (9% -42%), erectile dysfunction, decreased libido.
- Gastrointestinal diseases: nausea, vomiting (11%-12%), diarrhea.
- Hepatic diseases: mild increases of transaminases (mostly GPT) and of lactate dehydrogenase (LDH).
In lesser proportion (1-10%):
- Cardiovascular diseases: hypertension (1%).
- Hematologic diseases: anemia (6%), leucopenia (3%), thrombocytopenia (1%).
- Neuro-muscular diseases: muscle weakness (1%).
It very seldom (< 1%) produces pneumonitis caused by hypersensitivity, pulmonary embolism, jaundice, hepatitis and hepatic failure.
Of all the above, hepatic failure is the most serious disease. Besides being rare, it is rarely reported (5). In 1992 Gómez et. al. reported 4 cases out of 1091 treated patients, whereas Prattichizzo (1994) reported one case out of 200 patients (8).
Clinical manifestations and biochemical changes in hepatic failure induced by flutamide can result in:
- Asymptomatic transminase elevation (11).
- Toxic Hepatitis with jaundice, ascites, hypoalbuminemia and Hepatic encephalopathy, which can be lethal (3, 11).
- Cholestatic hepatitis with a pronounced alkaline phosphatase elevation and GGT.
A latency period from the start of administration of medication to the appearance of a medical profile varies in length from 12 days to 52 weeks. Even though most patients completely recovery after administration of medication is stopped (within a period of weeks or months), there are cases that develop into Hepatic encephalopathy, fulminant hepatic failure (FHF) and even (5, 6, 12, 13). This is the case of a patient who presented prostate adenocarcinoma, but who also developed a secondary hepatotoxicity caused by flutamide.
Case presentation
The patient was a 71 year old male journalist, who presented jaundice. The patient had a hypertension antecedent with no precedent pharmacological treatment. In December of 2009, well-differentiated prostate cancer, Gleason grade 2, was diagnosed. On that occasion patient began treatment with goserelin (a synthetic analogue to a gonadotropin-releasing hormone - GnRH-) continuously for 6 months. It was replaced by Cyproterone acetate (a steroid anti-androgen). With this treatment the patients Serum Levels of Prostate-Specific Antigen (PSA) decreased, but without level normalization. For these reason, a non-steroid anti-androgen, Flutamide, was introduced. Thereafter, the patient continued treatment with both medications for 4 months, at which point cyproterone was discontinued.
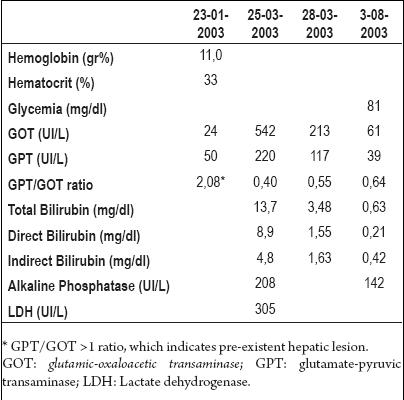
The patient was asymptomatic for his prostate condition, and consumed moderate amounts of alcohol. He took Flutamide for two years, at which point he was hospitalized for respiratory problems (March, 2003). During his hospital stay he developed jaundice and elevation of transaminases. These exams were evaluated by the gastroenterology service, who asked for viral markers and autoimmune tests (antinuclear antibodies and anti-smooth muscle antibody), the results of which were negative. Afterwards, the causal relationship between the clinical profile and flutamide was established and the medication was suspended (after approximately 730 days of treatment). With the medications suspension a gradual improvement in hepatic tests was noticed until normal levels were reached (Table 1).
Table 1. Results of Paraclinical tests during the first hospitalization.
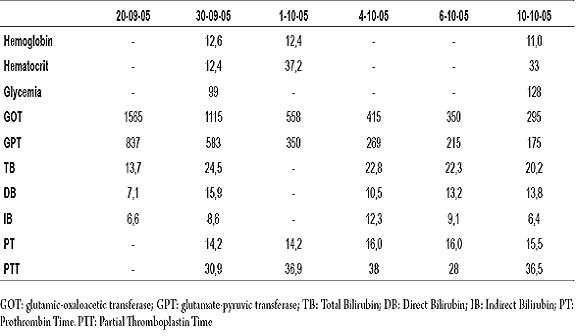
An orchiectomy, decided upon after a medical-surgical meeting, was performed for long term therapy. The patient was discharged, followed by sporadic check-ups of prostate-specific antigen, which tended to increase again. For this reason treatment with flutamide was reinitiated in 2005. Ii is important to note that some liver function tests were performed with normal results before treatment. In September, 2005, after 7 weeks of treatment, the patient presented asthenia, adynamia, jaundice and decreased appetite. He was hospitalized again and continuously monitored by the urology service. Because of the high levels shown in the liver tests which were performed, he was again sent to the gastroenterology service. A physical examination revealed generalized jaundice, vascular spiders in the superior thoracic aperture, non-abdominal pain or visceromegaly, and either the presence of palmar erythema or encephalopathy. Lab tests showed transaminases, bilirubin and prothrombin time elevation at higher levels than during the previous hospitalization (Table 2). Abdominal ultrasonography showed increased hepatic echogenicity, and an abdominal TAC revealed mild splenomegaly and small liver size. In accordance with these findings, we decided to investigate for the presence of gastric and esophageal varices. An esophageal duodenoscopy was performed and was normal. During the hospitalization, the patient received treatment with 300 mg of ursodeoxicolico acid every 8 hours, 10 mg of intravenous vitamin K every 24 hours and a low fat diet. The patient was moved to the general ward where his liver tests improved, after which he was discharged. The patient passed away a year later, in 2006, due to complications of hepatic failure.
Table 2. Results of paraclinical tests during the second hospitalization.
Discussion
Among currently available therapeutic options for long term prostate cancer treatment, bilateral orchiectomy and Diethylstilbestrol (DES) are the most commonly used methods. DES can cause secondary cardiovascular effects including thrombosis and erectile dysfunction. However, there are other alternatives with better security profiles than DES, but similar therapeutic results. These alternatives are the LHRH analogues, aminoglutemide, and steroidal and nonsteroidal antiandrogens including flutamide, bicalutamide and nilutamide (14).
Flutamide has been used for prostate cancer treatment since 1980. Since that time hepatotoxicity incidence has been reported constantly (5, 15), but in our circles there have been few cases and their prevalence still unknown. Wyowsky et. al. (1996) published two studies showing a prevalence of 3 cases per 10,000 patients per year (11, 12). Subsequently, Rosenthal (1996) found a 6% incidence, followed by Cetins findings (1999) of a 9% rate of incidence (16, 17). The problem with these studies is under reporting of cases (5).
In cases with hepatic toxicity associated with medications, diagnosis is based on the causal relationship of the treatment, the suspicious medication, and the appearance of signs of hepatotoxicity. Most of the time a clinical improvement will occur after administration of the medication is suspended. Initially, exclusion of other causes of hepatotoxicity is important for diagnosis. In our case, a causal relationship was established, because the patient had received flutamide for two years, then presented a first episode of cholestatic hepatitis, then improved after administration of the medication ceased. Renewal of administration of the medication then triggered a new more intense episode of cholestatic hepatitis that forced the patients hospitalization. Administration of medication was halted again, and the patient recovered.
Goserelin is not recognized as a hepatotoxic medicine. It was also used by our patient without other associated treatments. The patient did not present any hepatic dysfunction during the use of this medication. Hepatotoxicity cases have been reported with treatment combining and cyproterone. However, in this patient the hepatic dysfunction was presented a considerable time after the medication had already been suspended. Alcohol consumption could help explain the first episode of cholestatic hepatitis, but not the most recent episode in which there was no concomitant medication (22, 23).
Hepatotoxicity is caused by medications in several ways. One is direct toxicity in which increasing dosages induce liver lesions which can be predicted. On the other hand, idiosyncratic toxicity, in which normal dosages can produce unpredictable damage, also exists (18, 19). This type of reaction can be caused by drug hypersensitivity or by formation of hepatotoxic metabolites. This mechanism seems to correspond with flutamide reactions, considering that is not possible to demonstrate direct or hypersensitive toxicity (fever, rash or eosinophilia related to indicated doses) (20, 21).
Greater hepatic affect has been found in patients with chronic hepatitis caused by Hepatitis C and B viruses (20) and in patients whose ALT/AST (alanine aminotransferase and aspartate aminotransferase) (GPT/GOT) relation is >1 (Table 1). This suggests that flutamide could exacerbate latent or mild preexisting hepatic dysfunction. In some reported cases fatty liver disease is the cause of previous hepatocellular dysfunction; therefore it should be diagnosed or eliminated as a possibility before beginning treatment of any patient (22, 23, 24).
The severity of toxicity oscillates between subclinical states with low hypertransaminasemia levels, to serious hepatic failures. Cases of cholestatic, hepatocellular and/or mixed patterns are described. The pathology has not shown a clear and consistent pattern. Severe or diffuse necroses of hepatocytes, cholestasis and inflammation or even focal hepatic necrosis can be found (10). The unfortunate fatal outcome in the case of our patient was associated with chronic hepatopathy complications.
Conclusion
Flutamide-induced hepatotoxicity has to be considered before a patient begins treatment with this drug. For this reason a patient must be checked periodically for early disease detection. If hepatotoxicity is detected, the drug must be suspended immediately.
An evaluation every 15 days is proposed. Liver function tests should be conducted during each check-up in the first 2 months of treatment and once a month thereafter for the next four months. Under no circumstances is reinitiation of treatment with flutamide justified for a patient with a previous instance of hepatic toxicity caused by this drug.
References
1. Bloomer JR, Goodman ZD, Ishak KG. Drug-induced liver injury pathology. In: clinical and pathological correlations in liver disease: Approaching the next millennium; American Association for the Study of Liver Diseases. Postgraduate Course; 1998: 236-239.
2. Sgro C, Clinard F, Ouazir K, Chanay H, Allard C, Guilleminet C, et al. Incidence of drug-induced hepatic injuries: A French population-based study. Hepatology 2002; 36: 451-459.
3. Andrade RJ, Lucena MI, Fernández MC, Suárez F, Montero JL, Fraga E, y col. Fulminant liver failure associated with flutamide therapy for hirsutism. Lancet 1999; 353: 983.
4. Azziz, R. The evaluation and management of hirsutism. Obstet Gynecol 2003; 101: 995-998.
5. García-Cortés M, Andrade RJ, Lucena MI, Sánchez-Martínez H, Fernández MC, Ferrer T, y col. Hepatotoxicidad por flutamida: análisis retrospectivo de una serie. Rev Esp Enferm Dig 2001; 93: 424-427.
6. Lee HW, Chung JP, Lee KS, Kim KC, Lee KS, Chon CY, et al. A case of Flutamide-Induced Acute Cholestatic Hepatitis. Yonsei Med J 1996; 37(3): 225-229.
7. Caballería E, Aragó JV, Sanchís A. Hepatotoxicidad por flutamida. Med Clin (Barc) 1994; 102: 434-438.
8. Takashima E, Iguchi K, Usui S, Yamamoto H, Hirano K. Metabolite Profiles of Flutamide in Serum from Patients with Flutamide-Induced Hepatic Dysfunction. Biol Pharm Bull 2003; 26(10): 1455-1460.
9. Brodgen RN, Clissold SP. Flutamide: A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic use in advanced prostatic cancer. Drugs Aging 1991; 1: 104.
10. Gomez JL, Dupont A, Cusan L, Tremblay M, Suburu R, Lemay M, et al. Incidence of liver toxicity associated with the use of flutamide in prostate cancer patients. Am J Med 1992; 92: 465-470.
11. Wysowski DK, Fourcroy JL. Flutamide hepatotoxicity. J Urol 1996; 155: 209-214.
12. Wysowski DK, Freiman JP, Tourtelot JB, Horton ML. Fatal and nonfatal hepatotoxicity associated with flutamide. Ann Intern Med 993; 118: 860-864.
13. Fernández CM, Morano LE, Montes J, Fachal C. Fallo hepático fulminante con evolución fatal inducido por flutamida. Med Clin (Barc) 1997; 108: 237-238.
14. Robson M, Dawson N. How is androgen-dependent metastatic prostate cancer best treated? Hematol Oncol Clin North Am 1996; 10: 727-738.
15. Labrie F. Mechanism of action and pure antiandrogenic properties of flutamide. Cancer 1993; 72(supl. 12): 3816-3824.
16. Cetin M, Demirci D, Unal A, Altinbaş M, Güven M, Unlühizarci K. Frequency of flutamide induced hepatotoxicity in patients with prostate carcinoma. Hum Exp Toxicol 1999; 18: 137-140.
17. Rosenthal SA, Linstadt DE, Leibenhaut MH, Andras EJ, Brooks CP, Stickney DR, et al. Flutamide associated liver toxicity during treatment with total androgen suppression and radiation therapy for prostate cancer. Radiology 1996; 199: 451-455.
18. Knowles SR, Uetrecht J, Shear NH. Idiosyncratic drug reactions: The reactive metabolite syndromes. Lancet 2000; 356: 1587-1591.
19. Navarro VJ, Senior JR. Drug-related hepatotoxicity. N Engl J Med 2006; 354: 731-739.
20. Benichou C. Criteria of drug-induced liver disorders. Report of an international consensus meeting. J Hepatol 1990; 11: 272-274.
21. Kaplowitz N. Drug-induced liver injury. Clin Infect Dis 2004; 38(Supl 2): S44-S48.
22. Pu YS, Liu CM, Kao JH, Chen J, Lai MK. Antiandrogen hepatotoxicity in patients with chronic viral hepatitis. Eur Urol 1999; 36: 293-297.
23. Dourakis SP, Alexopoulou AA, Hadziyannis SJ. Fulminant hepatitis after flutamide treatment. J Hepatol 1994; 20 (3): 350-3.
24. Aizawa Y, Ikemoto I, Kishimoto K, Wada T, Yamazaki H, Ohishi Y, Kiyota H, et al. Flutamide-induced hepatic dysfunction in relation to steady-state plasma concentrations of flutamide and its metabolites. Mol Cell Biochem 2003; 252(1-2): 149-156.
1. Bloomer JR, Goodman ZD, Ishak KG. Drug-induced liver injury pathology. In: clinical and pathological correlations in liver disease: Approaching the next millennium; American Association for the Study of Liver Diseases. Postgraduate Course; 1998: 236-239. [ Links ]
2. Sgro C, Clinard F, Ouazir K, Chanay H, Allard C, Guilleminet C, et al. Incidence of drug-induced hepatic injuries: A French population-based study. Hepatology 2002; 36: 451-459. [ Links ]
3. Andrade RJ, Lucena MI, Fernández MC, Suárez F, Montero JL, Fraga E, y col. Fulminant liver failure associated with flutamide therapy for hirsutism. Lancet 1999; 353: 983. [ Links ]
4. Azziz, R. The evaluation and management of hirsutism. Obstet Gynecol 2003; 101: 995-998. [ Links ]
5. García-Cortés M, Andrade RJ, Lucena MI, Sánchez-Martínez H, Fernández MC, Ferrer T, y col. Hepatotoxicidad por flutamida: análisis retrospectivo de una serie. Rev Esp Enferm Dig 2001; 93: 424-427. [ Links ]
6. Lee HW, Chung JP, Lee KS, Kim KC, Lee KS, Chon CY, et al. A case of Flutamide-Induced Acute Cholestatic Hepatitis. Yonsei Med J 1996; 37(3): 225-229. [ Links ]
7. Caballería E, Aragó JV, Sanchís A. Hepatotoxicidad por flutamida. Med Clin (Barc) 1994; 102: 434-438. [ Links ]
8. Takashima E, Iguchi K, Usui S, Yamamoto H, Hirano K. Metabolite Profiles of Flutamide in Serum from Patients with Flutamide-Induced Hepatic Dysfunction. Biol Pharm Bull 2003; 26(10): 1455-1460. [ Links ]
9. Brodgen RN, Clissold SP. Flutamide: A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic use in advanced prostatic cancer. Drugs Aging 1991; 1: 104. [ Links ]
10. Gomez JL, Dupont A, Cusan L, Tremblay M, Suburu R, Lemay M, et al. Incidence of liver toxicity associated with the use of flutamide in prostate cancer patients. Am J Med 1992; 92: 465-470. [ Links ]
11. Wysowski DK, Fourcroy JL. Flutamide hepatotoxicity. J Urol 1996; 155: 209-214. [ Links ]
12. Wysowski DK, Freiman JP, Tourtelot JB, Horton ML. Fatal and nonfatal hepatotoxicity associated with flutamide. Ann Intern Med 993; 118: 860-864. [ Links ]
13. Fernández CM, Morano LE, Montes J, Fachal C. Fallo hepático fulminante con evolución fatal inducido por flutamida. Med Clin (Barc) 1997; 108: 237-238. [ Links ]
14. Robson M, Dawson N. How is androgen-dependent metastatic prostate cancer best treated? Hematol Oncol Clin North Am 1996; 10: 727-738. [ Links ]
15. Labrie F. Mechanism of action and pure antiandrogenic properties of flutamide. Cancer 1993; 72(supl. 12): 3816-3824. [ Links ]
16. Cetin M, Demirci D, Unal A, Altinbas M, Güven M, Unlühizarci K. Frequency of flutamide induced hepatotoxicity in patients with prostate carcinoma. Hum Exp Toxicol 1999; 18: 137-140. [ Links ]
17. Rosenthal SA, Linstadt DE, Leibenhaut MH, Andras EJ, Brooks CP, Stickney DR, et al. Flutamide associated liver toxicity during treatment with total androgen suppression and radiation therapy for prostate cancer. Radiology 1996; 199: 451-455. [ Links ]
18. Knowles SR, Uetrecht J, Shear NH. Idiosyncratic drug reactions: The reactive metabolite syndromes. Lancet 2000; 356: 1587-1591. [ Links ]
19. Navarro VJ, Senior JR. Drug-related hepatotoxicity. N Engl J Med 2006; 354: 731-739. [ Links ]
20. Benichou C. Criteria of drug-induced liver disorders. Report of an international consensus meeting. J Hepatol 1990; 11: 272-274. [ Links ]
21. Kaplowitz N. Drug-induced liver injury. Clin Infect Dis 2004; 38(Supl 2): S44-S48. [ Links ]
22. Pu YS, Liu CM, Kao JH, Chen J, Lai MK. Antiandrogen hepatotoxicity in patients with chronic viral hepatitis. Eur Urol 1999; 36: 293-297. [ Links ]
23. Dourakis SP, Alexopoulou AA, Hadziyannis SJ. Fulminant hepatitis after flutamide treatment. J Hepatol 1994; 20 (3): 350-3. [ Links ]
24. Aizawa Y, Ikemoto I, Kishimoto K, Wada T, Yamazaki H, Ohishi Y, Kiyota H, et al. Flutamide-induced hepatic dysfunction in relation to steady-state plasma concentrations of flutamide and its metabolites. Mol Cell Biochem 2003; 252(1-2): 149-156. [ Links ]

