










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista colombiana de Gastroenterología
versão impressa ISSN 0120-9957
Rev Col Gastroenterol vol.33 no.4 Bogotá out./dez. 2018
https://doi.org/10.22516/25007440.205
Case report
A case of a neuroendocrine tumor of the ileocecal valve with a single hepatic metastasis
1Hospital Provincial Docente ¨Manuel Ascunce Domenech¨ Camagüey. Cuba
Neuroendocrine tumors of the gastrointestinal tract are very rare tumors that most frequently occur in the small intestine, primarily in the ileum. They secrete bioactive peptides and amines. The World Health Organization (WHO) classifies them into five grades according to the degree of differentiation and biological behavior. Clinical manifestations may be absent or nonspecific. We report the case of a 49-year-old patient who was admitted due to abdominal pain in the right hemiabdomen, accompanied by aerogastria, vomiting and constitutional syndrome. A painful hepatomegaly with a single nodule of approximately 2.5 cm was found during physical examination. CAFF and laparoscopy with biopsy diagnosed a single hepatic metastasis of a neuroendocrine tumor of gastrointestinal origin. This was confirmed by colonoscopy with ileoscopy which found a subepithelial tumor in the ileocecal valve. Immunohistochemistry helped confirm the diagnosis. Treatment for this type of tumor can be surgical, but this patient rejected surgery. It was treated with chemotherapy and radiation therapy. Early diagnosis of this entity is fundamental but is rare because of the infrequency of the disease.
Keywords: Neuroendocrine tumor; classification; diagnosis; colonoscopy
Los tumores neuroendocrinos (TNE) del tracto gastrointestinal son muy infrecuentes, el intestino delgado y principalmente el íleon son los sitios donde ocurren con mayor frecuencia. Tienen la capacidad de secretar péptidos y aminas bioactivas. La Organización Mundial de la Salud (OMS) los clasifica de acuerdo con el grado de diferenciación y conducta biológica en 5 grados. Las manifestaciones clínicas pueden estar ausentes o ser inespecíficas. Se reporta el caso de un paciente de 49 años de edad quien fue ingresado por dolor abdominal en hemiabdomen derecho, acompañado de aerogastria, vómitos y síndrome constitucional; en el examen físico se encontró hepatomegalia dolorosa con nódulo único de 2,5 cm aproximadamente. La citología por aspiración con aguja fina (CAFF) y la laparoscopia con biopsia diagnosticaron una metástasis hepática única de un TNE de origen gastrointestinal, que se confirmó con la colonoscopia con ileoscopia encontrando un tumor subepitelial en la válvula ileocecal. La inmunohistoquímica realizada ayudó a la confirmación del diagnóstico. El tratamiento puede ser quirúrgico; sin embargo, este paciente rechazó esta terapia, por lo que se trató con quimioterapia y radioterapia. Lo fundamental en esta entidad es el diagnóstico precoz, que pocas veces se realiza por lo infrecuente de la enfermedad.
Palabras clave: Tumor neuroendocrino; clasificación; diagnóstico; colonoscopia
Introduction
Neuroendocrine tumors (NETs) of the gastrointestinal system are very aggressive heterogeneous clinical-pathological entities that account for less than 5% of all neoplasms of the digestive system. 1 Their incidence varies from 2.5 to 5 cases/100,000 people. 1,2 Because they are derived from neuroendocrine cells of the gastrointestinal tract, NETs have neurosecretory capacity (the ability to secrete bioactive peptides and amines). Their most important secretion is serotonin (5-hydroxytryptamine, 5-HT). 2 NETs are most frequently located in the gastrointestinal tract (74%), especially the ileum in the small intestine where 30% are reported to be located. This was the location in the case presented here. Nevertheless, they can also be found in the bronchopulmonary system (25%). 3 The remaining 1% occur in the larynx, gallbladder, extrahepatic bile ducts, liver, spleen and male and female genitalia. 4 NETs are named according to the hormone they release only if it is released in measurable quantities and is functionally active. Otherwise they are called neuroendocrine tumors. 1,3 The objective of this study is to present the case of a patient with a NET of the ileocecal valve which is very rare in our environment.
Clinical case
The patient was a 49 year old white male who works as a carpenter. He had smoked a pack of cigarettes daily for 20 years and was chronically alcoholic having drunk 1/2 liter of rum daily for 15 years. He had no family history of interest. He reported diffuse abdominal pain throughout the abdomen, especially in the right hemiabdomen, for approximately six months prior to diagnosis. This pain started in the right hypochondrium and had increased until it became sharp. As the pain intensified, it began to be accompanied by nausea to the point that the patient was vomiting three times a day and had aerogastria and abdominal distension. He had been treated by a doctor without improvement. Rather he had developed additional symptoms of constipation, asthenia, anorexia and a loss of 10 kg. He consulted another specialist who decided to refer him to our clinic.
Physical Examination
Physical examination revealed impairment of the patient’s general state. He had moist and normal-colored mucous membranes without adenopathies in peripheral lymph node chains and without or edema or jaundice. His cardiorespiratory examination was normal with blood pressure (BP) 130/80 mm Hg. His central heart rate was 84 beats per minute (bpm).
He had diffuse abdominal pain in the right hemiabdomen with hepatomegaly that exceeded the costal margin by 2 cm, and a painful, fixed and rounded mass of approximately 2 cm was felt. An indurated and slightly painful area was detected near the right iliac fossa. No other alterations were found. The rest of the physical examination was normal, including the urological sphere and the fundus of the eye.
Analytical studies of ions and enzymes and of renal, hepatic and pancreatic functioning showed no significant alterations except for a globular sedimentation rate of 80 mm/1 h (The normal value is 20 or less.) and a lactate dehydrogenase level of 850 IU/L (The normal value is between 130 and 300). A chest x-ray and the electrocardiogram were normal, and abdominal ultrasound showed a single nodule of 2.5 cm in the liver but no other alterations.
A fine needle aspiration (FNA) biopsy contained low-grade epithelial tumor type adenocarcinoma of possible endocrine origin. A laparoscopic thick trocar biopsy reported the same characteristics as the FNA biopsy (Figures 1 and 2). Computed tomography (CT) of the abdomen, retroperitoneum, thorax and mediastinum showed no abnormalities.
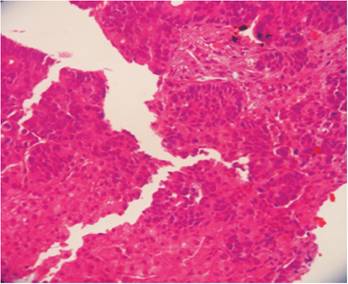
Figure 1 Microphotograph of a liver biopsy showing diffuse metastatic infiltration by malignant cellular nests. H/E-20 X.

A barium enema showed the complete lesion in the terminal ileum.
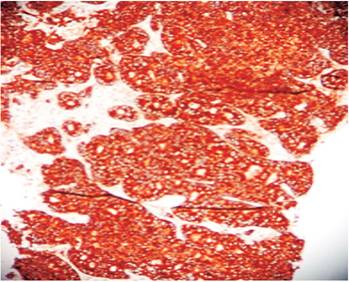
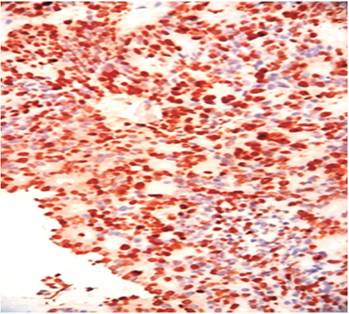
Colonoscopy revealed a rounded 4 cm tumor-like lesion of the same color as the surrounding mucosa at the ileocecal valve. The sign of the tent, elevation of the intestinal wall with a broad base and a blunt apex, could be seen without a pedicle and with the mucosa intact (Figures 3 and 4). A biopsy taken for histological study contained poorly differentiated neuroendocrine carcinoma grade III. Immunohistochemistry was positive for neuron specific enolase (NSE), synaptophysin and Ki 67 (Figures 5, 6 and 7).
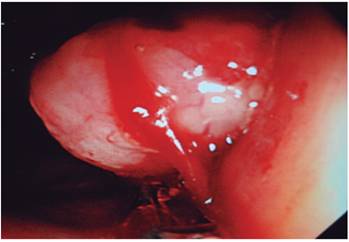

Figure 4 Macrophotography of the terminal ileum. Note the rounded dark yellow tumor at 1.5 cm from the ileocecal valve.
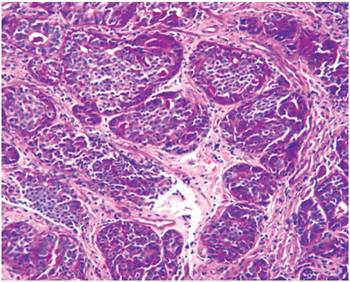
Figure 5 Microphotograph of the intestinal lesion showing well-defined nests of malignant tumor cells with neuroendocrine histological features. H/E-20 X.
The patient was moved to the Madame Curie Oncological Hospital in the city of Camagüey, where he began treatment with chemotherapy and radiation therapy.
Discussion
Why tumors of the small intestine occur so infrequently is unclear, but it has been proposed that their high liquid content causes less irritation of the mucosa and less exposure to carcinogens. It has also been suggested that increased secretion of immunoglobulin A (IgA) is a protective factor. 5 NETs originate in the gastrointestinal endocrine system and are related to NETs of the thyroid, pancreas and pheochromocytomas as well as to multiple endocrine neoplasms (MEN) in 9% of cases. 2 The gastrointestinal tract has the largest number of neuroendocrine cells in the body. These cells produce peptides and amines that regulate motility and digestion. 5 Only some cause neoplastic proliferation which occurs least frequently in the submucosa of the terminal ileum although this was the case in the patient we have presented. 1,4
NETs are named according to the hormones they produce. The classification of NETs proposed by Capella and adopted by the WHO is based on the site of origin, size of the tumor, extension in the surrounding tissue, angioinvasion, biological behavior and histological differentiation in combination with whether its status is functioning or non-functioning.1,2 This patient was at grade III of this classification. The peak period of appearance is between the sixth and seventh decades of life. Ten percent of these tumors secrete bioactive mediators which produces symptoms typical of carcinoid syndrome, but patients usually are diagnosed following abdominal pain or intestinal obstruction. Nevertheless, preoperative diagnosis is usually difficult due to the insidious evolution of symptoms. 6 These tumors can remain asymptomatic for years until after the onset of metastasis but can also have obstructive symptoms which are found incidentally during surgery or radiological study. 5
Diagnosis of this entity should include 5-HT determinations in 24-hour urine for serotonin-producing carcinoids. This was not possible in the case of our patient due to difficulties with the study. CT scans and MRI have similar diagnostic success with regional and distant metastases (77% and 80%, respectively). 7 For this patient, a CT scan with double contrast was very effective; and digestive endoscopy, intestinal transit and abdominal ultrasound were equally useful. To improve the diagnosis of this entity, a series of immunohistochemistry markers are used including neuron specific enolase (NSE) and markers associated with small vesicles (synaptophysin). There is an almost linear relationship between the size and the presence of metastasis, 85% of tumors of more than 2 cm metastasize. 5 This was clearly shown in our patient.
Treatment for NETs varies from medical treatment with chemotherapy and radiation therapy, to surgical treatment with tumor resection. Choice of treatment depends on the location, the stage and the symptoms. In patients with metastases, resection of the primary tumor together with mesenteric nodules has resulted in notable improvement of symptoms. 8 Chemotherapy and radiation therapy have been shown to have little utility for treatment of these tumors. 4 The prognoses of NETs of the small intestine are less favorable than for gastric and rectal NETs. 8 The ten-year survival rate ranges from 65% to 73% for well-differentiated tumors and from 46% to 71% for localized and distant disease. 2,3
Conclusions
NETs of the gastrointestinal system are very infrequently occurring entities. These tumors have heterogeneous clinical manifestations and may remain asymptomatic for years. Differential diagnosis includes many causes of abdominal pain. The time between the onset of symptoms and diagnosis is 6 to 7 months, and digestive endoscopy ultrasound and double contrasted CT are key diagnostic tools. Therapy varies from medical treatment to surgical treatment, depending on the location, stage and symptoms.
Referencias
1. Alvarado Camello I. Tumores neuroendocrinos del aparato gastrointestinal y páncreas. Patología Rev latinoamericana. 2009;47(3):213-9. [ Links ]
2. Lawrence B, Gustafsson BI, Chan A, Svejda B, Kidd M, Modlin IM. The epidemiology of gastroenteropancreatic neuroendocrine tumors. Endocrinol Metab Clin North Am. 2011;40(1):1-18, vii. doi: 10.1016/j.ecl.2010.12.005. [ Links ]
3. Reynolds I, Healy P, Mcnamara DA. Malignant tumours of the small intestine. Surgeon. 2014;12(5):263-70. doi: 10.1016/j.surge.2014.02.003. [ Links ]
4. Pasieka JL. Carcinoid tumors. Surg Clin North Am. 2009;89(5):1123-37. doi: 10.1016/j.suc.2009.06.008. [ Links ]
5. Zúñiga D. Tumores neuroendocrinos gastrointestinales. Medicina legal de Costa Rica. 2013;30(1):89-98. [ Links ]
6. Gornas J, Varas M. Diagnóstico definitivo de los tumores neuroendocrinos mediante PAFF ecodirigidas por ultrasonido endoscópico. Rev Esp Enf Diag. 2011;103(3):123-8. [ Links ]
7. Mocellin S, Nitti D. Gastrointestinal carcinoid: epidemiological and survival evidence from a large population-based study (n = 25 531). Ann Oncol. 2013;24(12):3040-4. doi: 10.1093/annonc/mdt377. [ Links ]
8. Coan KE, Gray RJ, Schlinkert RT, Pockaj BA, Wasif N. Metastatic carcinoid tumors--are we making the cut? Am J Surg. 2013;205(6):642-6. doi: 10.1016/j.amjsurg.2012.05.036. [ Links ]
Received: February 05, 2018; Accepted: April 03, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
