










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista colombiana de Gastroenterología
versão impressa ISSN 0120-9957versão On-line ISSN 2500-7440
Rev. colomb. Gastroenterol. vol.35 no.4 Bogotá out./dez. 2020 Epub 12-Jul-2021
https://doi.org/10.22516/25007440.461
Letter to the editor
Bronchoesofageal Fistula Secondary to Pulmonary Aspergillosis

1Servicio de Aparato Digestivo. Hospital Universitario Clínico San Cecilio. Granada, España.
2Servicio de Aparato Digestivo. Hospital Universitario Virgen de las Nieves. Granada, España.
Dear Editor:
A 61-year-old man was admitted to our center due to a 2-week history of dyspnea and dysphagia for solids and liquids. He had mucocutaneous pallor on examination and lab test results only showed slight anemia (hemoglobin [Hb]: 12.5 g/dL). Two months earlier, he had been diagnosed with acute myeloid leukemia and treatment with idarubicin had been started.
An upper gastrointestinal (GI) endoscopy was performed, finding a 0.8 cm whitish-to-yellow and whitish esophageal lesion was observed at about 29 centimeters from the dental arch. It did not seem to originate in the esophageal mucosa as it moved independently (Figure 1), suggesting the presence of an esophageal fistula. A computed tomography (CT) scan was performed, confirming the diagnosis of bronchoesophageal fistula associated with mediastinal mass (Figure 2). A subsequent bronchoscopy showed an obliterative and necrotic endobronchial mass with malignant pseudomembranes.

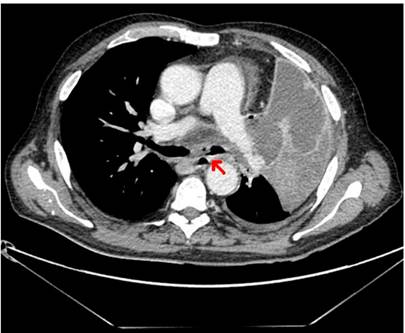
Figure 2 CT scan showing communication between the esophagus and the bronchus associated with a mediastinal mass.
A bronchoalveolar lavage (BAL) and biopsies were performed. The mass was surgically removed. During the intervention, a new upper GI endoscopy was carried out and the fistula was successfully closed using an over-the-scope clip (Ovesco®) (Figure 3). Pathology results reported necrotic tissue and granulation, as well as large colonies of Aspergillus hyphae, with no malignant cells. Bronchoalveolar lavage galactomannan was positive (I > 4). Unfortunately, the patient died two days after the surgical procedure.

Aspergillosis is a rare finding in contexts such as immunosuppression, chemotherapy for blood disorders or transplanted patients1. Fistula formation is a rare complication of pulmonary aspergillosis2, and bronchopleural fistulas are the most frequently described. In the last decade, Ovesco clip has been used during endoscopic procedures for gastrointestinal bleeding, fistulas, or perforations, with a clinical success rate between 64% and 91.7%3-5. Chronic fistulas or previous radiation therapy are common in cases where treatment failed. The risks of using this system (bleeding, perforation, or aspiration) are rare when it is used correctly. Cases of tracheoesophageal fistulas successfully treated with Ovesco have been reported, although that is not the case for bronchoesophageal fistulas. The latter is an exceptional and underreported finding, which, in this case, was resolved using an Ovesco clip. However, in the clinical context of this patient, it was not enough because there was no opportunity to start a specific antifungal treatment.
REFERENCES
1. Yu Y, Zhu C, Qian X, Gao Y. Tracheoesophageal fistula induced by invasive pulmonary aspergillosis. Annals of Translational Medicine. 2016;4(18):345. https://doi.org/10.21037/atm.2016.09.16 [ Links ]
2. Mineur P, Ferrant A, Wallon J, Otte JB, Michaux JL. Bronchoesophageal fistula caused by pulmonary aspergillosis. Eur J Respir Dis. 1985;66(5):360-6. [ Links ]
3. Goenka MK, Rai VK, Goenka U, Tiwary IK. Endoscopic Management of Gastrointestinal Leaks and Bleeding with the Over-the-Scope Clip: A Prospective Study. Clin Endosc. 2017;50(1):58-63. https://doi.org/10.5946/ce.2016.028 [ Links ]
4. Morrell DJ, Winder JS, Johri A, Docimo S, Juza RM, Witte SR, Alli VV, Pauli EM. Over-the-scope clip management of non-acute, full-thickness gastrointestinal defects. Surg Endosc. 2020;34(6):2690-2702. https://doi.org/10.1007/s00464-019-07030-3 [ Links ]
5. Mosquera-Klinger G, Torres-Rincón R, Jaime-Carvajal J. Endoscopic closure of gastrointestinal perforations and fistulas using the Ovesco Over-The-Scope Clip system at a tertiary care hospital center. Rev Gastroenterol Mex. 2019;84(2):263-266. https://doi.org/10.1016/j.rgmx.2018.10.004 [ Links ]
Citation: Caballero-Mateos AM, López de Hierro-Ruiz M, Redondo-Cerezo E. Bronchoesofageal Fistula Secondary to Pulmonary Aspergillosis. Rev Colomb Gastroenterol. 2020;35(4):558-559. https://doi.org/10.22516/25007440.461
Received: December 12, 2019; Accepted: December 14, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
