











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
Gestational diabetes mellitus (GDM) has been usually defined as “carbohydrate intolerance that is discovered or manifests for the first time during gestation”1. In Colombia, the reported prevalence of GDM ranges between 1.43%2 and 6.3%3; at present, international publications estimate a prevalence between 10.3%4 and 15%5, 5% corresponding to type II diabetes, 7.5% type I who become pregnant, and the remaining 87.5% are true gestational diabetes cases6. Recently, emphasis has been placed on the difference between a diagnosis of diabetes mellitus (DM) before pregnancy, diagnosed early in pregnancy, or overt diabetes, in relation to DM of gestational onset, stating that the former presents with higher glucose values, resulting in a greater probability of complications and pharmacological management7. In fact, the American Diabetes Association (ADA) currently defines GDM or diabetes of gestational onset as “Diabetes diagnosed during the second or third trimester that is not clearly overt diabetes”8.
Diabetes of gestational onset is more common in obese women, with a personal or family history of diabetes, or with a history of foetal demise or macrosomic neonates9,10. Moreover, pregnant women with GDM are more frequently affected by maternal complications such as preeclampsia, present in 10% to 25% of GDM cases11-14. Also, the frequency of cesarean section is higher in diabetic women, mainly due to foetal macrosomia15,16 which is, in turn, the most important perinatal complication in GDM. Foetal macrosomia is defined as “birthweight greater than 4,000 g”16, although some authors establish a mínimum threshold of 4,500 g17.
In Colombia, the diagnosis of GDM according to the Clinical Practice Guidelines for the prevention, early detection and treatment of abnormalities during pregnancy, delivery or puerperium, published by the Ministry of Health and Social Protection in 201318, and the Clinical Practice Guidelines for the diagnosis, treatment and follow-up of gestational diabetes published in 201619, recommend giving all pregnant women an oral glucose tolerance test (OGTT) with 75 g of glucose between 24 and 28 weeks of pregnancy, using the following diagnostic thresholds: fasting ≥ 92 mg/dl, 1 hour after challenge ≥ 180 mg/dl, and 2 hours after challenge ≥ 153 mg/dl. This is in accordance with the recommendations of the International Association of Diabetes and Pregnancy Study Groups (IADPSG)20, which modified the traditional “two-step” diagnostic system based on a screening test at 24-28 weeks with a challenge of 50 g of glucose and a normal threshold of < 140 mg/dl 1 hour after the challenge (O’Sullivan test), giving pregnant women with abnormal results another challenge with 100 g of glucose and, if the two values are abnormal, the diagnosis is confirmed21.
Bearing in mind that if the diagnosis is made early in gestation it is considered as overt diabetes and not GDM22-24, and considering also that several studies confirm the benefits of early intervention in DM during pregnancy using dietary measures and exercise in order to reduce adverse outcomes15,25, it has been of interest to search for early diagnostic and prognostic factors of DM during pregnancy, such as fasting blood sugar in early gestation26, and measurement HbA1c levels27.
HbA1c measurement has been used as follow-up test for DM control28; however, it was approved in 2010 for DM diagnosis when the level is ≥ 6.5%, as long as a diagnostic test certified by the National Glycohaemoglobin Standardisation Program (NGSP), standardised with the Diabetes Control and Complications Trial (DCCT) reference is used29. HbA1c is not altered with dietary changes, does not require fasting and has little variation between tests30; it may appear falsely elevated in the presence of salicylates, diuretics hypertriglyceridaemia, polycythaemia and splenectomy, and falsely low after transfusion, haemodialysis, haemolytic anaemia, and use of vitamins C and E31,32.
In Colombia, although the potential role of early markers has been studied33 together with risk factors3,10 and the prevalence of GDM(2,3), research has been conducted in populations subjected to traditional diagnostic tests and not to the use of the new thresholds suggested in the national guidelines or the use of HbA1c; and it has not focused on the identification of individuals with full-blown diabetes or who really present with GDM. The use of the new diagnostic criteria for GDM in pregnant women needs to focus on several aspects: the local frequency of full-blown diabetes or onset of diabetes during the second or the third trimester of pregnancy, the measurement of adverse maternal and perinatal outcomes of pregnancy in each category34, and the financial implications for the health system35.
The objective of this study is to approach the prevalence of GDM and its complications, as well as the prevalence of overt DM in the first trimester of pregnancy.
MATERIALS AND METHODS
Design and population. Prospective cohort study in pregnant women 14 years or older who came to consultation before 14 weeks of gestation and agreed to participate in the study and who had initiated prenatal care between February 2015 and July 2016 in a level I healthcare centre of the Redsalud public health network that provides care to the subsidised population in the city of Armenia, capital of the department of Quindío in central Colombia. Excluded were all women with hypertension, know diabetes or diabetes confirmed at entry by HbA1C > 6.5%, use of medications (salicylates, vitamin E and C), or medical conditions (anaemia, haemoglobinopathies, splenectomy, renal failure) that could affect HbA1c results. Consecutive sampling. A simple size of 249 patients was estimated based on a total population of 1,600 pregnant women seen per year: miscarriages 10%: subtotal 1,440; 40% recruited before 14 weeks: N = 576. Estimated prevalence of gestational diabetes, 6%; 95% confidence level for three age groups and a 10% loss.
Procedure. A licensed practical nurse with prior experience in patient recruitment, completion of forms, and trained in the estimation of gestational age at the time of entry and verification of inclusión and exclusion criteria, recruited the candidates on their arrival at the laboratory of the healthcare Prevalence of gestational diabetes mellitus based on glucose tolerance test on weeks 24 to 28. provider institution. Women who met the selection criteria and agreed to participate in the study were explained the objectives of the project and were asked to fill the informed consent. Laboratory samples were then taken, and sociodemographic and clinical information was documented. The date of the last menstruation and the results of first-trimester ultrasound scans were considered for gestational age estimation. Blood sugar and HbA1c on entry to the study were determined using blood samples for fasting blood sugar and HbA1c in separate tubes. The samples were processed immediately, the glucose test in the institution’s internal laboratory and the HbA1c in a reference laboratory: D-10-TM Haemoglobin A1c Program (Bio-Rad Laboratories), which ensures compliance with international standards (certified by NGSP as a DCCT traceable test). The results were returned daily to the healthcare centre, emphasising abnormal results; a second sample was taken when the HbA1c was ≥ 6.5%, and the persistence of this value was considered abnormal, leading to the exclusion of the patients from the study. An oral glucose tolerance test (OGTT) with 75 g was performed on weeks 24-28, using three samples: fasting, 1 and 2 hours after the glucose challenge, with the following diagnostic thresholds: fasting 92 mg/dl, 180 mg/dl after 1 hour and 153 mg/dl after 2 hours. One abnormal value confirmed the diagnosis of GDM. Laboratory test results and physical findings were documented in the clinical record and in a special form designed by the researchers. Patients were followed through to the end of pregnancy and, when required, patients were contacted by pone to obtain or confirm information. The researchers did not participate in the final care process.
Measured variables. Age, baseline BMI, maternal weight gain, neonatal birthweight, preeclampsia, primary cesarean section (non-iterative), macrosomia (newborn weight ≥ 4.000 g). Full-blown diabetes was considered to exist with a confirmed baseline result of HbA1c ≥ 6.5%, or fasting blood sugar ≥ 126 mg/dl. The following were considered adverse pregnancy outcomes: preeclampsia, primary cesarean section and macrosomia.
Analysis. Data were analysed using the SPSS 19.0 software. A descriptive univariate analysis was performed, estimating relative frequencies; the prevalence of gestational diabetes in patients with abnormal glucose tolerance test after 24 weeks was estimated using the total number of participants who were tested as the denominator. Normality was determined for quantitative variables using the Kolmogorov-Smirnov test, and central trend and scatter were calculated for continuous variables, based on the distribution found.
Bioethical considerations. The study was approved by the Bioethics Committee of the Health Sciences School of Quindío University, a pre-requisite for the approval of all forms of research in the University. Participants were asked for their informed consent and data confidentiality was guaranteed. Patients with abnormal results in diagnostic tests at the start of the study or on weeks 24-28 (blood sugar, HbA1c, GTT) were included in the institution’s protocol for the management of high-risk pregnancies and were managed by specialised medical and nutrition staff.
RESULTS
Out of a total of 372 candidates to enter the study, there were two cases (0.5%) of pre-gestational diabetes mellitus, with HbA1c greater than 6.5% measured in the first sample and confirmed in the second sample (9.5% and 9.8%, respectively); moreover, the two patients had a fasting blood sugar > 126 mg/dl. Of the 370 patients who met the selection criteria, 43 (11.6%) miscarried and another 36 (9.7%) dropped out before 24 weeks; of the remaining 291, 35 pregnant women (12%) did not undergo the OGTT. Therefore, a total of 256 patients were tested with OGTT and HbA1c. Overall, 370 pregnant women entered the study. The mean age was 22.9 years (SD ± 6.1), and the majority of the women were housewives affiliated to the subsidised healthcare regime, with ages ranging between 18 and 35 years. The mean BMI at entry was 24.2 (SD ± 6.1), 35.3% had a BMI ≥ 25 (Table 1).
Table 1 Distribution according to history and first trimester findings in pregnant women assessed for gestational diabetes mellitus in Armenia, Colombia, 2015-2016
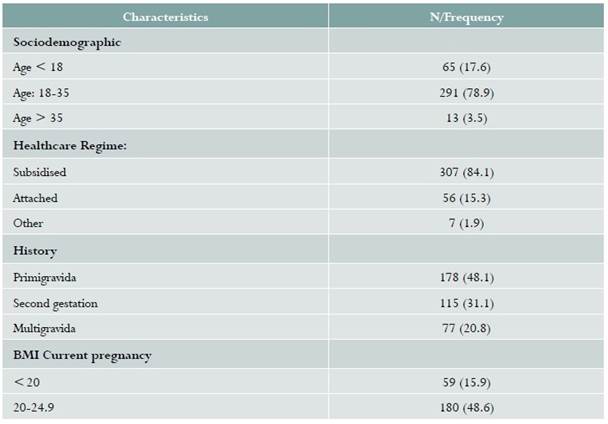
Source: study data.
Blood sugar, HbA1c and OGTT results. The average baseline blood sugar level was 82.3 mg/dl (SD ± 7.8). Baseline blood sugar was ≥ 92 mg/dl in 11.6% of the women and, of them, only one had an abnormal OGTT performed at 24-48 weeks. Noticeably higher HbA1c figures were observed in the group of patients with a baseline blood sugar ≥ 92 mg/dl (5.7 vs. 5.2). The average HbA1c was 5.1% (SD ± 0.4). Of the 256 women in whom was performed at 24 to 28 weeks, 12 had some abnormal result, for a prevalence of GDM of 4.7% (12/256).
Maternal and neonatal outcomes. Follow-up was completed until the time of delivery in 283 patients. The incidence of preeclampsia in the group of women studied was 2.1%; there were no cases of preeclampsia or foetal macrosomia among the women with GDM; 21.9% required cesarean section, while in the group with GDM, cesarean section was performed in 33.3% of cases; neonatal macrosomia was found in 3.5%, and the incidence of hyaline membrane was 0.7%, with no cases in the GDM group. The most frequent causes of cesarean section were dystocia and cephalopelvic disproportion.
DISCUSSION
In this study, the prevalence of GDM was 4.7% (12 out of 256). Based on the result of the OGTT with 75 g at 24 to 28 weeks, two cases of overt diabetes were found in the first trimester (excluded from the study) in patients who were unaware of their diabetic condition and whose history had not given rise to suspicion. Therefore, the prevalence of overt diabetes was 0.5% in accordance with the recommendation of the World Health Organisation (WHO) of investigating the possibility of DM in the first trimester7. The incidence of preeclampsia, macrosomic foetus and hyaline membrane was 2.1%, 3.5% and 0.7%, respectively.
The average fasting blood sugar levels in the first trimester (82.3 mg/dl) were found to be slightly higher than reported in the literature34,36.Although recent studies focus on the usefulness of HbA1c for the diagnosis of GDM27,37,38, in this study there were only two cases with an HbA1c ≥ 6.5%.
Historically, the diagnosis of GDM has been controversial39. The prevalence of GDM diagnosis has increased with the generalised application of the IADPSG criteria40. In a review of the literature, Brown et al. report a prevalence of GDM ranging between 3.5% and 45.3%, which is lower than the range between 9.3% and 25.5% reported by Sacks et al.41 in a retrospective analysis of the HAPO study (Hyperglycaemia and Adverse Pregnancy Outcome), Duran et al.42 report a prevalence of GDM of 35.5%, but in their study the mean age of the patients was notoriously higher than in ours (33 vs. 22.9), and the hispanic population included (34.4%) was smaller than the caucasian population (62%). On the other hand, the study by Mayo et al.4, which reports an increase in the prevalence of GDM from 3.2 to 10.3% with the use of new diagnostic thresholds, is a retrospective study of a population tested with the traditional “two-step” approach and not with the 75 g glucose test. Differences with the results of our studies might be attributed to potential underestimation due to losses to follow-up or because they are related to intrinsic factors of our population which were not investigated. The limitation of our study in terms of comparison with prior studies conducted in Colombia is that GDM prevalence studies published in the past two decades used as a basis the two-step system suggested by the ADA21.
Regarding maternal complications, our data are similar to those reported by Hirst in Vietnam in a population of 386 women with a BMI of 21.1% diagnosed with GDM using the IADPSG criteria, where the frequency of preeclampsia, large foetus for gestational age and admission to the ICU was 2.1%, 16% and 4%, respectively43. These figures are lower than those reported by Crowther et al. in 510 women with GDM diagnosed on the basis of a single measurement on weeks 24-48, with no treatment, where the incidence of preeclampsia, foetal macrosomia and neonatal respiratory distress syndrome was 19%, 21%, and 4%, respectively; this was a study conducted in an Australian population with a mean BMI of 2644.
Regarding weaknesses of our study, the small sample size resulted in a small population of women with GDM, affecting our ability to assess the frequency of complications related to this condition. On the other hand, losses to follow-up (33%) might result in an underestimation of the prevalence of GDM and its complications. These were related to the presence of miscarriage (11.6%), found to be present in a similar range as that reported in international publications45,46. Another cause of loss to follow-up was the fact that 36 patients (9.67%) dropped out from the study when they were transferred from the state-subsidised regime to the contributive regime resulting in a change of healthcare provider, and a 12.3% of patients who did not come for the OGTT between weeks 24 and 48. Another weakness was the inability to know whether the patients were assessed and followed by the nutritionist, given that this service at the institution is dependent on the insurance organisation; this would have shed light on the low incidence of maternal and perinatal complications.
Strengths include the fact that all pregnant women were tested for HbA1c and blood sugar levels upon entry in the study; HbA1c samples were processed in accordance with international standards and the results were reported to the researchers on the same day and immediately to the healthcare centre; a second confirmatory test was performed in all the pregnant women who had an initial HbA1c ≥ 6.5%.
CONCLUSIONS
In this sample, the prevalence of GDM was found to be 4.7% (12/256) in accordance with the 75 g OGTT result in the period between 24 and 28 weeks. Population studies are needed in order to arrive at more accurate and valid estimates and gain a better understanding of the size of the problem in Colombia.

