











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink
INTRODUCTION
The medical student, in addition to knowledge about health and illness, must develop capacities for an adequate relationship and communication with patients. This interaction, defined as empathy, has been considered an essential factor in the patient medical relationship 1, the ability to understand the situation of others, and caring for patients with compassion, are dimensions of empathy that are closely associated with an adequate doctor-patient relationship 2,3.
In the medical career, the results of the measurement of empathy levels in the different courses have been contradictory: lower scores in some cases 4, and higher in others 5,6. This also happens with other health careers in general 7,8. Empathy levels show variability around the "course" and "gender" attributes 1,9,10,11. In Latin America, variability is also observed between, and within, Faculties of Medicine of the same country, as well as between countries 9.
Likewise, empathy is presented differently, depending on the type of family, and family functioning that one has. According to Olson’s family and marital system circumplex model 12, there would be three types of families by combining the dimensions of cohesion and adaptation:
1. Balanced level, which corresponds to a flexible or structured operation; they are families that have openness to change, and a greater capacity, as a system, to modify their rules and regulations, according to the requirements they face. 2. Rigid or chaotic level, where the guidelines and norms that govern family functioning tend to be extremely rigid, with a low willingness to modify these pre-existing guidelines, even when the situation warrants changes.3. Extreme level, predominantly agglutinated families, characterized by a strong emotional bond between their members, which negatively affects the process of individualization of the members.
It is permissible to assume then, that there is influence of the family in the social, personal, and empathy development of its members, making the influence of family functioning, in extra-family systems, very important. Indeed, studies by Shaffer et al. 13) have suggested that the well-being of doctors is a result of their early family relationships, which affect and predict their positive functioning. In this regard, Weiner et al. 14 reviewed the effect of family relationships, of the family of origin, on the well-being of doctors, and found that emotional closeness between family members was a predictor of positive relationships, and, therefore, of empathic attitudes.
The objective of this study is to explore the distribution of general, and particular, levels of empathy, among different family functioning styles of medical students of the University of Azuay, in the city of Cuenca, Ecuador.
MATERIALS AND METHODS
This was a cross-sectional descriptive study seeking to survey all medical students at the University of Azuay. The Jefferson Medical Scale of Empathy, S-version (JMSE-S), and the Faces-20 Family Functioning Scale were previously submitted to cultural validation, using judged criteria. Four experts examined the questions, in order to adjust the concepts to the cultural environment, and to avoid confusion or subjective influences that distort student responses, which was examined through a pilot application.
The application of the surveys was carried out by a neutral investigator, in March 2015, during a regular class session of the students, safeguarding the anonymity and confidentiality of the information, by signing an informed consent approved by the ethics committee, and following the declaration of Helsinki. A total of 278 students of the Medicine course of the University of Azuay (Cuenca - Ecuador), enrolled for the academic period corresponding to 2015, were included, covering 98.2% of the student body. One hundred sixty-six women (59,7%) and 112 men (40,3%) participated, with a range between 17 and 41 years of age (M=20.88, SD=2.78), distributed in six courses or educational levels: 1st. year (n = 72), 2nd. year (n = 92), 3rd. year (n = 24), 4th. year (n = 45), 5th. year (n = 17), and 6th. year (n = 28).
The Jefferson Medical Scale of Empathy, S -version(JMSE-S), is based on the Jefferson Scale of Medical Empathy (JSME)3, being a specific version for medical students (s version) validated by Alcorta-Garza et al. 2 in Mexican medical students. This is a multidimensional scale that considers three components: a) "Take on perspective", b) "Care with compassion" and c) "Ability to understand the situation of the other". "Take on perspective" refers to the ability to spontaneously adopt the point of view of the other, and has a close relationship with the reasoning that the person performs to represent the beliefs and intentions of that other. "Care with compassion" refers to the possibility of issuing an appropriate emotional response to the emotional state that others present. Finally, the "Ability to understand the situation of the other" is a cognitive component that allows adopting the perspective of the other, understanding their feelings, to infer and predict the behavior of the other15. The Spanish version consists of 20 items, organized on a Likert scale of seven response levels, from 1(strongly disagree) to 7 (strongly agree), giving scores between 20 and 140, to measure the three dimensions or subscales of the construct: 10 items evaluate "Take on perspective" (10 to 70 points), 7 items evaluate "Care with compassion" (7 to 49 points), and 3 items for "Ability to understand the situation of the other" (3 to 21 points); without establishing cut-off points to constitute categories of low or high empathy.
The JMSE-S has an adequate construct validity, convergent, discriminant, high internal consistency (cronbachfs alpha between 0.80 and 0.90), and adequate stability coefficients 1,2,10-11.
The FACES-20 Family Functioning Scale was also applied. The scale measures the dimensions of cohesion and adaptability, based on the Olson marital and family systems circumplex model 12,16. This test consists of 20 Likert scale items, with scores per item ranging from 1 (strongly disagree) to 5 (strongly agree), forming two dimensions of 10 items each. Cohesion essentially refers to emotional union, that is, the degree of connection that the individual perceives in the relationship with their system (items 11 and 19), to emotional support (items 1 and 17), to internal and external family boundaries (items 5 and 7), to the time dedicated to the family, and the physical space available for family gatherings, with friends, in communion (items 3 and 9), and the degree of individual participation in shared activities and interests by the family group (items 13 and 15). The adaptability dimension investigates leadership (items 8 and 18), the degree of control (items 2 and 12), discipline (items 4 and 10), and roles and rules (items 8, 14, 16 and 20).The measurement made by the scale has shown high reliability coefficients in different populations, reaching a Cronbach's alpha of 0.89 in the cohesion dimension, and of 0.87 in the adaptability dimension, when applied in the Chilean population 17.
Statistics Analysis
The Kolmogorov-Smirnov test was used to establish the normality of empathy and its dimensions, and the Levene test of equality of variances, to test homoscedasticity.
To analyze the behavior of the variable, the mean and standard deviation of the general empathy, and each of its dimensions, were estimated. Subsequently, a Variance Analysis (ANOVA, Model III) was applied, with weighted least squares analysis (compensated by academic year). To assess the size of the effect, the square eta (η2), the power of the test (1-β: type II error), and the corrected coefficient of determination of the regression of weighted least squares per academic year (R2), were estimated. The distribution of empathy in the factors of family functioning style (FFS), gender (G), and the interaction between both factors (FFS * G), were evaluated.
In cases where ANOVA was significant, the Tukey multiple comparison test was applied to define the order of differences between empathy means and their dimensions, according to factor levels. The used level of significance was α≤ 0.05 and 1- β ≤ 0.20. All analyzes were performed using the IBM SPSS Statistics 22 program (IBM Corp., 2011).
RESULTS
Empathy means, with standard deviations (SD) and standard errors of the mean (SEM), are shown in Table 1. Empathy presented a normal distribution (p>0.05), with homogeneous variances when segmented by gender and FFS (p> 0.05). The ANOVA F test of the distribution of general empathy was significant for the FFS factor (p<0.05, η 2=0.023, 1-P=0.602). Concerning the gender factor and interaction (FFS * G) they were not significant (p = 0.077 and p = 0.104 respectively), with the regression model reaching a value of R2=0.049. Regarding empathy, on the "Take on perspective" dimension, the results of the ANOVA were significant for the FFS factor (p=0.035, η2=0.024, 1-β=0.718); there are no effects associated with gender or interaction (FFS*G) (p=0.293 and p=0.478 respectively), with a value of R2=0.24. On the other hand, in the "Care with compassion" dimension, no significant differences were observed in any of the factors (FFS: p=0.117; gender: p=0.07; FFS*G: p=0.207). For the "Ability to understand the situation of the other" component, the FFS factor was significant (p=0.044, η2=0.016, 1- β =0.449), however gender and the interaction between both factors were not significant (p=0.579 and p=0.124, respectively).
Table 1 Estimation of observed means of empathy in general according to family functioning and gender
FFS=Family functioning style, M=Mean, SD= Standard deviation, SEM=Standard error of the mean.
Source: Elaborated by authors.
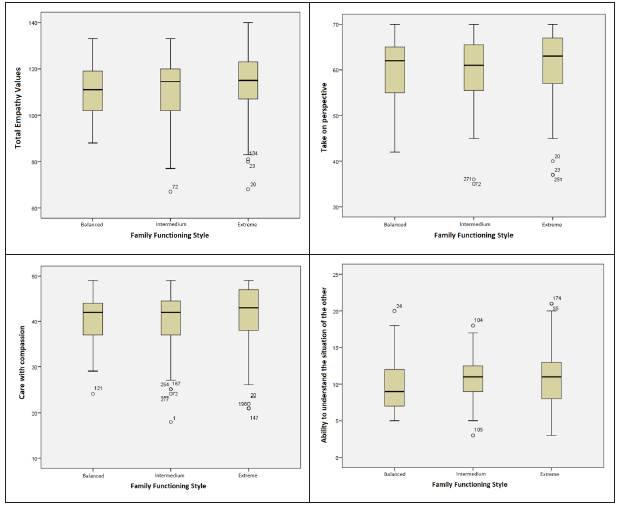
Table 2 shows the results of the application of the multiple comparison test of empathy means in general, and for each of its components, according to family functioning styles. In the general assessment of empathy, it was found that the average of the extreme family functioning style has values of empathy greater than that of the intermediate style, with significant differences between them (p<0.05); however, the mean balanced style does not differ from the other styles (p>0.05). The same relationship, indicated above, is evident when the empathy means of the three family functioning styles were compared in the "Take on perspective" component (p>0.05). In the "Care with compassion" component, no significant differences were observed between the means of empathy of the studied family functioning styles. Finally, in the "Ability to understand the situation of the other" component, there was a greater average of empathy in the intermedium style with respect to the balanced style, resulting in significant differences between them (p<0.05); the mean of the extreme style is between the above mentioned means, and does not differ significantly from them (p>0.05). Comparisons of empathy means according to family functioning styles can be seen in Figure 1.
Table 2 Multiple comparison between the observed means of empathy according to family functioning
M= Mean, SD= Standard deviation
Source: Elaborated by authors.
Source: Elaborated by authors.
Figure 1 Means of empathy and its dimensions according to family functioning styles
The observed significance of the distribution of empathy in the FFS allows to state that there are differences in the levels of this factor. In this case, the effect size is small (η2 =0.044), and, therefore, the found differences may not be so relevant.
The power of the test was relatively less than the normally accepted value (0.80), so the sample size also plays an important role.
DISCUSSION
The objective of this study was to explore the distribution of general, and particular, levels of empathy among the different family functioning styles of medical students of the University of Azuay, in the city of Cuenca, Ecuador.
Regarding gender, several authors have found that this factor influences the distribution of empathy 18,7,19,1,10,11,20,21, however, other studies indicate that such differences do not have to be necessarily present, because in some cases, empathy is similar in women and men 18, just like in the present study.
The lack of significance in this factor in interaction with the FFS, and the low value achieved by R2,implies that such interaction does not generate an effect on empathy, a finding consistent with that reported by Sandoval et al. 22, and if it does, it would be in such magnitudes that can be considered, from the causal point of view, as a complementary contributor 23.
Regarding empathy and family functioning, on the "Take on perspective" dimension, the results of the study were significant for the FFS factor. Regarding their interaction with gender (FFS*G) there were no significant results. On the other hand, in the "Care with compassion" dimension, no significant differences were observed in any of the factors (FFS; gender; FFS * G), results consistent with the findings of González-Martínez et al. 19.
In the "Ability to understand the situation of the other" component, the FFS factor was significant, results that coincide with those of Madera et al. 24, who concluded that family functionality could be responsible for generating awareness and understanding behaviors towards the patient. However, the results for gender, and the interaction between both factors, were not significant (FFS * G).
It was found, in the general factor, that extreme family functioning styles have empathy values greater than the intermedium style, with significant differences between them. A similar situation arose when comparing the "Take on perspective" and "Care with compassion" variables, showing significant differences between intermedium and extreme style, in favor of the latter. Therefore, it can be attributed that this type of family functioning contributes with certain formative factors that may have an impact on the development of empathic values 22.
Extreme families are often considered chaotically attached, chaotically detached, rigidly attached, or rigidly detached 12. It is possible that these conditions contribute to the development of attitudes of empathy, especially if the family shows a rigid attachment, even if it is chaotic, since its strong demand for fidelity and loyalty to its members 25) could imply the development of skills to put oneself in the place of other. Family communication has been considered as a promoter of empathy, as it encourages to listen and reflect, to offer support 26.
In fact, the expression of affection, functional communication, and family support variables, are highly correlated with empathy in resident doctors 22. In the case of extreme families, these values may be present, although they may be erratic or strict 27, however it would be interesting to review the communication, support, and expression of affection positive variables in these types of families, that contribute to the development of empathic attitudes, through new research.
However, it has been suggested that the development of empathy is related to positive perception, the result of open communication, present in family relationships that express affections, adapt their rules, and are flexible 22. In the case of extreme families, the authoritarian or absent leadership that characterizes them, affects communication 27.This relationship has been criticized for a series of limitations in the studies that support it, and the tendency of researchers to simplify the characteristics of family communication, and reduce it to good, bad, positive, or negative 13,11,27. On the other hand, these families can function well if there is a high level of satisfaction on the part of all their members with this family dynamic 25, satisfaction that apparently has implications with their ability to listen and reflect, that is, in communication, and consequently, in the deployment of empathic behaviors.
The characteristics of the extreme families in the context of Ecuadorian culture should be reviewed, since it is likely that what is considered extreme does not necessarily mean erratic. Indeed, perceptions of behavior tend to vary between cultures 28, as well as in certain areas, affected by family functioning 29, so communication in extreme families is not necessarily affected.
Previous studies have demonstrated the value of family support in the development of empathic behaviors 13, although they have not reviewed typology and family functioning, certain family values have been considered for their involvement in the development of this attitude, such as emotional closeness among family members. The family unit influences the individual's ability to cope with the daily tensions of life, their professional functioning, and their psychological health 14. Precisely, the family trait that stood out the most in the study, cited as a predictor of well-being in doctors, was the individualization in the family of origin, that is, the possibility that family members have in maintaining their rights, identities, beliefs, and points of view, in relation to the other members. It is worth asking whether extreme families maintain these traits, which apparently are promoters of empathic behavior. Additionally, the degree of support from family and friends was correlated with the development of empathy in male students, but not in female students 30.
There is a possibility of involvement of other variables, such as contact with patients, training in subjects that treat the doctor-patient relationship, and experiential factors, such as the experiences of critical situations in health services, which could contribute to the development of empathy 31. Additionally, it would be useful to review whether these attitudes of empathy, shown by medical students, are maintained when they exercise their profession, since it has been shown that professional exhaustion could be related to a decrease in empathy 30.
A single variable showed greater significance in the intermedium operating style: "Ability to understand the situation of the other", compared to the balanced style.
The intermedium style seeks balance between chaotic, rigid, flexible, and structural conditions, all of them in their connected or separate categories 12. These families have the ideal communication characteristics to promote empathic attitudes 25, which apparently are not remarkable, because they have not affected neither the other two empathy variables analyzed, nor the general variable.

