











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink1. Introduction
In Colombia, the population with limited movement of the body, hands, arms, and legs is approximately 21% nationally, while it is 35% in Cauca Valley [1]. As a result of these disabilities, patients have limitations in activities of daily living (ADLs); 21% do not perform general tasks and 31% have mobility problems [1]. For this reason, the quality of life of people who suffer some type of injury is affected, as they are unable to perform certain tasks. The 2010 census, conducted by DANE, showed that the most accepted methods for rehabilitation treatments are medications with 58%, physical medicine with 16%, and physiotherapy with 22% [3]. Physical rehabilitation treatment includes three procedures: elimination of inflammation and reduction of joint pain, recovery of mobility, and muscle strengthening. According to DANE [3], the quality of the rehabilitation service is commonly negatively affected by the lack of money for travel (64%), lack of a companion (4%), and distance from the care center (6%). These factors are responsible for the increase in risk of geographic vulnerability of the population, so designing telerehabilitation equipment is clearly needed to reduce these effects.
This study focuses on the recovery of mobility and muscle strength by facilitating active and passive rehabilitation treatment protocols in patients with a transitory disability. By using telerehabilitation, the system seeks to minimize the barriers imposed by the centralized medical service in Colombia. This research problem poses major challenges, such as safe remote operation, treatment traceability, basic Internet connection, active and passive rehabilitation, and complying with medical protocols.
In the review of the state of the art equipment for shoulder rehabilitation, several systems or machines were found worldwide [5,6]. These machines run the gamut from conceptual proposals [15] to commercial products [5,8,9], and the following were described: a device with characteristics that provide safe conditions for the patient [5]; a shoulder rehabilitation system at the prototype level [10]; a system allowing several people to be attended to at the same time (although locally) [11]; and a virtual tool guiding the patient in treatment implementation [8]. Other studies had limitations: one prototype did not consider ergonomics or the anthropometrics of patients [9]; one study described a device allowing muscle strengthening, but not the traceability of rehabilitation [12]; and one study explained a conceptual design proposal without describing the machine construction [7]. Kiguchi [13] illustrated an exoskeleton that was developed to ensure treatment continuation and support body weight loading, because it was designed for people with motor skill problems. Finally, Ayala [6] proposed a machine with characteristics that allow treatments to be carried out in a bipedal position, which may be inconvenient for its application in other disabilities.
In the search for related studies, no references were found proposing an integral solution for the population with geographical vulnerability, which should consider aspects of synchronous remote operation, permanent monitoring of the patient by the specialist, implementation of active and passive treatments, patient comfort, anthropometry for the Colombian population, functionality, user safety, and traceability of the rehabilitation protocol, among others. In this context, the importance of this study lies in considering all these aspects, under the framework of one of the branches of telemedicine: remote operation. This would allow decentralizing the Colombian health system related to human rehabilitation, by extending coverage to the population with geographical vulnerability due to problems with access to specialized rehabilitation services [14].
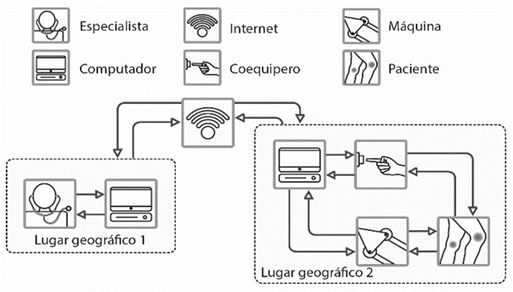
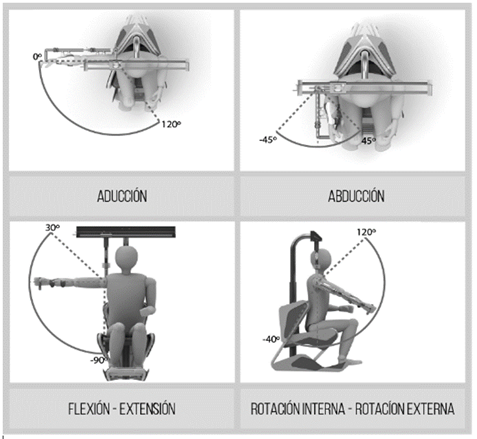
The design of an assistive technology device for shoulder rehabilitation involves high biomechanical complexity because the shoulder joins the trunk with the upper limb, and in conjunction with the elbow and wrist allows positioning of the hand in space. The shoulder involves the gleno-humeral, acromio-clavicular, sterno-clavicular, and scapulo-thoracic joints, which are integrated with the muscles and ligaments, allowing joint mobility [4]. This implies considering three degrees of mechanical freedom in the design, whose movements are: flexion-extension (sagittal plane), abduction and adduction (frontal plane), and internal and external rotation (arm in adduction). In addition, the proposal must be coupled with service-oriented architecture to enable a remote system. Fig. 1 shows the proposed telerehabilitation system.
The modeling of the assistive technology device with colored Petri nets is also shown; this modeling is related to the anatomical movements, as well as the maximum and minimum angles that can be achieved by the assistive technology device according to the anatomical movements. Finally, the tests of a shoulder telerehabilitation service are shown, along with screen captures of the data insertions or modifications in the database verifying the implementation, validation, and integration of web services required for service-oriented architecture.
2. Methods and instruments
2.1. Power unit for the telerehabilitation assistive technology device
The power unit for the assistive technology device was designed with the aim of performing active and passive treatment with the same device because these two treatments are essential for full patient recovery. In passive treatment, the patient regains lost mobility, and in active treatment, the patient regains muscle strength. In addition, rehabilitation procedures will have a traceability that could be consulted by the specialist on duty, which will allow specialists to make decisions for the definition of new rehabilitation protocols.
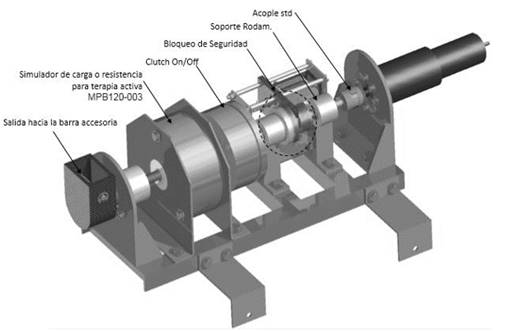
The power system consists of the following components: a motor-reducer, a clutch, and a magnetic brake. The motor- reducer is responsible for performing the movement of the patient's limb when in passive treatment, the clutch is responsible for decoupling the motor when switching from passive to active treatment, and the magnetic brake is responsible for opposing resistance to the patient at the time of active treatment. The information from both active and passive treatments is obtained through the control and communication system and is updated in each patient medical record. Fig. 2 shows the power unit for the rehabilitation assistive technology device.
2.2. Biomechanics of the shoulder joint
In the cinematic and kinetic analysis, the maximum range of movement, center of gravity, and static loading conditions were defined, in order to determine the power needed to move the upper limb (arm). Fig. 3 shows the upper limb segments, the points of application of the weight of each limb, and their lengths with respect to the shoulder joint. Based on the free body diagram, the torque needed to move the upper limb were determined. This kinetic analysis was performed considering a person with a weight of 130 kg, which is well above the mean of the Colombian population. This consideration allows the design to be appropriate for the 95th percentile of the population [15].
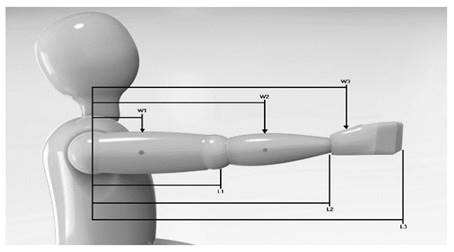
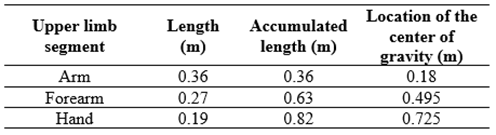
Table 1 shows the weight of each upper limb segment. Segment 1 corresponds to the arm, Segment 2 to the forearm, and Segment 3 to the hand. The weight ratio of the segment is related to the total weight of the person; in this case, the reference is the above-mentioned 130 kg.
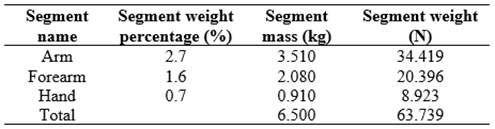
Fig. 3 shows the length of each arm segment. Table 2 shows the lengths of each upper limb segment, determining their centers of gravity.
To select the final control element that will generate arm movement, it is necessary to know the torque necessary to move each segment independently. Where the total torque consists of the static and dynamic torque, the torque calculated for each segment must be added to obtain the total torque needed to move the entire upper limb. Table 3 shows the results of the static torque for each segment. The effect of the dynamic torque is only 1%. In addition, in the total torque, a safety factor of 1.3 was considered to ensure anomalous system operating conditions (undue manipulation of the assistive technology device) and any possible damage.
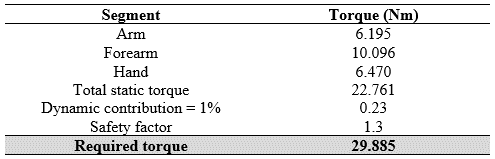
According to the results shown in Table 3, it was concluded that the actuation system should use a motor-reducer assembly with a minimum torque output of 30 Nm.
3. Results
In the results, the characterization of the variables used by the power unit is initially shown, and then the design of the assistive technology device coupled with the power unit is explained. Subsequently, the modeling with colored Petri nets of the operation of the assistive technology device in terms of anatomical movements and their maximum and minimum ranges is shown. Finally, the result of a remote treatment system via the Internet is shown with the help of technology integrated into the architecture.
3.1. Characterization of the power unit variables
3.1.1. Speed reference of the power unit
The speed reference will be given in degrees per second; however, motor speed control requires a reference in frequency rates. Next, the data and the graph obtained from the power unit are shown.
The real data obtained from the power unit are compared with the expected data with which the design was made; Table 4 shows these data with their respective error rates.
Table 4 Comparison of theoretical and practical angular velocity data from the power unit
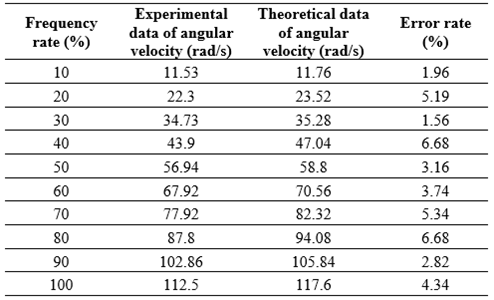
Source: authors
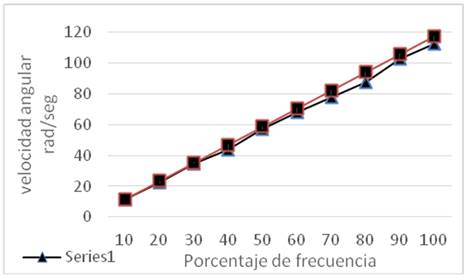
Fig. 4 shows the two curves, both theoretical and experimental, in order to measure the motion error and take into account the efficiency of the motor reducer. The data of Series 1, represented by triangles, are the experimental data and the data of Series 2, represented by squares, are the theoretical data. From the error calculated in Table 4, it can be determined that the highest error value could be approximately 6.68%, which causes an offset of the angular speed of approximately 1.5 or 2 rad/s, a value that does not affect the provision of the rehabilitation service and does not affect the physical integrity of the patient.
3.1.2. Characterization of the angular position of the power unit
It was necessary to test the power system regarding its instrumentation for measuring the angular position at the output of the power unit because these data are essential for recording and updating the rehabilitation treatments in the patient medical records. Calibration of the linear potentiometer was performed by measuring potentiometer voltage versus its angular position; the results were plotted and are shown in Fig. 5. The function obtained in Equation 1 was used in programming the microcontroller, to obtain the desired angular position in degrees (º).
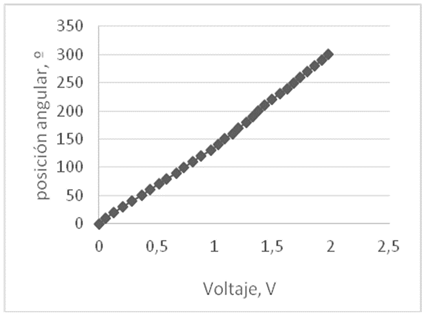
With the obtained data, it was possible to obtain the linear function shown in Eq. (1).

3.2. Assistive technology device for shoulder rehabilitation
The assistive technology device for shoulder rehabilitation allows the patient to perform active and passive rehabilitation movements in three degrees of freedom, which are shown in Fig. 6; this means that patients recover mobility and muscle strength in six joint movements. These three degrees of freedom are achieved using the power unit coupled to the mechanical system.
Once all the requirements of the elements were integrated and the conceptual design was established, the design proposal was elaborated, where the building blueprint of the parts and components to be used was developed in detail.
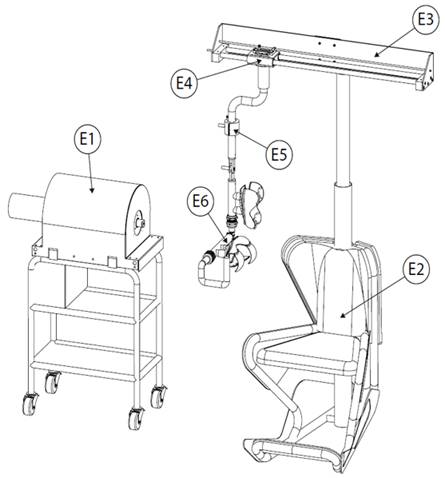
Fig. 7 shows the final design proposal, with all its components and sub-assemblies: power unit (E1), chair (E2), upper frame (E3), carriage (E4), motor unit (E5), and arm (E6).
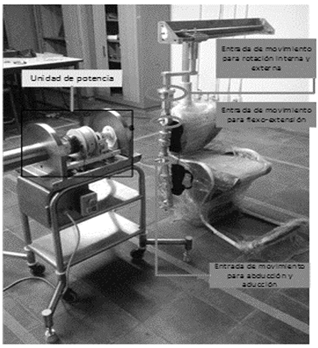
Next, the prototype of the shoulder assistive technology device was designed, built, and implemented with the service-oriented architecture for telerehabilitation systems. Fig. 8 shows the prototype, indicating motion inputs according to the rehabilitation protocol to be implemented.
3.3 Modeling with colored Petri nets of an assistive technology device for shoulder telerehabilitation
Validation of the assistive technology device design for shoulder rehabilitation was tested by means of simulation with colored Petri nets; these simulations were used to validate the degrees of freedom and maximum and minimum movement ranges of the assistive technology device when carrying out telerehabilitation. Fig. 9 shows the system model detailing all the anatomical movements that can be rehabilitated by the assistive technology device.
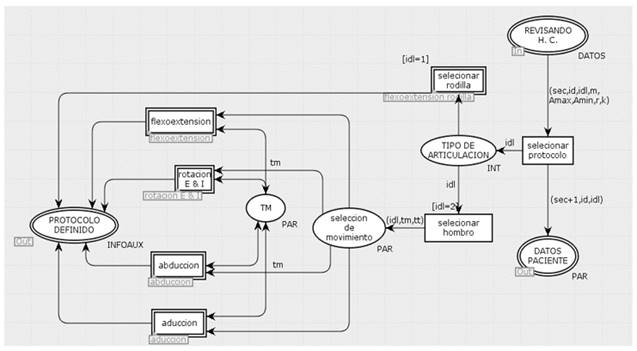
In Fig. 9, each movement shown is a substitution transition, which means that it is a new net characterizing each movement independently. Figs. 10-13 show each movement for rehabilitation; this modeling is necessary for characterizing each movement in terms of its maximum and minimum ranges and for decision-making when a protocol is poorly defined by the specialist.
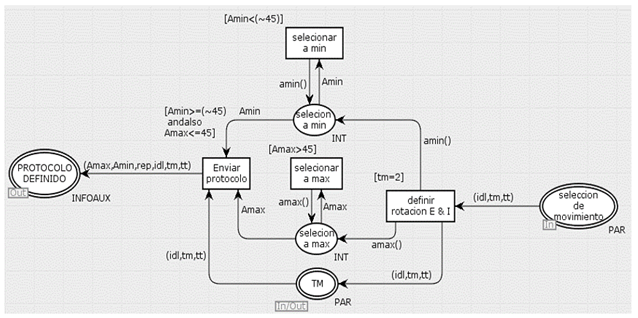
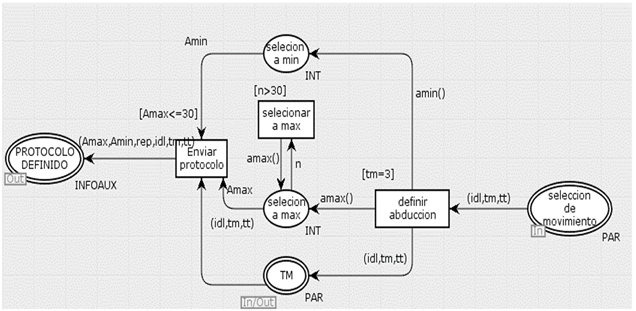
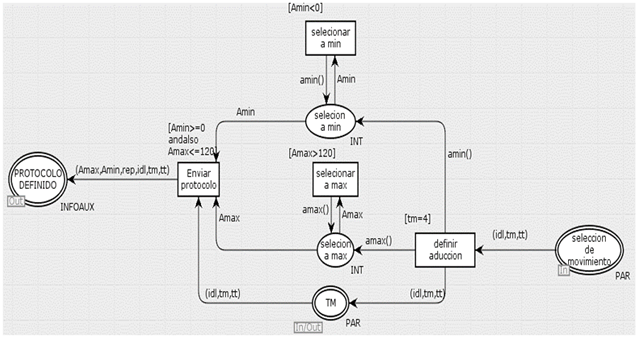
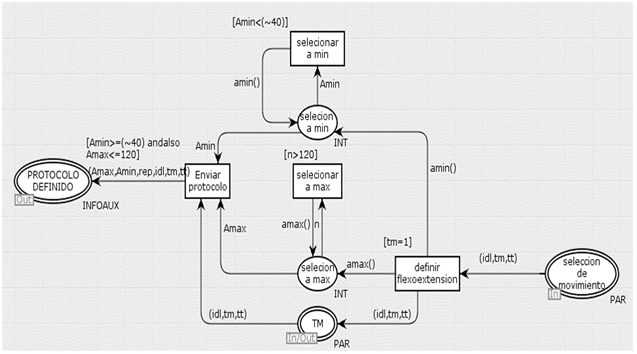
The possibility of selecting active or passive treatments was also included in the model, so that validation with colored Petri nets was as close as possible to the proposed system.
3.4. Comparison tests of the angular position of the power unit
To validate the design of the anatomical movements of the shoulder assistive technology device, tests were performed, which consisted of comparing angular values entered by the specialist with measuring the angular output of the power unit. Table 5 presents these values, and Fig. 14 shows comparative graphs between theoretical and experimental values.
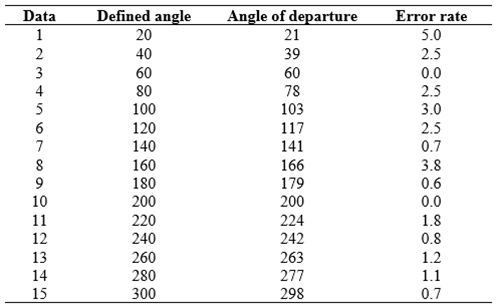
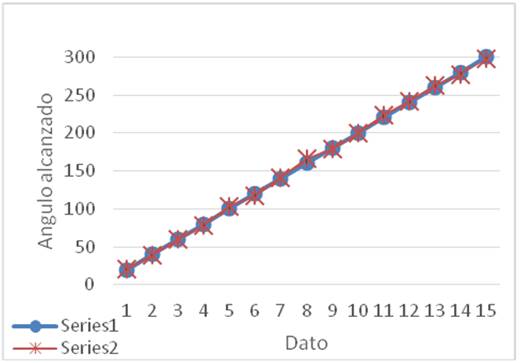
Fig. 14 shows the theoretical angular position values of Series 1, represented by circles, and the experimental angular position values of Series 2, represented by asterisks. For these data, error rates are low because the maximum value is approximately 5%, which would indicate that in rehabilitation, an error between 3 and 4 degrees could occur according to what is defined by the specialist in the protocol.
3.5. Design and development of web services for the implementation of service-oriented architecture for telerehabilitation via the Internet
To implement service-oriented architecture, it was necessary to design, develop, and coordinate the web services proposed in the architecture. Next, in Figs. 15-18, the process diagrams of the four services and their interaction with the actors of the telerehabilitation system are shown.
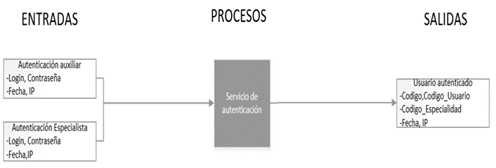
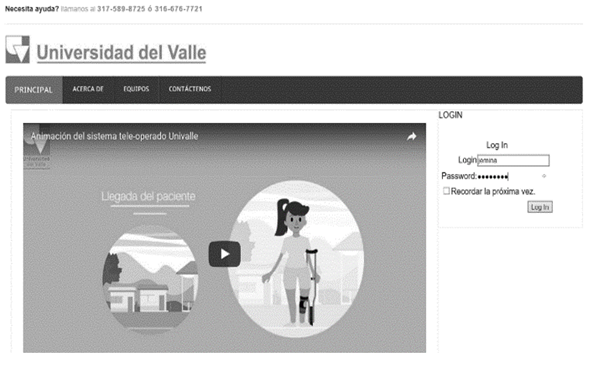
3.5.1. Authentication service
Fig. 15 shows the authentication service model, representing its inputs and outputs. This service is responsible for authenticating users and providing them with an interface, according to their role as a specialist or assistant.
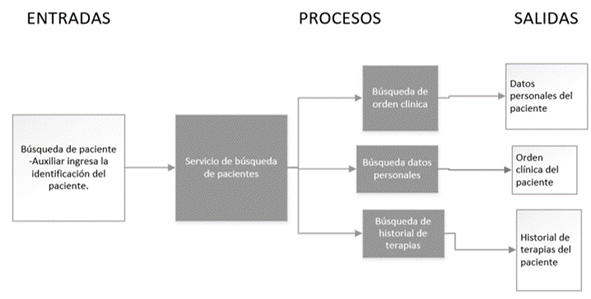
3.5.2. Patient search tool
This tool is responsible for searching in the patient database and classifying patient data in different categories to facilitate access to the appropriate information for each agent in the system. The classified information is related to general patient information and treatment information. Fig. 16 shows the service as a process, indicating its inputs and outputs.
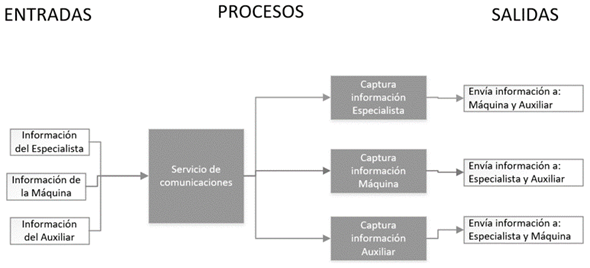
3.5.3. Communication service
This service was present throughout treatment implementation, to maintain a permanent communication between the assistive technology device and system agents. Fig. 17 shows the process diagram of this service.
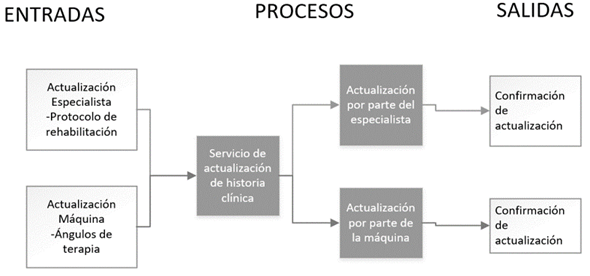
3.5.4. Medical record update service
Fig. 18 shows the process diagram of the medical record update service, which is responsible for recording in the patient database the information related to the treatment performed or any possible eventuality that may arise and need to be recorded in the medical record.
These four services were designed, developed, and implemented to employ service-oriented architecture for telerehabilitation via the Internet. These services were integrated and coordinated so that the events corresponded to what was defined in the design. The characteristics of the services are that they do not keep the event state-which allows them to return to their initial state-they fulfill specific functions, and they have low coupling-allowing them to be independent-therefore making the system resilient to failures, so that a possible failure in a service does not affect the entire system and is easy to identify. These services are present once they are available, and their access protocol is universal. Finally, the system is scalable, as it can be scaled to one of greater or lesser complexity by coupling or decoupling the required services.
3.6. Implementation tests of service-oriented architecture for the shoulder telerehabilitation system via the Internet
Once the services have been presented, functional tests for shoulder rehabilitation are performed. In this case, the system behaves optimally without any type of eventuality while providing the rehabilitation service; this is done in order to evaluate and validate the architecture and the services developed for its implementation.
The process begins with user authentication, followed by specialist registration, in the application interface, which gives the option of entering a login and password as shown in Fig. 19 according to the data provided by the person to the web service (called “user authentication”)-and searches the hospital database to confirm if the authenticated person is a specialist or assistant.
When the specialist is authenticated, this event is recorded in the database, as shown in Fig. 20. The database provides information of the authenticated person: their specialty, their last access, and the IP address of the access point; this allows monitoring of the specialists and assistants who perform telemedicine tasks in the respective hospitals.
Once the specialist is authenticated, the application opens a new screen showing the user, connection IP, and date and time of the start of the last session as a specialist, as shown in Fig. 21. In addition, the system is on standby to receive information about the patient waiting for treatment.

Once the assistant is authenticated, the same thing happens as with the specialist; there is an entry in the database with the authenticated assistant information, as shown in Fig. 22.
The assistant performs the same procedure as the specialist in terms of registration. Once registered in the assistant's interface, the following data appear: user, IP, date, last access, and a prompt to enter the identity document of the incoming patient. The requested information is shown in Fig. 23.

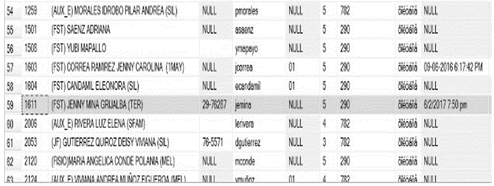
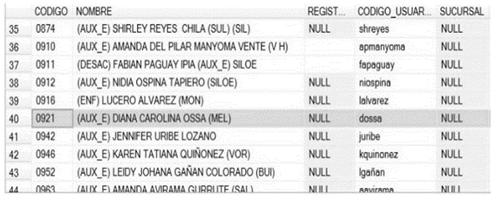
Once the assistant enters the patient identity data, a search of the patient database is performed. The web service called “patient search” performs this procedure, and the assistant's interface is updated with patient data. The updated data corresponds to general patient information, as shown in Fig. 24.

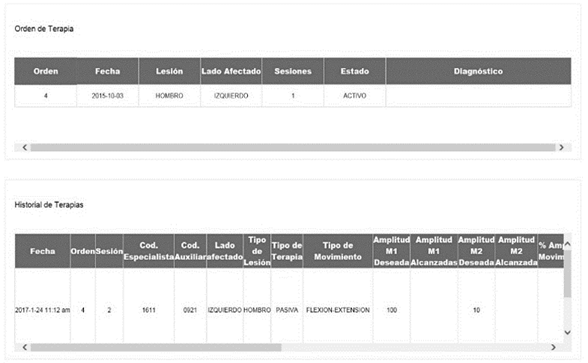
Fig. 25 shows medical record data related to rehabilitation treatments. It is observed that the left shoulder is injured; this information is obtained from the treatment order found in the patient medical record.
The patient search is recorded in the database; its record is shown in Fig. 26. This database contains general information and that related to rehabilitation, as well as administrative information such as the medical order, which defines the type of injury and injured side.
Because the assistant already registered the patient when entering their identity document number, the information obtained by the patient search service is sent to the specialist's interface, which displays general patient information such as treatment order and treatment history, so that the specialist may have information about the patient to be attended.
Next, the events related to the communication web service are shown. This service is mainly linked to the input and output information of the assistive technology device. As shown in Fig. 27, in the specialist's interface, specialists have the possibility of filling the fields related to the rehabilitation protocol. Unlike knee rehabilitation, the specialist can choose between six anatomical movements to be performed by the shoulder. It should be noted that some fields cannot be modified because they are defined by the treatment order entered in advance into the database. The reason for this is to reduce the possibility of errors by the specialist because of not having direct patient contact.
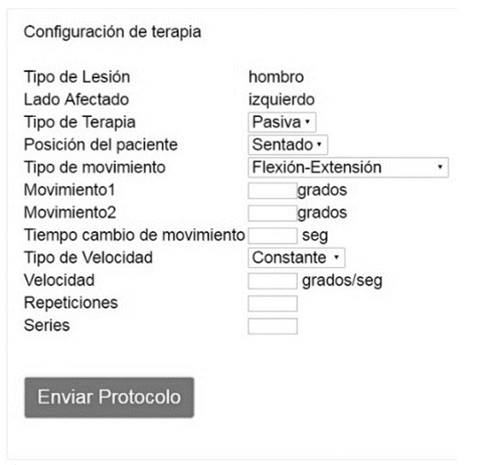
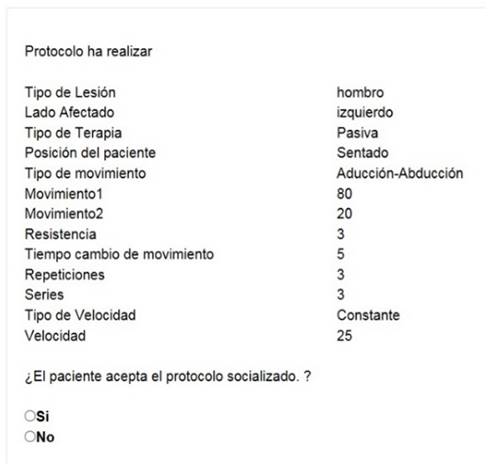
Fig. 28 shows the protocol sent by the specialist as received by the assistant. This protocol can only be read and cannot be modified by the assistant; also, in this event, patient choice to accept the protocol is shown.
Once the protocol is received and accepted by the patient, this information is managed by the assistant and entered through the interface designated for this function.
The confirmation of acceptance of the protocol by the patient and the optional observation entered by the assistant then arrives at the specialist's interface.
Once the specialist receives the confirmation from the patient sent by the assistant, the specialist has the option to start treatment or not; this function is used to ensure patient treatment safety.
The data obtained by the assistive technology device during the course of treatment are recorded both in the specialist's interface and in that of the assistant, in order to monitor treatment implementation and check if the protocol data are correct in comparison with the data available to the assistive technology device for execution.
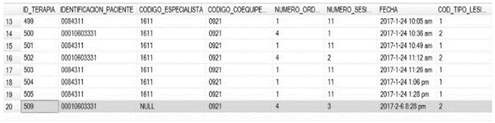
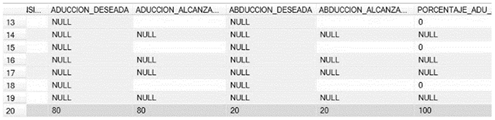
Once the treatment is finished, the database is updated, and the desired data are compared with the range of motion achieved by the patient during treatment. Fig. 29 shows the entry of this information in the database with the success rate of treatment implementation.
Finally, the system generates a last update of the patient medical record with the data of the treatment performed. In this way, service-oriented architecture was implemented for a telerehabilitation system via the Internet.
4. Discussion
The assistive technology device prototype was verified to comply with the maximum angles defined by the biomechanics of the shoulder, rejecting the rehabilitation protocol when the data exceeded the established values, which proves that the procedure is safe for the patient. In addition, according to the literature found, this is the only prototype incorporating both active and passive rehabilitation.
Web services allow a more efficient remote operation in terms of resource use and connection to the Internet because only plain text is transmitted and the system is resilient to failures.
The system was designed to be synchronous and implemented as such to ensure patient safety, guaranteed by the permanent presence of the specialist during the course of rehabilitation.
The system allows continuous recording in the database of the treatment performed; this information is stored in the patient medical record, allowing traceability of the progress of treatment sessions.
The integration of web services was done in an adequate manner, evidenced by the organized flow of information, and all records were entered into the database.
5. Conclusions
This assistive technology device for active and passive shoulder rehabilitation was incorporated into a service-oriented architecture, first designed and later implemented, thus allowing patients who are temporarily disabled to achieve rehabilitation. Rehabilitation is ensured because the protocols for active and passive shoulder movements are being followed.
The information entered into the database allows the specialist to have traceability of the rehabilitation processes of their patients; in addition, remote access to the information recorded in the database is possible.
Implementing service-oriented architecture with the assistive technology device was successful because it was possible to verify the flow of information between Geographic Location 1, Geographic Location 2, and the server in addition to the correct functioning of the mechatronics of the assistive technology device.
The results and tests performed in this project are related to prototype construction; in future projects, it is proposed to move from the prototype to product development.

