











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
1. Introduction
Lean manufacturing (LM) is a methodology originating from the automotive industry, which seeks to maximise value by eliminating waste [1]. This focuses on improving operational efficiency by reducing activities that do not provide value to the end customer, ensuring a more agile and less costly production [1]. Thus, in healthcare, the concept of lean healthcare (LH) seeks to optimise hospital processes to improve the quality of care and reduce costs by systematically eliminating waste in the management of healthcare services.
An efficient healthcare system requires advanced technological infrastructure, trained staff and optimised processes [2,3]. In this context, the need for innovative techniques to improve quality and patient safety has been emphasized [4]. However, hospitals must continuously refine the efficiency of their processes to respond to increasing demand and the addition of new services [5].
LH and Industry 4.0 (I4.0) are transforming healthcare systems by optimising processes without compromising service quality [6]. The application of lean principles has been shown to reduce process times [7] while digital simulation validates interventions prior to implementation [8]. In addition, the integration of LM tools with I4.0 technologies facilitates tactical and operational decision making, for example, through predictive analytics and workflow modelling in virtual environments to improve operational efficiency and reduce waiting times [9,10]. On the other hand, sustainability in healthcare systems is achieved by integrating quantitative models that optimise resources and reduce waste. This approach aligns with LH and I4.0 methodologies, which seek to improve operational efficiency and ensure an optimal experience for patients and medical staff [11].
Previous literature identifies operational waste such as unnecessary patient transfers and excessive specimen transport times [12,13]. Also, the integration of LH with I4.0 technologies allows addressing these issues through better resource allocation and workflow optimization [14]. This drives a healthcare model that is more agile, efficient and better able to respond to changes in demand, ensuring an optimal experience for both patients and medical staff. In addition, operational waste affects service quality, increases costs and raises the risk of adverse events [15]. In this sense, LH principles are of particular importance in hospital management in terms of safety and quality of care [12].
Therefore, this paper aims to reduce hospital waiting times that currently affect operational efficiency and quality of care by generating delays in diagnosis and treatment. Our motivation is aligned with the growing challenges in health services management, where the demand for care often exceeds the operational capacity of hospitals. In that context, by identifying bottlenecks (BO) and optimising the use of resources through I4.0 technologies, such as simulation, more effective decisions can be implemented to improve operational efficiency. Also, the integration of methodologies such as LH contribute to the sustainability of the healthcare system, ensuring a better experience for both patients and medical staff [16]. Finally, this study provides new insights into the application of LH integrated with I4.0 in medical areas, with a special focus on the optimisation of hospital processes. Based on the identified situation in hospital process management, this study poses the following research questions: i) How can LH improve capacity in the current healthcare system and hospital service efficiency; ii) How can simulation, as an I4.0 technology, improve human resource allocation for proper decision making; and iii) How can simulation, as an I4.0 technology, improve human resource allocation for proper decision making?
The rest of the article is structured as follows: section 2 presents a review of the relevant literature, providing the theoretical context and background of the study. Section 3 describes in detail the methodology adopted, including the procedures and tools used. Section 4 presents the results obtained, accompanied by their respective analysis and a discussion of the findings. Finally, section 5 offers the conclusions of the study, as well as possible lines of future research.
2. Theoretical background
2.1. The digital technologies of I4.0
I4.0 technologies have revolutionised industrial processes in traditional supply chains. So, raw material procurement, manufacturing and logistics are driven by the digitisation of business processes, for example, with the internet of things (IoT) [17]. IoT facilitates real-time monitoring of patients, equipment and supplies, improving decision-making and operational efficiency. Moreover, artificial intelligence (IA) plays a key role in analysing large volumes of data to forecast demands, optimise logistical routes and personalise patient care, improving responsiveness to unforeseen changes [17] Cybersecurity becomes a critical aspect to ensure the protection of clinical information and the digital infrastructure of hospitals. In this context, autonomous robots optimise repetitive and high-precision tasks, reducing the burden on healthcare staff. Newly, simulation is crucial in validating processes to reduce waste because it allows modelling and optimising workflows in virtual environments before they are implemented. Also, it improves agility in decision-making and response to variations in demand without affecting service quality, e.g., for healthcare systems[18]. In addition, big data and the integration of universal systems allow optimising hospital management, improving communication between devices and responsiveness to variations in demand. In this context, the capacity of the healthcare system is fundamental to efficiently manage resources and avoid BO and maintain service quality, especially in times of high demand. Here, correct decision making is supported by technologies such as simulation [9]. In particular, three decision levels can be distinguished in terms of the decision to be made in a given time frame: strategic, tactical and operational [19]. These decisions can be oriented towards minimising costs in the selection of production sites, storage and distribution of products or raw materials.
On the other hand, sustainability in resource management seeks not only efficient use, but also continuous improvement. In this sense, they highlight the importance of integrating quantitative models to optimise the management of inventories and resource flows [11]. This is approached from several perspectives: economic, optimising operational costs without affecting quality; environmental, minimising ecological impact by reducing resources and energy; and social, ensuring an accessible and quality service for all patients [20]. Here, cloud computing enables scalable storage and processing of medical data, improving information access and management. Additive manufacturing, through 3D printing, facilitates the customisation of prostheses and surgical tools, reducing costs and production times. Augmented reality and virtual reality improve medical training and procedure planning by providing accurate and interactive simulations [9].
In the context of simulation, this replicates a real process with sufficient fidelity to improve workflows. There are several types of simulation, such as discrete event simulation (DES), which models systems with changes at specific points in time [21], and continuous simulation, which uses equations to represent variables with constant changes. Other approaches include agent-based simulation (ABM), which models complex systems with autonomous interaction [21]. Monte Carlo simulation models uncertainty with random simulations, useful for risk analysis and economics. System dynamics (SD) studies the interaction of variables in non-linear systems, such as population growth. Optimisation simulation integrates simulation and optimisation techniques to improve complex processes [14]. Virtual simulation, which includes augmented and virtual reality, creates replicas of physical systems, useful for training and industrial simulation. Finally, stochastic Monte Carlo simulation explores systems with multiple random variables, using probabilistic methods [22].
In the clinical setting, simulation is essential for learning, recreating complex scenarios and evaluating performance in medical procedures [23]. Clinical simulation has proven to be essential in medical training, providing professionals with a controlled environment to deal with complex situations without the risks inherent in real practice. This improves decision-making, team coordination and quality of care [23]. In this context, FlexSim healthcare (FCH) is a specialised software for simulating the healthcare sector, offering advanced tools such as full-scale 3D visualisation and statistical analysis. Its use allows evaluating scenarios and optimising resources in environments with capacity constraints, such as the availability of beds, medical equipment and staff. This approach is essential to mitigate BO [18], where demand exceeds capacity, causing waiting times and reducing efficiency.
In environments of uncertainty, DES is suitable for optimising processes and improving the efficiency of the healthcare system by analysing and making decisions based on simulated data. This involves minimising waiting times, improving staff allocation and maximising medical equipment utilisation without compromising quality of care [18]. Also, simulation with deterministic demand plays a crucial role in operational planning and management. It is a demand that can be predicted with certainty, which facilitates optimal resource allocation [18]. However, when variability in medical care is high, such as in emergency units, uncertainty in demand creates additional challenges in maintaining efficient patient flow. From this perspective, projected demand is introduced, which refers to an advance estimate of the volume of medical care based on historical data and expected patterns. This type of demand allows for anticipating variations in the number of patients and optimising resource allocation, ensuring a more efficient response to fluctuations in demand [19].
The simulation process in FCH follows several sequential steps to ensure an efficient analysis of the system: (i) system analysis, where simulation objectives are defined and critical areas are identified; (ii) data collection, considering initial conditions and internal variables; (iii) system model building using flow diagrams or networks to represent discrete events; (iv) simulation model development, defining its structure and software platform; v) validation of the model, ensuring its accuracy through testing and verification; vi) running the simulation, observing how the system responds to different inputs; and vii) obtaining and analysing results to evaluate system behaviour and look for optimisation opportunities [24].
2.2. Lean healthcare
LH is a key methodology for optimising processes and is focused on reducing waste and continuously improving clinical outcomes, which reduces costs and improves the quality of care [25]. Its integration with simulation, using tools such as FCH, allows modelling and analysis of processes, facilitating decision-making to improve the efficiency and productivity of the healthcare system[12]. Within this approach, operational decisions seek to minimise waste and waiting time. Also, tactical decisions are aimed at improving the productivity of the services provided in relation to the resources used. This monitors system performance in terms of quality and quantity of care [18].
A key aspect of LH is the elimination of waste through LM tools adapted to the hospital environment. Among them, 5S encourages workspace organisation; value stream mapping (VSM) allows visualisation of the value stream to identify improvements; kanban optimises inventory management under the just-in-time (JIT) model; and poka-yoke introduces error-proofing mechanisms in medical and administrative procedures [26].
Other effective strategies include kaizen, based on continuous improvement, and heijunka, which balances workload to avoid saturation. In addition, single-minute exchange of die (SMED) reduces changeover times between procedures, and total productive maintenance (TPM) ensures preventive maintenance of medical equipment, improving its availability and reliability [26].
Within the framework of LM thinking, the identification and elimination of waste is crucial to improve operational efficiency. Traditionally, seven types of waste have been identified: overproduction, excessive inventory, unnecessary movements, waiting times, defects, overprocessing and inefficient transportation. However, in modern environments, especially in the hospital setting and within the I4.0 paradigm, three additional wastes have been added: underutilisation of human talent, which refers to the underutilisation of staff competencies and skills; poor information management, which leads to delays and errors in decision-making; and poor quality of inputs or suppliers, which affects operational continuity and patient safety [26].
Effective LH implementation depends not only on the application of tools and strategies, but also on human capital. Through continuous training and the incorporation of new professionals, the flexibility of the system to adapt to the changing demands of the clinical environment can be improved. Moreover, the flexibility and polyvalence of professionals allow for the optimisation of available resources, which favours the efficiency of the system in contexts with high variability of demand [27,28] .
In this sense, system overload occurs when the amount of care required exceeds the system's capacity to manage it effectively. This phenomenon can lead to saturation of resources, increasing waiting times and affecting the quality of services. Consequently, the correct identification of these critical points and the implementation of preventive measures are essential to maintain adequate flow of care and operational efficiency [29]. Also, at LH, quality is an essential component that is ensured through the recruitment of highly qualified staff. This approach ensures that care is delivered in a safe, efficient and patient-centred manner. Other strategies, such as process standardisation and the adoption of advanced technologies, are also critical to improving outcomes [16]. In that sense, the business challenge lies in balancing these strategies to optimise both diagnostics and treatments as well as the patient experience, minimising medical errors and improving clinical efficiency.
It is important that all staff are actively involved in identifying inefficiencies and proposing solutions. Here, continuous improvement (kaizen) provides effective strategies, such as constant feedback and training in best practices. While the incorporation of doctors and nurses can improve the flow of care and reduce waiting times, other approaches such as restructuring care processes and implementing flow management technologies can also be considered [28]. For that reason, any approach that allows for more efficient and faster care will be beneficial for the patient experience and hospital operations. Finally, the principle of workload levelling (heijunka) suggests that the equitable distribution of tasks is key to avoiding overload and maintaining optimal performance. Solutions such as reorganising shifts, adding more medical staff, implementing multifunctional teams and using scheduling tools can help to better balance demands and available resources [30].
3. Methodology
This study uses conceptual modelling to improve process performance by implementing I4.0 enabling technologies, specifically simulation [26]. Here, a quantitative and experimental approach is adopted to model hospital processes using FCH software. The design includes the creation of simulation models that represent the flow of patients from admission to discharge. Evaluation of key metrics (KPIs) considers all intermediate stages of care.
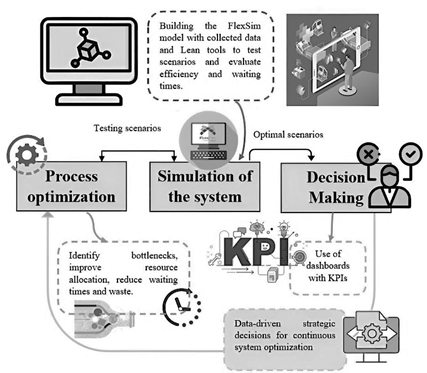
Regarding the implementation steps for LH and the details of the tools used, a conceptual framework for programming the simulation is presented in Fig. 1. First, data is collected and theoretical input calculations are performed for the simulation in Flexsim, i.e., performance measures, work-in-process inventories, and distributions of arrivals to each process. Next, the simulation model is constructed in the healthcare environment. Then, the experimental scenarios are tested to evaluate the impact of waiting time and efficiency. Here, the LM tools are incorporated. In the next step, scenarios are chosen for decision-making that eliminate waste, optimisation of processes, and the promotion of a culture of continuous improvement in the organisation. Finally, these scenarios are evaluated considering KPIs to optimise resource allocation and system efficiency, facilitating strategic decision-making.
Data collection includes process times, care flows and resource utilisation. Interviews with medical staff, direct observations and review of hospital records are used. In this sense, the analysis of available data on the system to be simulated is a key task that must be carried out rigorously, as it simplifies and optimises the process of developing simulation models. So, the relevant information is identified, based on the objectives defined in the project. For the collection of data needed for the simulation, the care flows present for patients are studied in order to obtain key information for modelling and analysis.
Table 1. shows the analysis of the activity times of the medical staff, in order to identify the BOs in the process.
Table 1 Standard time for each process.
| Process | Time (minutes) |
|---|---|
| Patient reception and initial evaluation Diagnostics Medical consultation | 56.45 70.45 71.43 |
| Tests and operation | 108.75 |
Source: Own elaboration.
To determine the arrival distributions for each process, the FCH ExperFit tool is used. This tool automatically and accurately generates a probability distribution that optimally represents a data set for the modelling and analysis of the simulated processes. Table 2 presents the fitted probability distributions for the different model parameters.
Table 2 Probability distribution of each process, from FCH
| Process | Distribution |
|---|---|
| Registration and transport | beta (41.451096, 112.979605, 37.523096, 33.290444, <stream>) |
| Transport to waiting room | beta (18.931491, 54.113646, 29.936199, 34.615791, <stream>) |
| Transport to emergency room | loglogistic (0.001362, 41.976442, 23.821625, <stream>) opc 2 |
| Triaje | beta (3.294162, 1551.812034, 17.804659, 17.883504, <stream>) |
| Transfer to observation room | beta (15.518288, 73.273535, 53.957810, 51.952136, <stream>) |
| Emergency medical examination | weibull (1490.952979, 11.667304, 3.946799, <stream>) no |
| Emergency medical consultation | beta (525.319578, 659.245646, 31.778915, 25.224985, <stream>) |
| Location in the emergency operating room | lognormal2(0.000000, 300.004653, 0.009302, <stream>) |
| Emergency surgery | beta (3586.995716, 3609.383641, 67.328649, 40.671087, <stream>) |
| Emergency recovery room location | beta (276.598245, 316.566239, 40.216633, 22.607272, <stream>) opc2 |
| Emergency patient exit | loglogistic (31.375206, 29.979410, 23.047032, <stream>) |
| Weighing in the balance | Johnson bounded (97.216798, 148.054684, -0.222860, 2.926063, <stream>) |
| Location in a hospital bed | beta (2.537234, 67.841892, 48.279582, 44.009175, <stream>) |
| Medical examination | beta (1639.514543, 1921.928166, 44.802877, 32.603515, <stream>) |
| Electrocardiogram | lognormal2(0.000000, 659.182762, 0.013292, <stream>) |
| X-rays | lognormal2(0.000000, 1501.033324, 0.003534, <stream>) |
| General consultation | johnsonbounded (574.469277, 632.364177, 1.032101, 4.300052, <stream>) |
| Patient exit | beta (41.853312, 69.975457, 42.834650, 38.970669, <stream>) |
Source: Own elaboration.
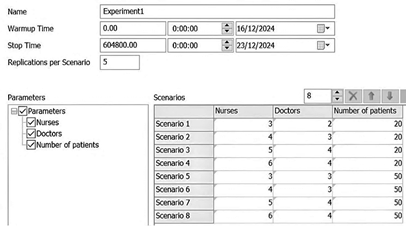
In terms of scenario analysis, strategies proposed by the LH methodology are used to evaluate the impact of adding more medical and nursing staff in a hospital setting. So, the initial conditions are evaluated against the experiments. The simulation time corresponds to a week of 604,800 seconds (sec). These scenarios include variations in the number of patients, the availability of resources and the organisation of the workflow, allowing to evaluate how they affect the demand, the redistribution of resources and the implementation of operational improvements. Thus, eight scenarios are modelled in FCH with DES to analyse patient flow and resource allocation.
Table 3 presents the design of experiments with details of each scenario, highlighting the simulation conditions and key differences between them. This allows to assess the impact of each strategy on hospital capacity and system sustainability.
Table 3 Design of experiments
| Scenario Code | Description | Increase in staff | Demand |
|---|---|---|---|
| E1 | Base Condition (actual situation) | ++ | DI |
| E2 | Increased demand | XO | DI |
| E3 | Minimal staff expansion | XO | DI |
| E4 | Moderate expansion of staff | XO | DI |
| E5 | Exclusive increase of doctors | +O | DA |
| E6 | Increase in nurses and doctors | XO | DA |
| E7 | Maximum expansion of staff | XO | DA |
| E8 | Optimised staff expansion | XO | DA |
Note: ++ initial number of staff XO increase in nurses and doctors +O increase in doctors only DI initial patient demands DA increase in patient demand.
Source: Own elaboration.
4. Results
4.1. Integral evaluation of production processes under initial conditions
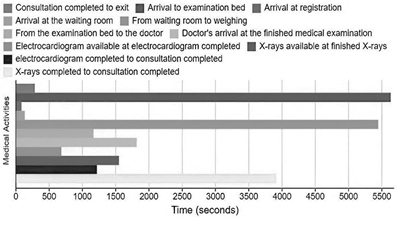
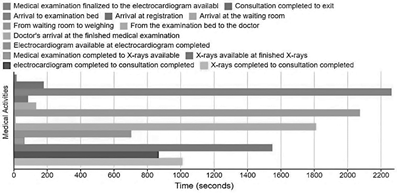
To perform the analysis of times, throughput and resources under initial conditions. Fig. 2 presents the transit times of patients in different areas of the clinic. Administrative phases, such as patient registration (82.39 sec) and discharge (283.07 sec), show efficient times, indicating adequate management at these stages. However, significant delays were identified in the clinical stages. Waiting time for weighing in general consultation reaches an average of 5444.63 sec, and waiting time in the examination room until the arrival of the doctor is 1165.34 sec, suggesting BO in patient management and the availability of medical resources. As for diagnostic procedures, electrocardiogram takes 682.37 sec, while X-ray takes 1547.15 sec. In addition, the total X-ray process (3906 sec) is considerably longer than electrocardiogram (1216.85 sec), which could be attributed to equipment availability, logistics or complexity of the procedure.
Source: Own elaboration.
Figure 2 General consultation time intervals under initial conditions, from FCH
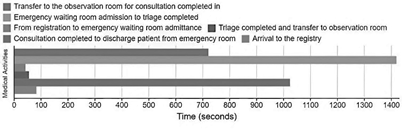
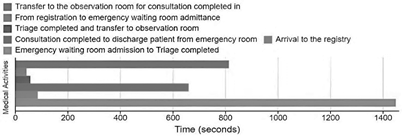
Fig. 3 details the times recorded in the emergency area, where both strengths and opportunities for improvement in care management are identified. Initial activities show an efficient flow: patient registration is completed in 82.39 sec, followed by admission to the waiting room (41.81 sec), which evidences a quick incorporation of patients into the system. In contrast, triage represents a critical point, with an average duration of 1418.44 sec. This delay can be attributed to the detailed assessment of patients or to BO in the availability of specialized staff and infrastructure.
Source: Own elaboration.
Figure 3 Emergency consultation time intervals under initial conditions, from FHC
Given its impact on the allocation of care, it is recommended that resources be optimized to reduce these times. The transfer to the observation rooms is agile, with an average of 54.57 sec, reflecting adequate logistics. Emergency medical consultation has an average duration of 720 sec, considered to be in accordance with the complexity of the cases attended. Consequently, patient discharge requires 1024.17 sec, time associated with final evaluations, documentation and coordination of transfers. Optimizing these processes would reduce delays in discharge and speed up the availability of resources for new admissions.
Finally, the findings highlight how simulation can provide key information to improve the allocation of human resources. By identifying critical areas, informed decisions can be made to optimise patient flow and minimise waiting times, which contributes to increased operability.
Regarding to BOs, in general practices the weighing of patients represents a BO due to the availability of only one scale, which slows down the flow of care. In emergencies, triage is also a BO, whose improvement could be achieved with more assessment stations to increase the capacity of the process. Also, the availability of a single operating theatre limits surgical capacity, suggesting the need for a second theatre to meet demand more efficiently. These improvements optimise resource utilisation and strengthen the economic sustainability of the system by maximising the use of existing infrastructure without compromising service quality. In conclusion, the simulation by managing the identified BOs facilitates tactical and operational decisions on how best to allocate staff. This ensures an efficient response in areas such as weighing or triage, improving care and reducing delays.
In terms of resource use, Fig. 4 shows the X-ray utilization for one week, with a total of 25 patients seen, reflecting the demand for this specific procedure. In addition, Fig. 5 shows the use of the wheelchair for the transfer of 50 patients, indicating that, although the patient flow is considerable, it is not high enough to require the use of other equipment or transfer methods. This suggests that transfer resources and diagnostic procedures are being used appropriately according to projected demand, without generating BO in these aspects of the flow of care.


Based on the staff available under initial conditions, the maximum care capacity is determined to be 137 patients, as shown in Fig. 6. This limit is due to the identified BOs and the restricted availability of resources, which directly impacts on the efficiency of the care system.
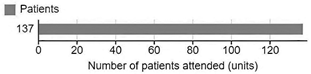
Fig. 7 presents a scorecard with various KPIs illustrating staff utilisation in the clinic. It shows that general practitioners have the highest percentage of utilisation, while nurses in this area have a lower workload, as health technicians are in charge of examinations. In the emergency area, nurses have a higher workload, participating in surgeries, while surgeons are more free. This distribution of tasks highlights the differences in staff responsibilities according to the type of medical care, suggesting the need for an adequate allocation of human resources to improve operational efficiency in both areas.
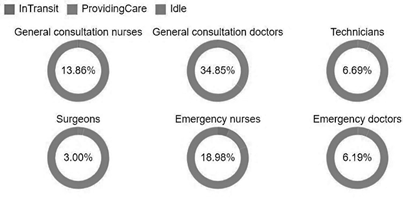
Fig. 7 also shows staff utilisation in the medical system, revealing a significant proportion of inactivity (Idle) in all roles, suggesting opportunities for optimisation in task allocation. On the one hand, general practice doctors spend the most time on direct care, with 34.85%, followed by emergency nurses (18.98%) and general practice nurses (13.86%). On the other hand, technicians (6.69%), emergency doctors (6.19%) and surgeons (3.00%) have a lower participation in direct care, which is in line with the specialised nature of their functions. The category ‘InTransit’ (on the move) has a low incidence.
4.2. Experimentation of production processes with LH
For the execution of the experiments shown in Table 3, different scenarios were configured using LH principles in order to optimise human and operational resources. Through the DES performed with the FCH software, the flow of medical care is modelled. This approach, based on accurate data, facilitates tactical and operational decision making to improve the efficiency of the system in the short and medium term.
In Fig. 8, it is evident that, despite maintaining efficient times in processes such as patient registration (84.68 sec) and discharge (178.86 sec), significant delays were identified in the weighing in general consultation (2073.77 sec) and waiting in the examination room (2262.24 sec), suggesting the presence of wasted waiting time. To mitigate these delays, LM tools such as heijunka, which helps to level the workload and avoid unnecessary backlogs, and VSM, which allows visualising the flow of care and identifying optimisation opportunities, can be applied. In contrast, electrocardiogram (702.95 sec) and x-ray (1548.76 sec) procedures were managed efficiently, but the total consultation time for x-ray (1008.66 sec) exceeds that for electrocardiogram (867.75 sec), which could be related to logistical or complexity differences.
In Fig. 9, the times recorded in emergencies reveal efficient management of registration (84.68 sec) and admission to the waiting room (41.84 sec). However, triage (1448.12 sec) remains a BO, suggesting the need for optimisation in this process. Transfer to observation rooms is fast (56.75 sec) and emergency medical consultation (659.01 sec) remains within an adequate range. Discharge time (812.51 sec) also presents an opportunity for improvement in the discharge process.
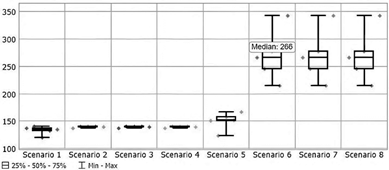
The simulation results show how different scenarios impact system capacity and demand. Fig. 10 presents different scenarios: standard operation with 20 patients per day, increasing staff (nurses and doctors) and increasing demand to 50 patients per day without changing the amount of resources.
In terms of system throughput, when the number of patients is maintained at 20 per day, the capacity of care varies between 120 and 140 patients per week in Scenario 1 (E1). In this initial scenario, the system throughput reaches 40.8%. In Scenarios E2, E3 and E4, where minimal or moderate expansion of staffing is implemented, capacity is maintained at a median of 139 patients. This indicates that these adjustments do not have a significant impact on operational efficiency. Consequently, when demand increases to 50 patients per day, E5 where only the number of doctors is increased shows a slight improvement. This suggests that the availability of doctors is not the only limiting factor in the system, but that other resources such as support staff and hospital infrastructure also play a role.
Fig. 11 shows that in the best-case scenario (E6), a significant improvement in the capacity of care is observed, along with a reduction in BO. From this scenario onwards, BO constraints are kept under control in subsequent scenarios, contributing to greater stability in system performance. With a simultaneous expansion of doctors and nurses, the system reaches a minimum of 214 patients seen weekly, with an average of 266 representing a throughput of 77.6% and a maximum of 343, at this being the total possible capacity, the throughput reaches 100%. This increase reflects a significant improvement of 36.8% in operational efficiency, highlighting the positive impact of resource optimisation and staff expansion on hospital capacity. Thus, the results highlight the importance of balanced staff growth in optimising hospital care, far exceeding the efficiency achieved in scenarios with partial expansions.
By taking advantage of E6 to reach the maximum number of patients, it is revealed that the system manages to serve an average of 266 patients weekly, as illustrated in Fig. 12. Thus, applying LM tools, such as kaizen, through continuous improvement and staff feedback, would allow detecting and correcting inefficiencies to further increase the capacity of the system.
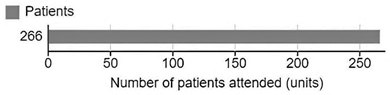
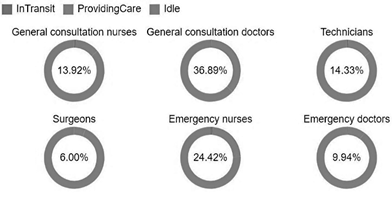
Fig. 13 presents staff utilisation as a function of E6. Here, there is a slight increase in the utilisation of general practitioners from 34.85% to 36.89%. Also, technicians experience a significant increase from 6.69% to 14.33%, and the utilisation of surgeons doubles. In addition, it is noted that physicians, technicians and surgeons all increase their time spent on direct care. In conclusion, there is an increase in staff utilisation due to the increase in the number of patients. Consequently, in the emergency area, nurses increase their share from 18.98% to 24.42%, while doctors increase from 6.19% to 9.94%. However, although some roles still show Idle, these changes reflect a better distribution of time towards direct care. Finally, it is identified that the use of LM tools such as heijunka can optimise load levelling, reducing these unproductive times and improving team performance.
Finally, Fig. 14 and 15 show the use of X-rays and wheelchairs, serving 52 and 104 patients respectively. This indicates a moderate workload that allows for efficient management of resources without generating excessive pressure.


4.3. Discussion of results
Analysis of the simulation results highlights the importance of optimising resources within the healthcare system. BO is identified in the process of weighing patients during general consultation and triage in emergencies, which has a negative impact on operational efficiency. In addition, it is observed that the addition of four nurses and three doctors significantly improves the capacity of care, increasing the number of patients seen weekly. In E6, the number of patients seen increases from a range of 157-166 in the initial conditions to a range of 214-343, reaching the maximum capacity of the system. This finding is in line with previous studies [31], where improved staff allocation results in an optimisation of resources and care times in an emergency hospital. Additionally, the results indicate that the efficient use of resources such as X-rays and wheelchairs avoids overloading the system. This is in line with other proposals [32], where the appropriate allocation of equipment and resources improves not only efficiency, but also the quality of service.
To further reduce waiting times and improve patient flow, we recommend applying the kaizen continuous improvement approach, implementing more weighing and triage stations, as well as the construction of a second operating theatre. Our simulation results are supported by other authors [33], who demonstrate how resource optimisation through simulation contributes to maintaining efficient flow in high-demand situations, such as health emergencies.
Implementing the recommendations derived from simulation not only reduces BO, but also optimises hospital operations, improving the allocation of staff and resources for more efficient care. This approach is especially relevant for economic sustainability, because increasing the capacity of care while reducing time wastage has a positive impact on KPIs, such as the system's profit to strengthen its long-term sustainability. In this sense, it reinforces the idea that appropriate resource allocation and improved operational efficiency not only reduce costs, but also contribute to economic stability and quality of care [34].
5. Conclusions
This study demonstrates that the combination of LH and DES can optimise efficiency and improve the allocation of hospital resources. Reducing wasteful waiting times, increasing care capacity and providing system sustainability are critical aspects of success. This answers the research questions posed in this article.
How can LH improve the capacity in the current healthcare system and the efficiency of the hospital service? LH optimises hospital capacity by reducing operational waste, such as excessive waiting times and overloading of staff on certain shifts. LM tools such as VSM allow for the detection of BO in care flows, while kaizen drives continuous improvement in critical processes such as patient weighing, triage and surgeries. In addition, the application of heijunka, which focuses on workload levelling, allows balancing hospital demand, avoiding peaks of saturation and staff downtime. This optimises the availability of doctors and nurses without generating additional costs. The methodology applied through experimentation has been shown to reduce waiting times by 35% and increase operational efficiency by up to 36.8%. Consequently, these results show that strategic staff redeployment based on LM principles increases capacity to meet up to 77.6% of projected demand without compromising service quality. This is in line with theoretical studies concerning the impact on the sustainability of the hospital system [10]. Thus, the requirements associated with these improvements include the integration of digital and operational systems, the standardisation of processes, and alignment with healthcare performance indicators, such as monitoring response times, analysing patient flow, and allocating resources in real time, to ensure sustainable improvements in efficiency.
How can simulation, as an I4.0 technology, improve the allocation of human resources for appropriate decision-making? DES, as a key tool of I4.0, enables the evaluation of different care scenarios and optimisation of human resource allocation based on actual demand. Its application facilitates the identification of BO and the dynamic redistribution of staff, ensuring that the workload is efficient and equitable in each shift. From an economic and social perspective, the simulation allows decisions to be made based on key KPIs, such as capacity, waiting times and profit. This ensures a more efficient response to variations in demand. In this study, our results show that the combination of simulation and LH to reduce waste achieves optimal resource allocation in care systems. At the tactical level, simulation allows planning medium-term staffing strategies, optimising the number of doctors and nurses needed according to the expected workload. At the operational level, DES enables immediate adjustments in staff deployment based on real-time demand, ensuring that resources are used efficiently, and service quality is maintained. This study confirms that the combination of LH and DES is an effective strategy to optimise hospital efficiency, improving decision-making at different levels.
This study has several limitations. First, the data used in the simulation are restricted to operational decisions within a specific hospital, which may restrict the ability to generalize the results to other hospitals with different characteristics, such as size, infrastructure, or type of patients.Furthermore, the model has focused exclusively on maximizing operational efficiency, without considering additional factors that could affect system performance, such as administrative processes, which are crucial for overall efficiency. For future research, it is recommended to integrate IA to optimize resource allocation in an adaptive way. IA would allow adjusting resources in real time, improving the flexibility of the system in the face of fluctuations in demand. Furthermore, it would be relevant to extend the model to different hospital contexts, evaluating hospitals with different characteristics to test the applicability and robustness of the model in different settings. It is also suggested to investigate the impact of the digitalization of administrative processes, as the automation of these processes could reduce waiting times, improve resource allocation and, in general, optimize the efficiency of the health system.

