











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Over the years, the percentage of people living with mental disorders has increased to 25% worldwide, with 450 million people being affected by mental and behavioral disorders.1 In the primary care setting, the prevalence rate of mental disorders or psychiatric symptoms may reach 51.1%:2-4 this suggests the need for proper training and specific support among general practitioners in order to manage mentally ill patients.
Given the need to redirect the mental health care model in Brazil, which was based in psychiatric hospitals and in order to protect and guarantee the rights of people with mental dis orders, Law No. 10,216 from 2001 was instituted, the so-called "Psychiatric Reform Law", which motivated the institutionalization of Psychosocial Care Centers (CAPS), whose purpose is to prioritize care for patients with moderate to severe men tal disorders without their hospitalization. Mild mental health disorders are referred to the primary care setting composed of basic health units, whereas severe mental disorders are treated at mental health services. (5
During their educational course as general practitioners, medical students are trained in each field of medicine, includ ing psychiatry. In addition, according to the Epidemiologic Catchment Area Study (ECA) (6 in the United States, 40 to 60% of mental health disorders are regularly managed by general practitioners.
In Brazil, medical students' curricula are poorly based on mental health/psychiatry, and most of the information is theoretical, with no proper practical internships. (7 Consequently, medical doctors working in primary care may not have ade quate training to manage mental health disorders. (7
The issues that primary care doctors face when managing mental disorders are mostly due to inadequate training. It is consequential that many patients are not properly treated or followed, which may lead to an increase in cases accessing the psychiatry emergency rooms. (8
Although general practitioners working at São Bernardo do Campo's basic health units and in the rest of the country are locally supported by mental health specialized staff, they daily cope with a remarkable number of mentally ill patients and may not guarantee a quality treatment to them. (9
The main goal of this research was to investigate the issues presented by general practitioners in managing mental health disorders at basic health units in the city of São Bernardo do Campo (São Paulo), as well as to evaluate the best train ing method and the percentage of interest and adhesion by these professionals. This research would be the start-point to successfully and punctually plan a set of interventions for improving mental health care in the primary care setting.
Methods
A descriptive study was conducted, from primary and secondary sources, presenting qualitative and quantitative results.
A total of 153 general practitioners (GP) working at the 34 basic health units (BHU) in the city of São Bernardo do Campo were enrolled, distributed in 9 territories (T), with T1 embrac ing Taboão, Paulicéia and Jordanópolis' BHUs; T2 embracing Rudge Ramos, Vila Dayse, Caminho do Mar and Planalto's BHUs; T3 embracing São Pedro, Parque São Bernardo and Farina's BHUs; T4 embracing Vila Euclides, Santa Terezinha and Baeta Neves' BHUs; T5 embracing Ferrazópilis, Silvina, Selecta, Leblon and Montanhão's BHUs; T6 embracing Alves Dias, Vila Nazareth, Vila Rosa and Vila Marchi's BSUs; T7 embracing Ipê, Orquídeas, Oliveiras, União and Alvarenga's BHUs; T8 embracing Demarchi, Batistini and Represa's BHUs, and T9 embracing Riacho Grande, Fincos, Areião and Santa Cruz's BHUs. The distribution of GP and psychiatrists can be seen in supplementary Table 1.
The city is divided into rural (T9), urban (T1-4), and tran sition areas (T5-8). T7-9 have the lowest per capita income of the city, T7 and T8 are the most contemplated by Bolsa Familia (a governmental social program to families with no income), T9 despite sharing a similar developmental level, have a low populational density. (10
A simple multiple-choice questionnaire was formulated from the merger of 2 questionnaires presented in highly regarded studies conducted in London and Portugal, (10,11 translated by Google Translator without any alteration and then applied from August to December of 2020 to identify the difficulties presented by GPs when managing mental health disorders.
The studied variables were assessed through multiple-choice questions, including the following: demographic data, information on the difficulties reported when approaching psychiatric outpatients, on the preferred modalities of being trained in mental health, on the expectations regarding better exchanges between psychiatrists and general practi tioners, among other variables. All questions were multiple choice.
All the questionnaires, alongside a written and informed consent of the participants, were personally delivered by the researchers to the managers of each BHU to reach a good num ber of questionnaire-fillings by the target population and were collected by the researchers after 30 days. As inclusion cri teria, we utilized any returned questionnaire that was fully answered after 30 days.
The computation and analysis of collected data were con ducted using the Statistical Package for the Social Sciences (SPSS) version 15.0.
The research has been previously approved by the Munic ipal University Hospital, from São Bernardo do Campo, Scientific Research Project Evaluation Staff, since human beings were involved in the study, as well as by the City Health Care and Care Management Department, and addition ally approved through the Plataforma Brasil by the Research Ethics Committee of São Paulo's Health Secretariat, with the following registration number: 4.167.865.
Results
A total of 153 questionnaires were delivered to GPs at the BHUs, with a response rate of 61.4% (94/153).
Among São Bernardo do Campo's 9 territories, T9, including Riacho Grande, Fincos, and Areião's BHUs, was excluded due to logistics and poor local accessibility. All other 8 territories with 30 BHUs were included.
The rate of answering ranged: T1 (10.6%); T2 (8.5%); T3(6.4%); T4 (10.6%); T5 (14.9%); T6 (10.6%); T7 (24.5%), and T8(13.8%).
The analysis of demographical data regarding GPs working at BHUs from São Bernardo do Campo has shown that there is a predominance of female physicians (64.9%), mostly aged23-29 years old (47.9%), with 68.1% working as GP for less than5 years (supplementary Table 2).
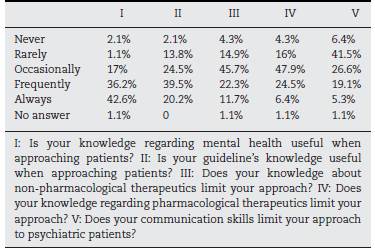
Table 1 shows GPs’ report that knowledge regarding mental health and guidelines are both significantly helpful in managing mental disorders. However, 22.3 and 25.5% frequently have their approach limited by their knowledge about non-pharmacological therapeutics and pharmacological therapeutics, respectively.
Table 1 Percentage distribution of general practitioners’ experience in approaching patients with mental health disorders according to their mental health knowledge.
GPs’ main difficulties in mental health were collected as shown in Table 2. They ranked: psychiatric emergencies (44.7%), alcohol and drug dependence (35.1%), psychotropic medications prescription (29.9%), and the evaluation of suicide risk (27.6%).
Table 2 Percentage distribution of the 3 main difficulties of each interviewed general practitioner when managing patients with mental health disorders
| Difficulties | Option 1 (%) | Option 2 (%) | Option 3 (%) | Total (%) |
|---|---|---|---|---|
| Psychiatric emergencies | 44.7 | 0 | 0 | 44.7 |
| Panic disorder | 4.3 | 3.2 | 0 | 7.5 |
| Dementia | 9.6 | 11.7 | 1.1 | 22.4 |
| Cognitive therapy | 9.6 | 4.3 | 1.1 | 15 |
| Adolescent problems | 2.1 | 4.3 | 0 | 6.4 |
| Evatuion of suicide risk | 8.5 | 13.8 | 5.3 | 27.6 |
| Alcohol and drugs' dependence | 8.5 | 20.2 | 6.4 | 35.1 |
| Childhood problems | 2.1 | 7.4 | 7.4 | 16.9 |
| Family and marital problems | 3.2 | 3.2 | 3.2 | 9.6 |
| Eating disorders | 0 | 5.3 | 2.1 | 7.4 |
| Psychotropic prescription | 4.3 | 9.6 | 16 | 29.9 |
| Mental health promotion | 1.1 | 1.1 | 1.1 | 3.3 |
| Somatization | 1.1 | 1.1 | 7. | 9.6 |
| Psychosexual problems | 0 | 4.3 | 5.3 | 9.6 |
| Anxiety disorders | 0 | 0 | 2.1 | 2.1 |
| Depression | 0 | 0 | 2.1 | 2.1 |
| Chronic mental disorders | 0 | 5.3 | 11.7 | 17 |
| Acute reaction to stress | 0 | 2.1 | 0 | 2.1 |
| Tiredness | 0 | 0 | 0 | 0 |
| Sleep problems | 0 | 1.1 | 7.4 | 8.5 |
| Behavioral therapy | 0 | 1.1 | 8.5 | 9.6 |
| ICD-10 classification | 0 | 0 | 4.3 | 4.3 |
| Mourning | 0 | 0 | 3.2 | 3.2 |
| No answer | 1.1 | 1.1 | 4.3 | 6.5 |
Also, 33% of GPs were unaware of the existence of referral criteria to psychiatric services as well as 54.3% of the BHUs reported not having any psychiatrist in their medical staff, as shown in Table 3. Besides this, 94.7% of the interviewed individuals reported the will to improve the interaction between GPs and psychiatrists from the Family Health Support Nucleus (best known in Brazil as NASF: Núcleo Ampliado de Saúde da Família).
Table 3 Sample distribution regarding knowledge about referral criteria, desire of a better interaction between general practitioners and NASF’s psychiatrists, presence of psychiatrists working at BHUs and interest in participating in trainings regarding mental health knowledge enhancement (N=94).
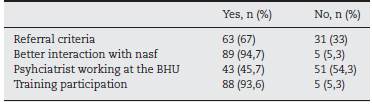
In addition, 93.6% of GPs showed interest in mental health training through small group meetings (27.7%) or case discussions (27.7%) as well as lectures (24.5%) or video lessons (1.1%).However, 5.3% of GPs (5/94) reported no interest in mental health training, mostly aged 50-60 years old.
BHUs not reporting any psychiatrist in their medical staff have shown more issues in mental health, such as dementia, in particular, 31.4% of GPs working without a psychiatrist versus 11.6% of those working with a psychiatrist; childhood psychiatry issues were higher as well: 25.4% without a psychiatrist versus 5.9% with a psychiatrist.
Lastly, in T7 and T8, located in the city suburbs, difficulties related to alcohol and drug dependence were higher, as reported by 8 doctors (34.8%) from T7 and T9 doctors (69.2%) of T8.
Discussion
GPs working in BHUs are responsible for follow-up psychiatric patients classified as low-complexity cases. However, these units may be overloaded and have poor network support, including mental health services. (13
In this research, we reported on the issues of GPs working at BHU in the city of São Bernardo do Campo in managing mental disorders in order to provide a set of data for the improvement of mental health interventions in the primary care setting.
As reported, most of GPs aged between 23 and 29 years old (47.9%) and 30 and 39 years old (24.5%) and 68.1% of doc tors had been working for <5 years in primary care. A study conducted in São Paulo13 showed that 75% of doctors who graduated in 5 years or less reported salary motivation and difficulties in entering medical residencies programs as the reason for working in primary care. Furthermore, 45% of the GPs did not have previous experiences of working in BHUs. (14
Knowledge regarding mental health may help GPs when approaching psychiatric patients, as well as the presence of specific guidelines or communication techniques. Compara tively, a study conducted in Portugal11 reported a significant difference in managing mental disorders based on the knowl edge (or not) of pharmacological and non-pharmacological interventions.
Regarding the main issues in managing mental disorders in São Bernardo do Campo, we found them ranking: psy chiatry emergencies (44.7%), alcohol and drugs' dependence (35.1%), psychotropic medications' prescription (29.9%), and evaluation of suicide risk (27.6%). Similarly, an English study10 reported a higher rate of difficulties among GPs related to the management of psychiatric emergencies, somatization disor ders, and psychotropic medications prescription. On the other hand, issues related to somatization in our study reported a low prevalence rate (9.6%). 54.3% of BHUs reported not having any psychiatrist in their medical staff, which led to more spe cific difficulties in managing dementia and childhood issues. This evidence may suggest that the possibility of acting in primary care with the support of a psychiatrist may be an important strategy of management. (15
In 2011, the Psychosocial Attention Network (best known in Brazil by the acronym RAPS) (15 was instituted as one of the net works in Brazil's Unique Health System (best known in Brazil by the acronym SUS) for people suffering from mental health disorders or drug abuse. It is constituted by 7 levels of atten tion: basic; specialized psychosocial; urgency and emergency; transient residential; hospital; deinstitutionalization strate gies, and psychosocial rehabilitation strategies. These levels are covered by specialized services, such as the psychosocial attention centers for people with mental health disorders (best known in Brazil by the acronym CAPS), for children and ado lescents (best known in Brazil by the acronym CAPSi), and for alcohol and drug users (best known in Brazil by the acronym CAPS-AD), hospital beds for hospitalization in general hospi tals, as well as primary care and community-based services, such as BHUs, family health strategy (best known in Brazil by the acronym ESF) teams, NASF, street offices (best known in Brazil by the acronym CR), among others, (16 due to particular ity of our mental health system it is not possible to compare with systems that are still based in psychiatric hospitals. The support network is adequate, but a high percentage of GPs do not know specific referral criteria to specialized services (33% in this study) as confirmed by a Portuguese study, in which 49% of GPs were unaware of such criteria. (12
As shown in Figure 1, São Bernardo do Campo is a city hold ing a complete RAPS, with units mostly situated in the central region. T7 and T8, located on the city outskirts, report more alcohol and drug dependence difficulties as reported by GPs from T7 (34.8%) and T8 (69.2%). The literature has reported that many people with drug-related disorders seek help in pri mary care units. (17 Thus, community-based services, such as the BHUs, are crucial for any care on the territory, (16,18 and it is extremely important to establish referral and counter-referral criteria within the SUS.
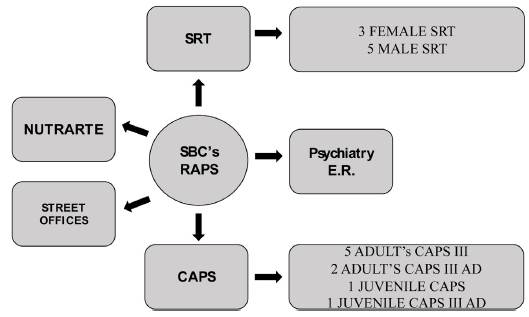
Figure 1 Psychosocial Attention Network (RAPS) in São Bernardo do Campo (SBC). CAPS: psychosocial attention center; NUTRARTE: Work and Art Nucleus; SRT: Therapeutic Residential Service. Elaborated from data gathered from SBC’s city hall website, available at: https://www.saobernardo.sp.gov.br/saude-mental. (17.
Among professionals working in primary care, there may be some difficulties in caring for patients with mental health disorders since academic backgrounds are incomplete. But, beyond that, ESF's workload includes a remarkable number of psychiatric cases to be managed. (5
Education in mental health must occur longitudinally, and primary care units should be connected to psychiatric services in a tighter way. (5
NASF guidelines indicate a co-responsibility among ser vices in following mentally ill patients even if work conditions for NASF's psychiatrist are often precarious, especially due to the lack of time to dedicate to ESF, since the matrix support of 20 teams is the maximum number of teams to be covered by a NASF, according to Ordinance n.154, from 20 08. (19,20 In this study, 94.7% of GPs would like a better interaction with matrix psychiatrists from NASF, as previously reported in the Por tuguese study11, in which 93% of GPs reported the same unmet need. 93.6% of the participants required a more focused educa tion on mental health: interactive and longitudinal programs with the opportunity to practice skills and acquire knowledge are considered to be more efficient. (21
In particular, in our research, 27.7% of participants pre ferred small-group reunions, 27.7% preferred case-simulation, 24,5% preferred lectures, 19.1% preferred orientation work shops, and only 1.1% preferred video lessons. These results are compatible with other studies that identified problem-based learning and small-group interactions as a more efficient intervention when compared to the traditional teaching methods. (15
Lastly, strategies that stimulate interest in mental health among GPs, above all older doctors, are crucial in order to improve attitudes and skills, (21 with a consequent improve ment of mental health treatments delivered in the BHUs.

