











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
As we begin this article, it is important for the lead author to share and express how the idea to write it emerged. This idea originated from a personal and anecdotal experience in which his father told him about his own education and training in the art of performing a physical exam, or semiol ogy, in the 1950s at Universidad Nacional de Colombia in Bogotá; his attendance at the 2023 regional internal medicine congress and the subsequent conversation between the main author and the authors (from yesterday and today) regarding the impact of point-of-care ultrasound on medical training and practice. The anecdote mentioned above describes the extraordinary physical exam skills of the semiology pro fessor and subsequent father of Colombian cardiology, Dr. Ramón Atalaya Varela 1,2. His students referred to him as someone who was able to "hear grass grow," which was not a joke, but rather an acknowledgement of his exceptional abil ity to auscultate his patients' hearts. What exactly were his students referring to? Well, using only his senses and inter preting what he heard, he was able to describe and diagnose patients' heart problems, foregoing the need to perform an echocardiogram, as is common in current medical practice.
Four decades later, the lead author had the privilege of witnessing the "magic," watching his professor, Dr. Jorge Gómez, at Hospital Mario Correo Rengifo, applying the classic technique of cardiac auscultation on a patient. He described the anomalous heart findings in detail which, to everyone's surprise, coincided with the echocardiogram findings that the same professor ordered after performing the physical exam.
Throughout the history of medicine, physicians have largely depended on skills like taking a proper complete medical history, observing carefully, performing a comprehensive physical exam, and using their senses and clinical reasoning or common sense. These skills are essential for diagnosing and treating patients properly. The clinical history plays an essential role in medical assessment, as it provides information about the symptoms, medical his tory, risk factors and other relevant details that can help the physician determine an accurate diagnosis. The ability to listen carefully to the patient, show empathy, ask pertinent questions and accurately understand the clinical findings is crucial for achieving the correct diagnostic aim. The clinical history also guides the aspects to look for during the physical exam, and helps make decisions about which complementary, biochemical and imaging, exams to or der, if necessary. It is important to emphasize that taking a proper clinical history may weigh significantly in the clinical diagnostic process 3-7 (Table 1).
Table 1 The percentage contribution of the clinical history, physical exam and laboratory tests to the diagnosis.
| Author | Year | Clinical his tory (%) | Physical exam (%) | Laboratory tests |
|---|---|---|---|---|
| Sandler et al. | 1980 | 56 | 17 | - |
| Hampton et al. | 1975 | 82.5 | 8.75 | 8.75 |
| Peterson et al. | 1992 | 76 | 12 | 11 |
| Roshan et al. | 2000 | 78.6 | 8.2 | 13.2 |
From another perspective, the physical exam contributes appropriately to the diagnosis, entailing a calm and detailed assessment following the art inherited from French medical practice and other schools, in the proper assessment of patients and their organs, following the classic sequence of inspection, palpation, percussion and auscultation. However, this art, or lost art, has declined in the amount of teaching time and depth provided in medical schools, which has led to its increasingly infrequent use in daily practice 8-12. The influence of technology has also contributed to this tendency, as it has become common to depend more on complementary medical exams and diagnostic tests rather than performing an exhaustive physical exam.
Reflection
Through these classic techniques used in the physical exam, physicians can identify relevant physical signs, like the presence of masses, skin changes, and abnormal body sounds, among others. A proper physical exam can provide important information for the patients' diagnosis and follow-up and guide the ordering of complementary biochemical or imaging tests. In addition to these technical skills, physicians also depend on their common sense and clinical experience to make appropriate decisions. Common sense involves the ability to reason logically, apply medical knowledge and consider different diagnostic possibilities. Clinical experience accumulated over the years also plays a crucial role, as physi cians learn to recognize patterns, interpret findings and make decisions based on similar clinical situations they have faced before. However, it is essential to emphasize that medicine is constantly evolving. As time goes on, technologies and medi cal approaches also advance. Today, physicians have more sophisticated tools, like imaging studies, advanced laboratory tests and cutting-edge medical technology that complement these traditional skills. The combination of clinical experience and the use of modern medical technology allows for more accurate and effective medical care. In summary, traditional skills like taking a complete clinical history, observing care fully, performing a detailed physical exam and using common sense continue to be significant in medical practice. These skills are complemented 13 by the advances in medical technology, allowing us to provide better patient care.
Although technology has had a direct and categorical ef fect in decreasing teaching on the art of the physical exam, there are two other conditions that have significantly affected the practice of medicine and the professionals. These are the growth of the population and the implementation of a massive healthcare system to protect it, which has led to more patients being seen by doctors, as well as norms being established to regulate the length of appointments in outpatient departments.
It is important to stop to analyze how the study of semiol ogy has evolved over time and ask ourselves, "What would be the ideal way of teaching this subject to integrate it with the current technological advances?" It is worth remember ing that in the 50s, medical students were trained in this subject for 12 months; this was then reduced to six months, and in some medical schools in the United States, now it is taught for only three months. This time reduction has led to a decrease in the length and depth of the academic texts dealing with this subject.
From the semiology by Tiburcio Padilla and Pedro Cossio (Biblioteca de Semiología), consisting of eight volumes, to Cediel's medical semiology and exploratory technique in a single volume and, finally, to a more modern, evidence-based pocket semiology by Steven McGee, there have been significant changes. These new textbooks incorporate clinical epidemiology terms like the sensitivity, specificity, predictive value (±) and likelihood of the signs found in a patient. This more updated semiology fits the current language better or uses the same terms employed to decide when one diagnostic test is better than another, just like when a physician today decides which sign to look for in his/her patient based on this same terminology which allows the sensitivity, specificity and likelihood ratio of a sign to be classified.
This seems to be an advantage for new physicians-in-training to integrate each sign's measured efficacy with the efficacy of the complementary tests to be ordered, if necessary. This could help provide a smoother and more integrated transition consisting of teaching a less extensive semiology than in years past, but one that retains the essen tials of performing a physical exam looking for signs with a higher sensitivity, specificity and likelihood ratio, according to each case (Table 2).
Table 2 Test characteristics of the traditional physical exam findings versus POCUS for common diseases16.
| Disease | PE Finding | S (%) | Sp (%) | LR (+) | LR (-) | POCUS | S (%) | Sp (%) | LR (+) | LR (-) |
|---|---|---|---|---|---|---|---|---|---|---|
| Pleural effusion | Dull to percussion | 89 | 81 | 4.8 | 0.1 | Fluid visualized | 93 | 96 | 23 | 0.07 |
| Vesicular murmur | 88 | 83 | 5.2 | 0.1 | ||||||
| Pulmonary edema | Rales | 19-64 | 82-94 | 3.4 | NS | Bilateral B-lines | 94 | 92 | 10.4 | 0.06 |
| Pneumonia | Bronchophony | 14 | 96 | 3.3 | NS | Consolidation pattern | 94-95 | 90-96 | 13.5 | 0.06 |
| Egophony | 4 -16 | 96-99 | 4.1 | NS | ||||||
| Rales | 19-67 | 36-94 | 1.8 | 0.8 | ||||||
| Congestive heart failure | Rales | 12 - 23 | 88-96 | NS | NS | CVP >10 mm/Hg Inferior vena cava >2 cm | 73 | 85 | 4.9 | 0.32 |
| Jugular venous pressure | 10 - 58 | 96-97 | 3.9 | NS | ||||||
| Hepatojugular reflux | 55 - 84 | 83-98 | 8.0 | 0.3 | ||||||
| Edema | 10 | 93-96 | NS | NS | ||||||
| NS: not significant. | ||||||||||
Advances in medicine and medical technologies have had a significant impact on medical practice and teaching today. The incorporation of new technologies in teaching has revolutionized the way in which students learn and apply medical knowledge, highlighting the importance of integrating traditional skills and techniques with the new technologies 13.
In the past, only the history, physical exam and ausculta tion were key components of the medical assessment. These skills allowed physicians to obtain valuable information on the patient's condition through direct observation and the use of basic tools like the stethoscope. However, with tech nological advances, more sophisticated devices have been developed, leading to the question of whether this basic, traditional medical tool might fall into disuse, giving way to the use of a combination of digital auscultation supported by assisted artificial intelligence 14,15.
It is essential to integrate these new technologies into medical teaching to prepare students for modern clinical practice. The students should learn to use these devices and understand how they work, interpret likelihoods and ana lyze the data they produce. This means teaching students to use medical technologies effectively and integrate the findings obtained from these tools with the information gleaned from the physical exam and auscultation.
Teaching traditional skills like physical examination and auscultation continues to be relevant, as they provide information that cannot be obtained through modern bed side technology in all healthcare sites. The physical exam allows the patient's general appearance to be evaluated, organs palpated, masses or skin lesions identified, and a closer doctor-patient relationship established. Ausculta tion, in turn, allows abnormal heart and lung sounds to be detected, which may indicate underlying illnesses.
It is important to emphasize that technology does not completely replace the traditional skills and techniques, but rather complements them. Medical students should learn to integrate the information obtained from different sources, including physical examination, auscultation and advanced medical technologies. This involves develop ing clinical reasoning skills to make informed decisions and provide patients with quality comprehensive care. Therefore, we must consider whether semiology training textbooks should be rewritten to integrate the traditional with the modern, incorporating the interpretation of the sensitivity, specificity, positive predictive value, negative predictive value and likelihood ratio of a sign.
The tension between physical diagnosis and technologi cal tests has never been greater. Physicians have inherited an extraordinary tradition in terms of the physical exam but should also seek a balance in teaching students and residents, keeping in mind the modern realities of clinical diagnosis, which is often based on technological tests 16.
In the context of a developing country, where the avail ability of medical technology in rural areas may be limited, it is essential to provide balanced teaching integrating both the traditional physical exam as well as diagnostic technology. While the new medical technologies are ines timably beneficial in diagnosing and treating diseases, it is essential to recognize that they are not always easily ac cessible in health care settings. Therefore, medical students and residents must be trained in acquiring and mastering physical examination abilities, enabling them to perform an appropriate clinical evaluation even without advanced technology. This will ensure that these physicians are pre pared to face the challenges and limitations of rural areas, where there may be limited access to diagnostic tests. By encouraging balanced teaching combining both the tradi tion of physical examination and the available technology, quality comprehensive health care can be provided, adapted to the circumstances and resources in each setting.
Point-of-Care Ultrasound (POCUS)
Point-of-care ultrasound is a portable, easy-to-use ultra sound technique that allows physicians to obtain real-time images of the body's organs and internal structures. Unlike the stethoscope, which only provides auditory information, POCUS offers a direct and detailed view that can reveal crucial information about the patient's health status 16.
The adoption of POCUS has been a revolutionary change in modern medicine. Physicians can now perform rapid and precise bedside assessments, without having to refer patients to other services to obtain diagnostic images. This not only saves time and resources, but also improves clinical decision-making in patient care. Furthermore, POCUS has proven to be especially valuable in rural areas with limited medical resources or healthcare institutions which lack imaging technology 17,18.
Point-of-care ultrasound is a bedside ultrasound tech nique that uses high-frequency sound waves to create real-time images of the inside of the body. Traditionally, it has been used in specialized settings such as radiology de partments or diagnostic imaging centers. However, with the development of increasingly smaller and more accessible portable ultrasound devices, this technology has reached patients at their bedside or wherever they may be found, transforming the way in which physicians perform physical examination 18,19. This is a source of great surprise and maybe even satisfaction in physicians like us, whose youth was influenced by entertainment programs like Star Trek, and who now see how our clinical practice embodies the way in which Dr. McCoy and Mr. Spock made diagnoses with a pocket scanner.
Point-of-care ultrasound allows physicians to obtain real-time images of internal structures like organs, tissues and blood vessels right where the patient is receiving care. This provides immediate visual information and helps make rapid and accurate clinical decisions. For example, instead of depending only on auscultation with a stethoscope to evaluate a patient's heart, physicians can use POCUS echocardiograms to directly view the heart's function and detect structural or functional abnormalities.
Point-of-care ultrasound has also been used in various medical specialties like emergency medicine, anesthesiology, obstetrics and internal medicine, among others. It allows a rapid, non-invasive patient assessment, which may be es pecially useful in emergency situations or limited-resource settings. In the emergency room, POCUS has become a tool which, in trained hands, helps accurately determine diagnoses or clinical situations in real time, at a low cost and without side effects (it does not require radiation or the administration of a contrast medium). This gives it an important and increasingly present role in resuscitation rooms evaluating shock, pneumo thorax, heart failure, pneumonia, hypovolemia, intracranial hypertension, cerebral vasospasm, pleural or pericardial ef fusion, and venous-arterial thrombosis. It also allows follow up of procedures like vascular accesses, catheter placement, punctures and drainage, among other activities, proving that it has arrived to stay in emergency medicine, intensive care and, in general, patient bedside procedures 19-21.
Challenges and advantages of POCUS
It is true that today's medicine is facing challenges related to the workload and healthcare accessibility. Physicians of ten have limited time to evaluate patients and make clinical decisions. The introduction of modern medical technologies, like POCUS, can help speed up the diagnosis and treatment process, allowing a faster and more accurate assessment.
Regarding the system's coverage, it is important to keep in mind that the availability of modern medical technology may vary according to the site and available resources. Some places may have limited access to these technologies due to financial or infrastructure restrictions. However, as technol ogy advances and becomes more accessible, it is expected that these limitations will decrease over time.
The incorporation of POCUS into the physical exam has proven to have a significant impact on the sensitivity and specificity of the clinical assessment (Table 2). Point-of-care ultrasound allows physicians to directly view the internal structures of the body, providing immediate and detailed in formation that can complement or even surpass the traditional physical examination techniques 18-23.
As teachers, it is important to evaluate the risks of not developing and implementing an appropriate strategy for helping students to understand and use POCUS technology or other technologies in an assertive manner to complement the traditional physical exam. We cannot afford to lose our focus on what our clinical forefathers handed us in the medical act. This act should include a clinical history, a physical exam, and the patient's specific situation, as this will guide us toward an assertive decision regarding ordering biochemical, imaging or other complementary tests. It is the medical act which should determine which technology and complementary tests should be used to confirm the diagnosis, and not the other way around.
Conclusion
Point-of-care ultrasound has proven to be a revolutionary technology in the medical field (Figure 1). Its portability in smaller to larger sizes (cell phones, tablets, laptops, etc.) and its accessibility have transformed the way in which physi cians perform physical exams and make clinical decisions. The ability to obtain real-time images of organs and tissues directly at the patient's point of care has improved diagnostic precision and allowed a faster and non-invasive assessment. This is especially valuable in emergency medicine settings or institutions with limited resources.
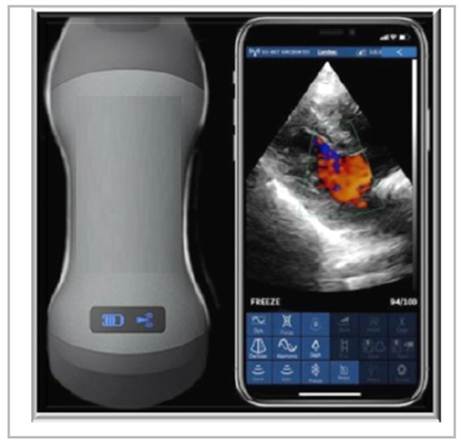
Figure 1 The EagleView, Philips Lumify, Butterfly IQ, and Vscan Airprobes have a double-headed transducer and are able to perform superficial to deep explorations of the body with a single movement, according to the companies' claims. These devices are useful for vascular, musculoskeletal, abdominal, cardiac, gynecological, obstetrical, urological, renal and pulmonary exploration.
However, it is important to keep in mind that there may be challenges in the general adoption of POCUS in terms of time and system coverage. Physicians already have a considerable workload, and the time devoted to each patient is limited. Furthermore, the availability of these technologies may vary according to the location and available resources. Although the limitations are expected to decrease as technology advances and there is more accessibility, the financial and infrastruc ture barriers must be addressed to ensure that all patients can benefit from this type of innovative technology in all types of healthcare services.
As an extension of the physical exam, POCUS has definitely managed to change the way in which healthcare is provided. However, work must continue to ensure its generalized and equitable adoption through all physicians in undergraduate and graduate training, as well as implement its use in healthcare services like primary care, home health, the emergency room, hospitalization and surgery.
It is important for medical schools to establish a compre hensive plan for training students and residents. The search for a balance between teaching evidence-based semiology and POCUS is important. The authors conclude that it would not be healthy to stop at the old-time medical teaching, but we should be realistic about the fact that, in our setting, not all urban or rural institutions will be able to acquire this technol ogy. Therefore, it is important for our future physicians and specialists to have a balance between both types of training to thus be able to respond to the needs of our reality. To con clude, some authors state that the stethoscope will disappear, while others insist that it will continue to be used, but in a limited fashion. To this we can only express the pride and nostalgia we felt when we obtained our first stethoscope and what it has represented in our lives as physicians, quoting Dr. Graham Easton (14):
"Tenemos un verdadero vínculo emocional, no solo los médicos, sino también los pacientes, con este icono fonen doscopio) de la medicina y la curación, simbólicamente, es una especie de conexión entre médicos y pacientes, como un cordón umbilical que va de uno a otro. A menudo, es la única vez que ponemos nuestras manos sobre un paciente durante un examen, y eso demuestra una atención cuidadosa, que sabemos que es muy poderosa en la curación"
The EagleView probe has a double-headed transducer and is able to perform superficial to deep explorations of the body with a single movement, according to the company's claims. The device is useful for vascular, musculoskeletal, abdominal, cardiac, gynecological, obstetrical, urological, renal and pulmonary exploration.

