text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
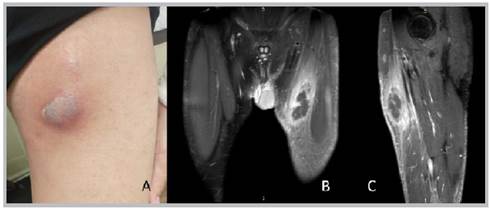
Figure 1 A: a photograph of the anterior internal aspect of the left thigh showing an abscess in the vertex of Scarpa's triangle. B: magnetic resonance imaging, coronal section, C: sagittal section showing an abscess and area of pyomyositis in the left thigh..
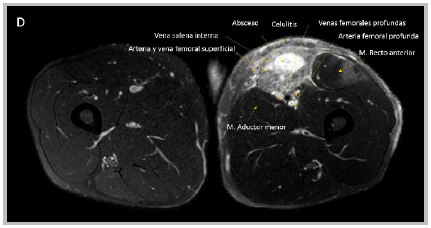
Pyomyositis 1 is an acute bacterial infection of the skeletal muscle with abscess formation. The incidence is 33-40%, mainly in young adult males. Staphylococcus aureus is responsible for 90% of the cases 2. It occurs due to dissemination from a distal infection or direct extension from an adjacent process. It has three phases: a) invasive: one to two weeks; b) purulent: the next 1021 days (90% of the patients consult at this stage); and c) systemic inflammatory response 3. A culture of the secretion and diagnostic ultrasound are required 4; magnetic resonance imaging is the test of choice 5. It is initially treated with antibiotics and requires surgical drainage in the second and third stages. Broad spectrum coverage is used in patients with comorbidities or immunosuppression, including Gram negative and anaerobic coverage. The reported mortality ranges from 2 to 20%, and is highest in patients with comorbidities.