











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Familial hypercholesterolemia (FH) is a genetic disease characterized by abnormally high plasma levels of cholesterol transported by low density lipoproteins (LDL-C) and high rates of morbidity and mortality at early ages 1,2. It is autosomal dominant, most often due to mutations in the gene that codes for the LDL receptors (LDLRs). Less often, it is due to mutations of the apolipoprotein B100 (apoB100) gene, the proprotein convertase subtilisin/kexin type 9 (PCSK9) gene, or the LDL receptor adaptor protein 1 (LDLRAP1) gene 3.
If untreated, both men and women with heterozygous FH (HeFH) with total cholesterol levels of 8-15 mmol/L (310580 mg/dL) typically develop premature coronary disease before age 55 and 60, respectively. Homozygous individuals, with total cholesterol levels between 12-30 mmol/L (4601,160 mg/dL), will develop premature coronary disease at a very early age, with a risk of death before age 20 if they do not receive adequate treatment; carotid, renal and femoral artery disorders are less common. Once diagnosed, patients with HeFH can be treated with lipid-lowering medications to attenuate the development of atherosclerosis and prevent coronary disease 4,5.
The prevalence of HeFH is estimated at one in 200-500 people, and that of HoFH at one in 300,000-600,000 people. With these data, there would be an estimated 96,000-240,000 people with HeFH and 160-300 people with HoFH in Colombia 6-8. The currently available information on the prevalence of FH in Colombia only allows us to derive extrapolated figures from international epidemiology, and, furthermore, there are no data indicating the prevalence of this disease in patients with prior cardiovascular or neurovascular events.
Materials and method
Study design
We performed an observational, analytical, cross-sectional study of anonymized secondary data from two tertiary care cardiovascular and neurovascular institutions in the metropolitan area of Bucaramanga, Colombia. All patients 18 years old and older with established coronary atherosclerotic disease (ischemic heart disease defined by myocardial infarction, angina, surgery or any other coronary revascularization procedure) and/or cerebral atherosclerotic disease (stroke or transient ischemic attack) were included, and patients with no evaluable lipid profile were excluded.
Sample size
The sample size was composed of the number of patients that make up the database of patients with established coronary and/or cerebral atherosclerotic disease between May 2017 and June 2018.
A total of 1,707 individuals from the anonymized databases at Instituto del Corazón de Bucaramanga and FOSCAL were analyzed, 470 of whom were found to have established coronary and/or cerebral atherosclerotic disease and laboratory data, and were included for analysis.
Data analysis
The analysis was evaluated and authorized by the FOSCAL research ethics committee. Subsequently, the data were analyzed through the previously described variables, obtained from an anonymized database. With the data collected, a database was set up in Excel, using a binary code, and transcription errors were corrected by reviewing the data from the 41 anonymous patients.
The data from the resultant database were statistically analyzed using the STATA 15 program. The sample size was calculated with different levels of confidence and margins of error to estimate a prevalence between 0.2-0.4%. The universe of patients in the database was analyzed, which helped estimate the prevalence of the target population and the factors associated with FH. Qualitative variables were described using proportions with their respective confidence intervals. Quantitative variables were described through means and standard deviation or medians, depending on their distribution. The intention of the univariate analysis was strictly descriptive.
Dependence analyses were done between the main sociodemographic and clinical variables and the prevalence of possible/probable HeHF. The prevalence was determined considering individuals classified as possible/probable cases of familial hypercholesterolemia; that is, those who scored 3 to 8 points on the Dutch Lipid Clinic Network (DLCN) criteria 6. Chi square or Fisher hypothesis tests were used for qualitative variables. Student's t or Wilcoxon Mann-Whitney tests were used for quantitative variables. An alpha level of significance of 0.05 was used for all statistical tests.
Results
In the study population, 300 patients (63.83%) were male, and 170 patients (36.17%) were female. The average age was 64.83 years, with the youngest being 26 years old and the oldest 97. The participants' most common socioeconomic level was 4, with 34.47%, followed by 3, with a frequency of 148, amounting to 31.49%. The most frequent risk factor in the study population was hypertension (HTN), reported in 72.77% of the patients, followed by dyslipidemia or being treated with lipid lowering drugs, in 57.45%, and smoking in 40.42% of the cases, 8.51% of whom were active smokers and 31.91% of whom had already quit. Altogether, 34.68% of the patients had a personal history of established coronary and/or cerebral atherosclerotic disease, and 27.23% had been diagnosed with diabetes mellitus, mainly type 2. The median weight was 73.25 kilograms (kg), with a maximum of 100 kg and a minimum of 41 kg. There were no records of tendinous xanthomas or corneal arcus.
As far as the lipid profile, the average total cholesterol level was 189.08 mg/dL, the average triglyceride (TG) level was 185.36 mg/dL, HDL-C was 40.91 mg/dL and LDL-C was 112.60 mg/dL. Other laboratory findings showed an average fasting blood sugar in the pre-diabetic range (113.43 mg/dL), average glycosylated hemoglobin (HbA1c) at 7.01%, TSH at 3.55 mIU/L, and creatinine at 1.00 mg/dL. The average creatine phosphokinase (CPK) level was 226.43 U/L, although it was only found in 10 medical charts.
Altogether, 88.09% (414) of the participants had LDL-C levels outside of the required targets, while only 11.91% (56) had LDL-C levels below 55 mg/dL. When stratified by LDL-C levels according to the Dutch Lipid Clinic Network (DLCN) criteria, 85.11% (400) of the population had levels less than 155 mg/dL and 9.57% (45) had levels between 155 and 189 mg/dL, while 4.68% (22) and 0.64% (3) had levels between 190 and 249 mg/dL and 330 mg/ dL or more. No patients reported LDL-C levels between 250-329 mg/dL. Of the 470 patients with coronary and/or cerebral atherosclerotic disease in the study, 338 (71.91%) exhibited none of the DLCN clinical probability criteria. The remaining 132 (28.09%) scored at least one point, as follows: 75 patients (15.96%) had one point, 20 (4.26%) had two points and 28 (5.96%) had three points. Only six patients (1.28%) had four points, one patient (0.21%) had five points, and two patients (0.43%) reached eight points.
After classifying the total score obtained according to the DLCN criteria, most of the patients (433, or 92.13%) were classified as unlikely FH cases. Thirty-five patients (7.45%) were classified as possible FH cases, and two (0.43%) as probable cases. No definite FH cases were found, as none of the patients underwent genetic analysis (Table 1).
Table 1 Probability of the clinical certainty of FH using the Dutch Lipid Clinic Network (DLCN) criteria.
| Criteria for a clinical suspicion of FH | n | % | Cumulative | 95%CI |
|---|---|---|---|---|
| Unlikely | 433 | 92.13 | 92.13 | 89.31-91.24 |
| Possible | 35 | 7.45 | 99.57 | 5.38-10.20 |
| Probable | 2 | 0.43 | 100 | 0.10-1.69 |
FH: familial hypercholesterolemia. Probable: from 6-8points, Possible: from 3-5points. Unlikely: fewer than 3 points.
It was confirmed that approximately one fifth of the study population (19.57%) walked for exercise, but only 14.26% did so for more than 150 minutes a week. A total of 1.91% of the population did some other type of aerobic exercise (like swimming, bicycling or jogging). Information on statin use prior to the cardiovascular event was found in 439 records (93.40%); of these,193 patients (43.96%) were on some type of statin, but only 13 (7.60%) received the maximum dose.
After the cardiovascular event, statins were prescribed for 426 patients. Of these, atorvastatin was the most prescribed, in 86.85% of cases, and only half of the patients, approximately 189 (51.08%), received the full dose (80 mg/day) at discharge. In order of frequency, rosuvastatin was the second most prescribed statin, in 6.10% of the cases, although it was the most frequently prescribed at full dose. Lovastatin (5.86%) and simvastatin (1.17%) were prescribed less frequently. Only two patients were statin-intolerant, leading to one of them not receiving statins and the other being treated with ezetimibe.
Beta blockers were the most used antihypertensive treatment, prescribed in 77.87% of the cases, followed by angiotensin converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) with 62.13%, diuretics (21.06%) and calcium channel blockers (16.38%). Regarding hypoglycemic therapy, metformin was the most used (12.55%), followed by insulin (8.51%), dipeptidyl peptidase 4 (DPP-4) inhibitors (4.68%) and sulfonylureas (1.06%), among others. Altogether, 87.87% of the patients received aspirin after the cardiovascular event, and 66.81% were prescribed clopidogrel or ticagrelor. Oral anticoagulation with warfarin was prescribed for 4.04% of the patients, with the same number being prescribed some type of direct oral anticoagulant (Table 2).
Table 2 Other medications prescribed after the cardiovascular event.
| Drug group | n | % | 95%CI |
|---|---|---|---|
| Antihypertensive drugs | |||
| Beta blockers | 366 | 77.87 | 73.87-81.40 |
| Calcium channel blockers | 77 | 16.38 | 13.29-20.02 |
| ACE inhibitors or ARBs | 292 | 62.13 | 57.63-66.41 |
| Diuretics | 99 | 21.06 | 17.60-25.00 |
| Hypoglycemic drugs | |||
| Metformin | 59 | 12.55 | 9.84-15.87 |
| Insulin | 40 | 8.51 | 6.29-11.40 |
| Sulfonylureas | 5 | 1.06 | 0.44-2.53 |
| SGLT2 inhibitors | 2 | 0.43 | 0.10-1.69 |
| DPP-4 inhibitors | 22 | 4.68 | 3.09-7.01 |
| GLP-1 agonists | 2 | 0.43 | 0.10-1.69 |
| Other pharmacological treatments used | |||
| Aspirin | 413 | 87.87 | 84.58-90.53 |
| Clopidogrel /ticagrelor | 314 | 66.81 | 62.40-70.93 |
| Warfarin | 19 | 4.04 | 2.58-6.26 |
| DOACs | 19 | 4.04 | 2.58-6.26 |
ACE inhibitors: angiotensin converting enzyme inhibitors. ARBs: angiotensin receptor blockers. SGLT2 inhibitors: sodium-glucose cotransporter-2 inhibitors. DPP-4 inhibitors, dipeptidylpeptidase-4 inhibitors. GLP-1 agonists: glucagon-like peptide-1 agonists. DOACs: direct oral anticoagulants.
Dependency was established between the patients> various sociodemographic and clinical variables and the prevalence of familial hypercholesterolemia (unlikely FH in those with scores between 1 and 3 points on the DLCN criteria; possible/probable FH in those with scores between 3 and 8 points), with significant dependency on the female sex in 54.05%, with p<0.05. There was no significant dependency on the socioeconomic level (Table 3).
Table 3 Dependency between the sociodemographic variables and the prevalence of familial hypercholesterolemia.
| Population characteristics | Unlikely FH (%) | Poss/prob FH (%) | p |
|---|---|---|---|
| Female sex | 150 (34.64) | 20 (54.05) | 0.021 † |
| Socioeconomic stratum | |||
| Stratum 1 | 25 (5.77) | 4 (10.81) | |
| Stratum 2 | 48 (11.09) | 5(13.51) | |
| Stratum 3 | 135 (31.18) | 13 (35.14) | 0.207 |
| Stratum 4 | 148 (34.18) | 14 (37.84) | |
| Stratum 5 | 62 (14.32) | 1 (2.70) | |
| Stratum 6 | 15 (3.46) | 0 (0.00) | |
FH: familial hypercholesterolemia; Poss: possible; prob: probable. f: Statistically significant difference
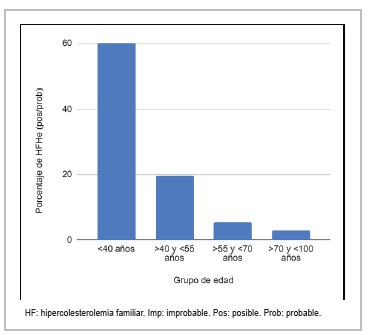
Patients with possible/probable FH were found to have a younger average age at onset of the cardiovascular events (55.83 years), compared with the rest of the patients (65.60 years), with a statistically significant dependency, p<0.0001. When the age variable was categorized, the highest prevalence of possible/probable HeFH was found in the under 40-year-old age group, with 60%; the 40-55-year-old group had 19.78%, the 55-70-year-old group had 5.39%, and there was a minimal prevalence of 2.99% for patients over the age of 70 (Figure 1).
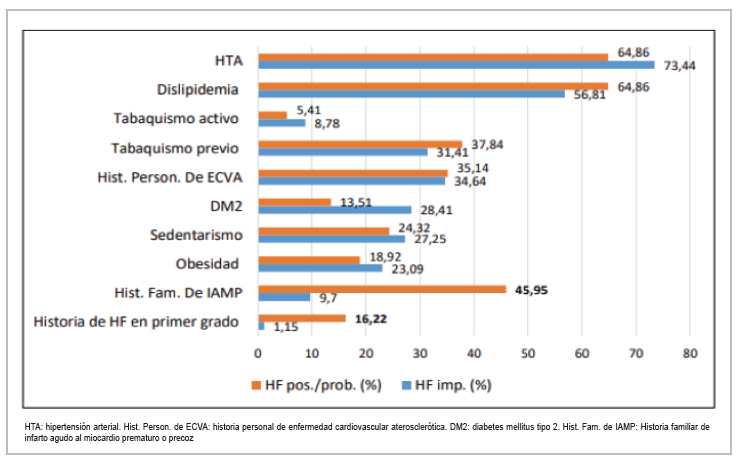
Regarding cardiovascular risk factors, a statistically significant relationship (p<0.0001) was found between having a history of first-degree FH and a family history of premature acute myocardial infarction (PAMI) and the prevalence of possible/probable FH (Figure 2). A statistically significant dependency (p 0.0001) was also found between patients with possible/probable FH and higher total cholesterol levels (263.24 mg/dL vs. 182.68 mg/dL). Likewise, these patients were found to have 1.5 times higher TG levels (271.82 mg/dL vs. 177.85 mg/dL), with a significant dependency (p 0.0001), and, as expected, 1.62 times greater LDL-C levels compared to the rest of the subjects (174.42 mg/dL vs. 107.14 mg/dL). None of the patients with possible/probable FH had target LDL-C levels. Furthermore, a dependency was found between the creatinine level (0.82 mg/dL) and the prevalence of possible/probable FH (p 0.005) (Table 4).
Table 4 Dependency between the biochemical findings and the prevalence of familial hypercholesterolemia.
| Parameter | Average poss/prob FH (n) | SD | 95%CI | p |
|---|---|---|---|---|
| TC (mg/dL) | 263.24 (37) | 76.99 | 237.57-288.91 | 0.0001 |
| HDL-C (mg/ dL) | 40.9 (37) | 8.50 | 38.06-43.73 | 0.99 |
| LDL-C (mg/ dL) | 174.42 (37) | 66.38 | 152.29-196.55 | 0.0001 |
| TG (mg/ dL) | 271.82 (37) | 245.21 | 190.06-353.58 | 0.0001 |
| Glycemia (mg/ dL) | 113.11 (30) | 47.9 | 95.22-130.99 | 0.96 |
| HbA1c (%) | 7.35 (9) | 2.09 | 5.74-8.96 | 0.56 |
| TSH (mUI/L ) | 3.55 (18) | 3.10 | 2.01-5.09 | 0.99 |
| Creatinine (mg/ dL) | 0.82 (37) | 0.17 | 0.77-0.88 | 0.005 |
TC: total cholesterol. HDL-C: high density lipoprotein-transported cholesterol. LDL-C: low density lipoprotein-transported cholesterol. TG: triglycerides. HbAlc: glycosylated hemoglobin. TSH: thyroid stimulating hormone. CPK: creatine-phosphokinase. FH: familial hypercholesterolemia. Poss: possible. Prob: probable. SD: standard deviation. f: statistically significant difference.
Most of the patients with possible/probable FH did some type of aerobic exercise other than walking, with a statistically significant difference (p 0.016), and most were physically active for more than 150 minutes per week, with a statistically significant difference.
Discussion
Our study's findings show that one out of every 13 patients (7.8%) with a cardiovascular event have possible/ probable FH. As far as we know, there are no studies in Colombia reporting the epidemiology, natural history or prevalence of FH and its complications. Regarding our results, the EUROASPIRE IV study, which enrolled 7,044 coronary patients from 24 European countries, found an FH prevalence of one in 12 patients (8.3%) by applying the DLCN criteria 9. On the other hand, some studies have reported lower FH prevalence levels in this type of special population, such as the one performed in Krakow on 341 patients with acute coronary syndrome (ACS), which showed an FH prevalence of one in 23 patients (4.4%), taking only probable and definite cases as a reference, based on the DLCN score 10. Another study by Faggiano et al. in patients with coronary disease and peripheral artery disease found a 3.7% prevalence of FH after including subjects with six or more points on the DLCN scale 9.
Rerup et al. found a 9.7% prevalence of possible FH (a DLCN score equal to or greater than 3 points) among 13,174 patients with acute myocardial infarction (AMI) 11 . A cohort of 1,843 Chinese patients diagnosed with AMI found a 3.9% prevalence of possible/probable FH 12 . A multicenter cohort study of 4,778 patients with ACS in Switzerland showed a prevalence of possible and probable/definite FH of 17.8 and 1.6%, respectively 13. The discrepancy between our results and those from other studies may be due to the fact that we did not only include probable cases, but also possible cases, considering that none of our subjects had a genetic analysis to be considered a definite FH case.
Patients with possible/probable FH were found to have an earlier age of onset of cardiovascular events (55.83 ±12.63, p 0.0001), similar to what has been found in the global population. Likewise, we found that this disease was more prevalent in women (54.05%), which has been reported previously 9. Regarding risk factors, dependency was only found between having a history of first-degree FH and a family history of premature AMI, and the prevalence of possible/probable HeFH. Despite finding a high prevalence of HTN (72.77%), no significant dependency was found with the prevalence of FH. In the same way, despite many patients with possible/probable FH having type 2 diabetes (DM2), this finding was not statistically relevant (p 0.055).
This information shows that the presence of conventional risk factors is less common in patients with possible/ probable FH compared to those without this disorder, indicating that these risk factors are not sufficient to predict risk in this group of patients, but rather there is a genetic component in the causality of atherosclerotic disease in this population 14.
Given the nature of the study, we could not determine which patients were on statins when the LDL cholesterol was measured. This raises the hypothesis of a greater prevalence of FH and will be the subject of a subsequent study in a prospective cohort.
Conclusions
This study established the prevalence of possible/probable FH among patients with established atherosclerotic disease, confirming the existent underdiagnosis of this disease and proving the existence of a higher prevalence in lower age groups. To increase the detection of patients with HeFH in our population, routine screening can be effectively employed by corroborating a history of first-degree FH, as well as a family history of premature AMI, together with an LDL-C level >174 mg/dL, and a score equal to or greater than three points on the DLCN criteria.
Conventional risk factors proved to be less frequent in subjects with possible/probable FH, indicating that these are not sufficient for predicting risk in this group of patients; rather, there is a known genetic component in the causality of atherosclerotic disease in this population. In addition, a younger age at the onset of the event may explain the fewer cardiovascular risk factors.
Despite most patients with HeFH receiving high intensity statins at the recommended dose, there is still a percentage of individuals who, after learning of the established atherosclerotic disease, do not receive the necessary lipid lowering treatment. In this context, it is important to evaluate possible gaps which have been reported in the diagnosis, treatment and follow up of high cardiovascular risk patients, such as not beginning statins appropriately, lack of screening for special populations (patients with a history of FH, DM, CKD, ACS, recurrent CVD), not beginning non-statin lipid lowering drugs like PCSK9 inhibitors and ezetimibe appropriately, and the inappropriate discontinuation of lipid lowering therapy 15.
Therefore, it is imperative to intensify the education of the teams treating high cardiovascular risk patients in order to not only provide proper treatment but also prevention.

