











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
INTRODUCTION
Currently, a surgical approach is often preferred for the treatment of clavicle fractures. The primary indications are fracture displacement, a third component, or neurovascular involvement for surgical treatment.1 Traditionally, anaesthetic management has favoured the use of general anaesthesia. Nevertheless, over the last few years, new regional techniques have been developed to improve postoperative pain control, opioid consumption, patient satisfaction and decrease hospital stay.
The innervation of the clavicle is complex and remains a controversial topic. Multiple nerves are involved in the sensory innervation of the clavicle, making it difficult to find an ideal option for postsurgical pain management. Although the interscalene brachial plexus block (IBPB) alone or in conjunction with a cervical superficial plexus block (CSPB) is the preferred technique, it is far from ideal due to the frequently associated phrenic nerve block.2
Recently, Valdez-Vichez3 described a new anaesthetic and analgesic approach for the management of the midshaft clavicle fractures: the clavipectoral fascia block (CPB). This technique involves spreading the local anaesthetic through the clavipectoral fascia (CPF) blocking the nerves that penetrate that structure. Some authors recommend complementing the CPB with a CSPB as the supraclavicular nerve from the superficial cervical plexus is responsible for the sensory innervation of the skin covering the shoulder, upper portion of the chest and clavicle.4 Although it is a safe and relatively easy regional approach, there are few publications in the literature about its effectiveness in distal clavicular fractures. This paper presents a case series of patients who received CPB with CSPB for midshaft and distal clavicle fracture repair with a discussion about the surgical and anaesthetic outcomes.
CASE SERIES REPORT
This is a case series of 8 patients who underwent surgical fixation for midshaft and lateral clavicle fractures. Informed consent for publication was obtained from all patients included in the study.
Both regional techniques were performed in the preanaesthesia room with the patient in supine position and the head turned to the contralateral side. A low-frequency linear probe (2 - 5 MHz; SonoSite SII; SonoSite INC., Madrid, Spain) and a 22-gauge 50 mm echogenic needle (Echoplex+; Vygon; Paterna; Spain) were used.
For the CPB, the probe was positioned perpendicular to the surface of the clavicle in the parasagittal plane. Initially, a sweep of the entire clavicle was performed to locate the fracture site. The clavicle is visualized as an hyperechogenic line with posterior shadowing. The pectoralis major can be seen caudally. After identifying the healthy periosteum adjacent to the fracture, the needle was advanced in-plane in a caudal to cephalic direction into the space between the CPF and the periosteum until contact was made (Figure 1A). Afterwards, the CSPB was performed positioning the probe transversely on the neck of the patient at the level of the cricoid cartilage. A transverse approach was used to identify the posterior border of the sternocleidomastoid muscle (SCM). In this position, the superficial cervical plexus is visualized anterior and medial to the paravertebral fascia. The needle was advanced inplane in a lateral to medial direction through the fascia posterior to SCM (Figure 1B). A local anaesthetic solution of 0.2% ropivacaine and 1% mepivacaine was used. With a previous negative aspiration, a total of 15 mL of the anaesthetic were injected medial and lateral to the fracture focus for the CPB and 5 mL for the CPSB. If the fracture site was distal, a single puncture was performed medial to the site.
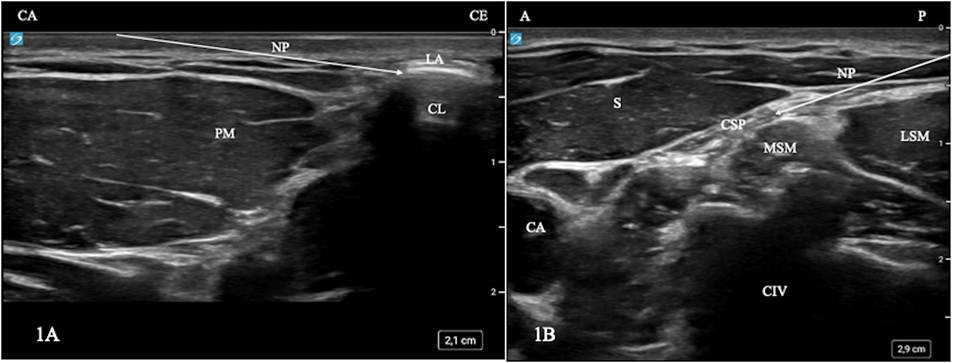
Source: Authors.
Figure 1 A: Ultrasound image of the clavipectoral fascia block (CPB): CA: caudal; CE: cephalic; CL: clavicle; NP: needle path; PM: pectoralis major. B: Ultrasound image of the cervical superficial plexus block (CSPB): A: anterior; CA: carotid artery; CIV: cervical four; CSP: cervical superficial plexus; LSM: levator scapulae muscle; MSM: scalenus medius muscle; NP: needle path; P: posterior; S: sternocleidomastoid.
After admitting the patient to the theatre, patient monitoring was started under non-invasive blood pressure, pulse oximetry and a 5-leads electrocardiogram. Afterwards, all patients underwent balanced general anaesthesia with laryngeal mask. Maintenance of anaesthesia was achieved with an oxygen/ air mixture and sevoflorane at 0.8 - 1 MAC.
During surgery, the patients received conventional intravenous (iv) analgesia (1 g of paracetamol and 50 mg of dexketoprofen). If during recovery the patients experienced pain >3 on the Numerical Pain Rating Scale (NRS), a rescue dose of tramadol was administered. If the pain persisted, a second rescue dose of 2 mg of morphine was used. Pain scores using the Numerical Rate Scale (NRS) during their stay in the recovery room and for the first 12 h and 24 h after surgery were recorded. The need for first analgesic rescue with iv tramadol or second rescue with morphine was also recorded. All of the demographic data, the characteristics of the surgery and the clinical results of the patients are shown in Table 1. No upper limb motor or sensory block was observed in any of the cases. No incidents or adverse events were documented during the first 24 hours that could be associated with the technique. Only one patient experienced pain according to the NRS pain scale in the recovery room. Moreover, most of the patients experienced only mild pain and only 3 patients reported mild pain according to the NRS scale at 12 h and 24 h respectively. It is even more significant that only one patient required a single dose of tramadol as rescue analgesia during the first 24 hours.
Table 1 Demographics, surgical characteristics and clinical results of the patients.
| Variables | Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | Case 6 | Case 7 | Case 8 |
|---|---|---|---|---|---|---|---|---|
| Age | 25 | 21 | 50 | 28 | 19 | 28 | 34 | 28 |
| Gender | F | M | M | M | F | M | M | M |
| ASA | II | I | II | II | I | I | I | I |
| Surgery | Midshaft | Distal | Distal | Midshaft | Distal | Distal | Distal | Midshaft |
| NRS Scores | ||||||||
| In PACU | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 0 |
| 12 h after surgery | 2 | 1 | 2 | 0 | 1 | 0 | 3 | 2 |
| 24 h after surgery | 1 | 0 | 0 | 0 | 0 | 0 | 2 | 1 |
| Analgesia rescue | No | No | No | No | No | No | Once | No |
ASA: American Society of Anesthesiologists; F: female; M: Male.
Source: Authors.
DISCUSSION
These results support the idea that CBP with CSPB are ideal regional techniques in the analgesic management of surgical clavicle midshaft and distal fractures. A review of the literature identified several publications demonstrating the potential efficacy of this nerve block. Most are small case series, similar to the one herein discussed and report comparable results.(5-6 However, the large majority of these publications focus on the effect of this technique on midshaft clavicle surgical repair. In our case, most patients had a distal clavicle fracture, demonstrating its efficacy in this subtype as well.
Currently there are some randomized control trials comparing the efficacy of CPB and IBPB in combination with CPSB.7-8 Although only one of these trials showed an analgesic improvement together with a longer duration of the block in the CPB group, both concluded that this technique prevented motor and hemidiaphragmatic paresis of the IBPB blockade. Furthermore, there were no incidents or adverse events reported during the administration of the clavipectoral fascia block, concluding that it is a safe and straightforward regional approach.
The clavicle innervation is complex and contoversial and we are gradually learning more and more about it. For this reason, there is some controversy about the analgesic mechanism of this regional technique. It is believed that the CPF, which supports the vascular and nervous components of the axillary space, encases the clavicle. This anatomical distribution facilitates the spread of the local anaesthetic around the periosteum. However, this theory contradicts classical published anatomical studies. Those studies describe the fascia as a supporting structure anchored to the periosteum of bones rather than embracing them. This anatomical distribution would limit rather than facilitate the spread of local anaesthetic. Two recently published studies in cadaveric models showed that the distribution of local anaesthetic in the CPB is different from what was originally imagined.9-10 Methylene blue was injected into cadavers on intact and fractured clavicles in the middle third. Both studies identified staining of the superficial muscle planes, the supraclavicular branches of the CSP and the anterosuperior portion of the clavicular periosteum. However, no detectable marking was observed in the deep muscle planes or in the posteroinferior portion of the clavicle.
In conclusion, we can assure that this novel technique is a safe and straightforward regional block that effectively controls pain during midshaft and distal clavicle surgery. Moreover, this approach avoids the side effects associated with other techniques, such as interscalene brachial plexus blocks that may lead to motor deficits or hemidiaphragmatic paralysis - which are poorly tolerated by patients with pulmonary conditions. However, further research is needed to assess the efficacy of the clavipectoral fascia block.

