text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
What do we know about this problem?
All of the international guidelines and consensus documents recommend that a known difficult airway be managed while maintaining spontaneous breathing during tracheal intubation. Currently, the safest and most widely used techniques are flexible bronchoscopy (considered the "gold standard") and videolaryngoscopy (as a novel approach). However, superiority of one over the other has not been yet established in terms of success on first attempt, overall success, time required, incidence of hypoxia during the procedure, or patient satisfaction.
What is the contribution of this study?
This study offers a systematic review and meta-analysis of the literature in 2024, comparing both intubation techniques in awake patients breathing spontaneously.
INTRODUCTION
Awake tracheal intubation (ATI) is the safest and most advisable method to secure a patent airway in patients with known or suspected airway (1-4). This procedure is usually performed using a fiberoptic bronchoscope (FB), considered the gold standard for the management of the difficult airway. Multiple devices have been developed over the past two decades for managing the difficult airway, including the videolaryngoscope (VL), which requires a skill that is easy to learn and maintain (4,5).
VL has advantages over FB. First, it provides a wider angle view of the glottic structures and improved spatial orientation, making it especially useful for the management of patients with pharyngeal and laryngeal malformations or abnormalities (6,7). Second, VL can create space in the upper airway to allow for effective aspiration of blood and secretions and facilitate topical anesthesia under direct vision (6-8). Third, there is no tracheal tube size limitation since it does not have the problem of space restriction associated with the encased FB tube; moreover, it can be easily exchanged as many times as needed during the procedure without removing the entire device from the airway (6). Fourth, in contrast with the need to advance the tube over the FB without the possibility to identify and bridge the structures which could be touched or impacted, advancement to the trachea can be observed under VL at all times, reducing the risk of impacting or injuring the epiglottis, arytenoids or other pharyngeal or laryngeal structures (6,9-11). Fifth, the VL device is portable, more accessible and easy to setup (12). Sixth, the process of acquiring and maintaining the skill is less demanding with VL compared to FB (13,14). Despite these theoretical advantages of VL, there are few published studies comparing the two techniques in awake intubation. In two meta analyses published in 2018 (15,16) and in 2021 (17), the authors did not find differences between the two devices in terms of success with the technique or the incidence of complications. Only intubation time was shorter with the use of VL. Evidence is yet insufficient to determine which of the two devices is ideal for awake intubation and the choice may perhaps depend on the clinical situation of each individual patient, the reason for requiring ATI, the availability of the device, and operator preference.
The objective of this systematic review and meta-analysis in 2024 was to examine de efficacy of VL as an alternative to FB in ATI.
METHODS
This systematic review and metaanalysis followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidance (18). It was previously (April, 2024) registered in PROSPERO (International Prospective Register of Systematic Reviews) under code CRD42024535061. All the authors agreed to the protocol before undertaking the review.
A literature search was conducted in PubMed, Web of Science and Cochrane Controlled Trials Central Registry (CENTRAL) in April 2024. The search strategy covered the following three families: videolaryngoscopy, flexible fiberoptic bronchoscopy, and awake intubation, together with their respective synonyms, with no language or publication date restriction. This strategy is described in the Supplementary material. Two authors independently assessed the literature according to the inclusion criteria. A third author intervened in case of disagreement between the first two reviewers. Only randomized controlled clinical trials comparing VL vs. FB for ATI regardless of indication were included. VL included channelled as well as non-channelled devices. Case series, observational studies as well as studies on mannequins, cadavers and those which included pediatric populations were excluded. To ensure search adequacy, published meta analyses were also reviewed in search for trials that might have been overlooked (15-17).
Two authors independently extracted data from the randomized clinical trials that met the inclusion criteria, using standardized Microsoft Excel spreadsheets. A cross review was carried out in order to identify discrepancies. The two authors reviewed the studies independently in accordance with the CONSORT (Consolidated Standards of Reporting Trials) checklist. Data extracted from the trials included: journal and publication year, author, number of included patients, inclusion and exclusion criteria, sedation technique, local anesthesia technique, operator experience, tracheal intubation approach (oral/nasal), type of airway device (FB/VL), and primary and secondary endpoint results.
The main objective of this review and meta-analysis was to compare the efficacy and safety of VL vs. FB in ATI. The primary outcomes were successful tracheal intubation on first attempt and tracheal intubation time. Secondary outcomes included the final success of the technique and associated complications (hypoxia, hoarseness or sore throat [%]). Continuous values were obtained as means and standard deviation (SD), as well as dichotomous values as total numbers and percentages. Continuous values are presented as medians and interquartile ranges or associated ranges, with the median estimated as the mean (19) and the interquartile range as the SD (20). If needed, the main authors would be contacted to solve questions regarding the methodology used, unclear data or data which were not presented in the original publication.
Statistical analysis
The R software together with the specific meta and metafor software packages were used for the combined analysis of the results of multiple studies. The random effects model described by DerSimonian and Laird was used to calculate summary statistics and their 95% confidence interval (CI) in the binary data analysis. This method estimates variance among studies and adjusts individual study weights, allowing for a more accurate estimate of the joint effect when heterogeneity is present. Heterogeneity was assessed using Cochran's Q test and the Higgins I2 statistic. The Q test allows to identify any significant differences among studies, whereas the I2 indicates the total per cent variance caused by heterogeneity among the studies.
For the combined and mean intubation time analysis according to the studied techniques, VL (experimental) and FB (control), a random effects meta-analysis was performed for the means difference. Mean values, standard deviations (SD) and sample size information of the selected studies were used. For the studies that provided 95% confidence intervals (CI), SD was calculated using transformations that consider CI length and study sample size. The standard error (SE) was derived from the standard deviation (SD) and sample size (n). In those cases in which medians and interquartile ranges (IQR) were reported, the values were adjusted to approximate means and SD, respectively (19-20).
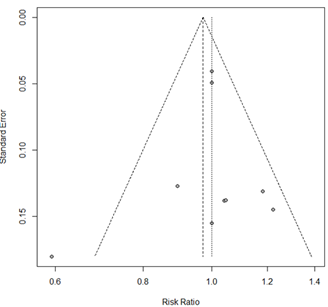
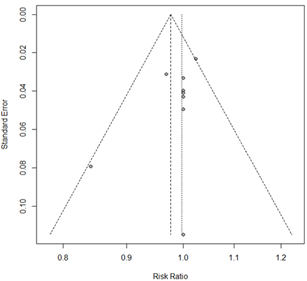
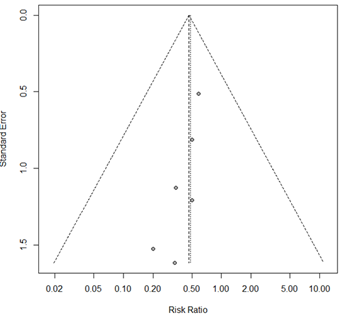
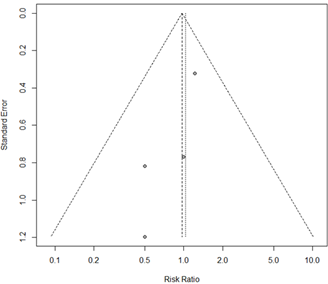
When a result was derived from single-study data, the effect estimates were specifically calculated on the basis of that single study. For results which could not be quantitatively synthesized in a meta-analysis, a qualitative systematic review approach was adopted. The results of the meta-analysis are presented as forest plots. Publication bias was evaluated by means of funnel charts.
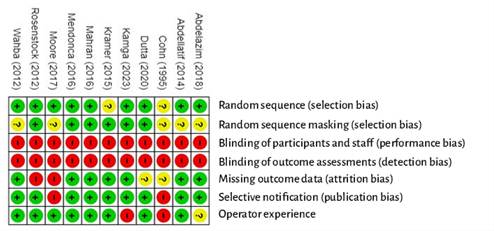
The risk-of-bias analysis was carried out independently by two of the authors using the Cochrane Manual for Systematic Review of Interventions (Cochrane Collaboration Risk of Bias [Rob2]) (21) Seven domains were analyzed: random sequence generation, random sequence masking, participant and staff blinding, result evaluation blinding, missing results data, selective results reporting, and operator experience. The risk of bias resulting from the degree of operator experience with the device used for tracheal intubation was also assessed because it was considered as a potential confounding factor. Each potential risk of bias was classified as low, high or unclear. Disagreements were resolved through discussion and involving a third author in the review. The relevant information of the studies was entered in a risk-of-bias table. Finally, a summary graph of the risk of bias was generated using RevMan Web.
The quality of the evidence of the results obtained in the meta-analysis was evaluated in accordance with the Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology using the GRADEpro software (http://gradepro.org). The reviewed domains included limitations or risk of bias, inconsistency, indirect evidence, imprecision and publication bias. A "GRADE evidence profile" table was then created using the GRADE software (www.gradepro.org) in order to assign a rating of high, moderate, low or very low quality to the results.
RESULTS
A total of 1,254 studies were identified. After the assessment process, 11 studies were included for qualitative review (22-32), with one of them (28) excluded from the metaanalysis due to missing data (Figure 1). Additional information was requested from the authors of five of the included articles (22,26-29) to whom at least four e-mails were sent. Only two of the authors provided the requested information (26,27).
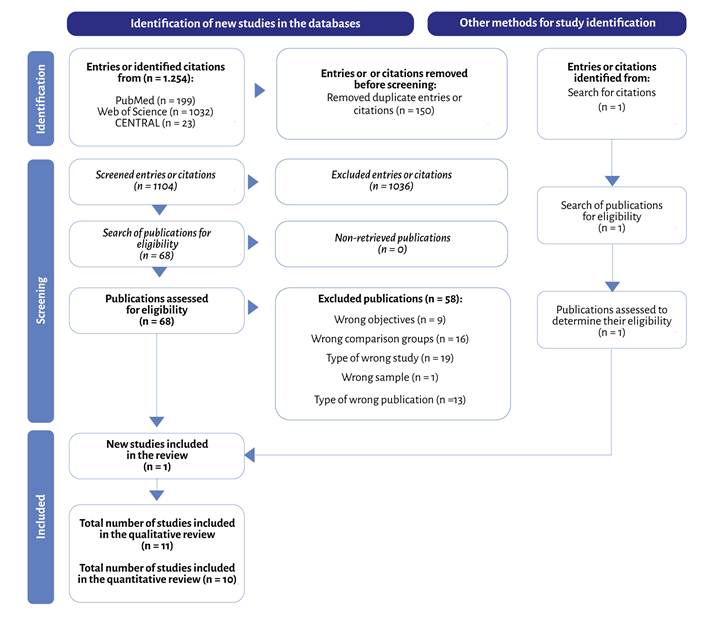
Source: Authors.
Figure 1 PRISMA, literature search flow diagram and selection of the included studies.
Description of the included studies
The most important characteristics of the 11 studies included in the review are shown in Tables 1 and 2 (22-32). In all of them, a VL device was compared with FB for awake intubation of patients undergoing surgery. The inclusion and exclusion criteria, as well as the type of surgery are described in Table 1. All tracheal intubations were performed under sedation and topical airway anesthesia. In three of the studies, the authors also used transtracheal anesthesia (23,31,32). The oral approach was used in the majority of the studies and the nasal approach to intubation was used in three (26,29,31). The experience of the operators who performed the procedure is described in Table 1. Table 2 lists the primary and secondary outcomes obtained in each study, as well as the VL used (22-26,28-30,32).
Table 1 Characteristics of the studies included in the review.
| Study author | n | Type of surgery | Inclusion criteria | Exclusion criteria | Anesthesia method | Oral/ nasal | Operator experience |
|---|---|---|---|---|---|---|---|
| Cohn et al. (1995) | 17 VL: 8 FB: 9 |
Cervical | Adults ASA I-III, cervical surgery with risk of neurological damage during intubation. | No data | - Sedation: fentanil, midazolam, droperidol. - Anesthesia: topical lidocaine |
Oral | Anesthetists or senior residents. Prior experience of ten successful intubations with the device. |
| Rosenstock et al.(2012) | 93 VL: 48 FB: 45 |
Gynecological, urological, abdominal, otolaryngological | Adults ASA I-III, anticipated difficult intubation or laryngoscopy and SARI ≥ 4. | ASA IV-V, Opening of less than 15 mm, poor dental condition, contraindication for transtracheal injection, indication for nasal intubation. | - Sedation: glycopirrolate, propofol, remifentanil (Ramsay 2-4). - Anesthesia: topical oral lidocaine, transtracheal lidocaine. |
Oral | SSix expert researchers. |
| Wahba et al. (2012) | 50 VL: 25 FB: 25 |
Cervical spine: Post traumatic fixation | Adults ASA I-II. | BMI ≥35 kg/m2, airway obstruction, cardiovascular disease, apparent difficult airway, patient refusal | - Sedation: glycopirrolate, midazolam, remifentanil. - Anesthesia: nebulized and topical lidocaine |
Oral | All airway expert researchers. |
| Abdellatif et al. (2014) | 63 VL: 31 FB: 32 |
Laparoscopic bariatric | BMI greater than 40 kg/m², difficult airway risk according to the El Ganzouri risk index >4. | Age <18 or >60 years, ASA >IV, severe mental disorder with inability to understand information, mouth opening <15 mm, poor dental condition, patient refusal. |
- Sedation: glycopirrolate, remifentanil. - Anesthesia: nebulized and topical lidocaine (spray or FB channel). |
Oral | One of the two researchers with more than 100 successful intubations with FB or VL. |
| Kramer et al. (2015) | 100 VL: 50 FB: 50 |
Maxillofacial | Need for nasal intubation, mouth opening > 13 mm, at least one difficult intubation criterion: Mallampati IV, incisor distance < 2,5 cm, documented previous difficult intubation, obstacle to intubation (tumor...). | Dental abscess, ASA ≥IV. | - Sedation: glycopirrolate, remifentanil, midazolam. - Anesthesia: topical lidocaine, nasal lidocaine gel, lidocaine spray to the glottis. |
Nasal | Nine expert researchers |
| Mendonca et al. (2016) | 40 VL: 20 FB: 20 |
Elective. 65% cervical | Adults, with criteria for awake intubation: Mallampati III-IV, limited cervical extension, protruding mandible, need to maintain the cervical spine in neutral position. | Mouth opening of less than 2,5 cm. Nasal intubation, pregnancy. |
- Sedation: midazolam, remifentanil. - Anesthesia: topical lidocaine, “spray as you go” through cannula. |
Oral | One expert researcher. |
| Moore et al. (2017) | 11 VL: 5 FB: 6 |
Bariatric | SARI ≥ 4. | No data. | - Sedation: glycopirrolate, midazolam, remifentanil. - Anesthesia: topical lidocaine. |
Oral | Experience with more than 40 intubations with the device |
| Mahran et al. (2017) | 54 VL: 27 FB: 27 |
Pharyngeal | Oropharyngeal cancer, 20-60 years, ASA I-II, Mallampati II-III. | Patient refusal, restricted mouth opening, contraindication for nasal intubation. | - Sedation: glycopirrolate, remifentanil. - Anesthesia: topical nebulized lidocaine. |
Nasal | Two trained researchers familiar with both techniques. |
| Abdelazim et al. (2018) | 60 VL: 30 FB: 30 |
Any elective surgery in obese patients | ASA II, BMI ≥ 35, 18-60 years, EGRI ≥ 4, elective surgery. | Risk of aspiration, severe disease conditions, cervical pathology, upper airway pathology, informed consent not signed. | - Sedation.: midazolam, fentanil. - Anesthesia: lidocaine spray. |
Oral | No data |
| Kamga et al. (2023) | 78 VL: 39 FB: 39 |
Unspecified. All except nose and mouth. |
Adult with indication for awake intubation. | Mouth opening less than 16 mm, and mouth or nose surgery. | - Sedation: remifentanil. - Anesthesia: topical lidocaine, superior laryngeal nerve block, transtracheal lidocaine injection. |
Nasal (FB) Oral (VL) |
Expert or supervised resident |
| Dutta et al. 2020 | 46 VL: 23 FB: 23 |
Cervical due to instability | Adults, 18-65 years, ASA I-II, with unstable cervical pathology (C1-C4). | Oropharyngeal pathology, mouth opening of less than2,5 cm, emergent surgery, pregnancy or failure to sign informed consent. | - Sedation: glycopirrolate, fentanil. - Anesthesia: bilateral superior laryngeal nerve block and transtracheal lidocaine injection,10% lidocaine spray to the oropharynx. |
Oral | One researcher with experience using both technique (>25 intubations). |
EGRI: El Ganzouri Risk Index; SARI: Simplified Airway Risk Index.
Source: Authors.
Table 2 Videolaryngoscopes used and primary and secondary outcomes obtained in the reviewed studies.
| Study author | Videolaryngoscope | Primary outcome | Secondary outcome |
|---|---|---|---|
| Cohn et al. (1995) | Bullard | Time to glottis visualization and intubation time. | Anatomical abnormalities predictive of difficult intubation. |
| Rosenstock et al. (2012) | McGrath | Intubation time. | Intubation on first attempt, number of attempts, success with the technique, number of esophageal intubations, glottis visualization, ease of the technique (0-10), patient discomfort (VAS), complications (SpO2 <90%, dental injuries, tissue da- mage). |
| Wahba et al. (2012) | GlideScope | Intubation time. | Intubation on first attempt, number of attempts, heart rate, blood pressure, neurological status, desaturation, airway discomfort (sore throat, hoarseness), patient satisfaction (1-3: excellent-poor). |
| Abdellatif et al. (2014) | GlideScope | Intubation time. | Number of intubation attempts, better glottic visualization according to the Cormack and Lehane scale. Patient response to intubation. Sore throat or dysphonia on postoperative day 1, patient satisfaction (excellent = 1, good = 2 and fair = 3). |
| Kramer et al. (2015) | C-MAC | Intubation time. | Technique success, glottic visualization, anesthetist satisfaction, patient satisfaction, complications. |
| Mendonca et al. (2016) | Pentax AWS | Intubation time. | Intubation time, midazolam dose, remifentanyl, lidocaine. Improved glottic visualization according to the Cormack Lehane scale. Complications such as dental injury or signs of airway harm. |
| Moore et al. (2017) | GlideScope | Intubation time. | Number of attempts, changes in heart rate, difficulty of the procedure VAS 0-10, patient satisfaction VAS 0-10. |
| Mahran et al. (2017) | GlideScope | Intubation time. | Success on first attempt (considered a failed attempt if intubation time is >3 minutes). Glottic visualization according to the Cormack and Lehane scale. Incidence of complications: sore throat, bleeding. |
| Abdelazim et al. (2018) | C-MAC | Intubation time. | Intubation success. Glottis exposure. |
| Kamga et al. (2023) | Airtraq | Success rate (six respiratory cycles on capnography). | Intubation time, number of attempts, success rate on first attempt, adverse events (cough, hypoxia, distress, nausea). |
| Dutta et al. (2020) | McGrath | Cervical movement during intubation. | Motor abnormalities following intubation, hemodynamic changes, intubation time, number of attempts, success rate on first attempt, complications(SaO2 less than 94%), patient satisfaction with the technique. |
Source: Authors.
The risk-of-bias assessment of the studies included in the review is illustrated in Figure S1 (Supplementary material). All of the studies describe the randomization method; however, there are questions on whether the procedure was really random with sufficient guarantees in two studies (26). The risk of selection bias, attrition bias and selective notification bias was low in the majority of the studies. Given the characteristics of the intervention, blinding of participants, staff and reviewers of the results was not possible and, therefore, performance and detection risk of bias was considered high for all the studies. The anesthetists who participated in the study by Cohn et al. (22) had only performed "at least 10 intubations with using VL or FB"; given that the learning curve for FB is considered steeper than for VL, the risk of bias was considered high because of the potential bias in favor of the VL group. In the study by Kamga et al. (31) no experience with VL was required in the awake patient, leading us to consider a high risk of bias in this study because of the potential benefit for the FB group. Given the high risk of bias and the absence of results, we decided not to include the study by Moore et al. in the meta-analysis (28).
In accordance with the GRADE methodology for assessing the quality of the evidence for each of the results extracted from this meta-analysis, the quality of the evidence was considered moderate for success on first attempt, overall success with the technique and hypoxia outcomes; low for intubation time; and very low for sore throat or hoarseness (Table 3).
Table 3 Quality of the evidence, GRADE System.
| Certainty evaluation | No. of patients | Effect | Certainty | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study number | Study design | Risk of bias | Inconsistency | Indirect evidence | Imprecision | Other considerations | Videolaryngoscope | Fiberoptic bronchoscope | Relative (95% CI) | Absolute(95% CI) | ||
| Success on first attempt | ||||||||||||
| 9 | Randomized trial | Higha | Low | Low | Low | None | 229/287 (79.8%) | 237/289 (82.0%) | RR 0.97 (0.90 to 1.05) | 25 less for 1000 (from less than 82 to 41 more) | ⨁⨁⨁◯ Moderate | Critical |
| Intubation time | ||||||||||||
| 10 | Randomized trials | Higha | Highb | Low | Low | None | 285 | 295 | - | MD 50.39 seconds less (from 82 to 87.7 less) | ⨁⨁◯◯ Low | Critical |
| Overall success | ||||||||||||
| 9 | Randomized trials | Higha | Low | Low | Low | None | 258/268 (96.3%) | 267/271 (98.5%) | RR 0.98 (0.95 to 1.01) | 20 less for 1000 (from 49 less to 10 more ) | ⨁⨁⨁◯ Moderate | Critical |
| Hypoxia | ||||||||||||
| 7 | Randomized trials | Higha | Low | Low | Highc | Strong association | 9/229 (3.9%) | 21/232 (9.1%) | RR 0.47 (0.23 to 0.98) | 48 less for 1000 (from 70 less to 2 less) | ⨁⨁⨁◯ Moderate | Critical |
| Sore throat or hoarseness | ||||||||||||
| 4 | Randomized trials | Higha | Low | Low | Very highd | None | 19/113 (16.8%) | 20/114 (17.5 %) | RR 0.97 (0.57 to 1.66) | 5 less for 1000 (from 75 less to 116 more) | ⨁◯◯◯ Very low | Important |
CI: Confidence interval; MD: Mean difference; RR: Risk ratio.
Explanations
a. The characteristics of the analyzed intervention preclude blinding of both participants as well as reviewers, making performance and detection biases difficult to avoid.
b. The heterogeneity identified in the review could be due to the differing definitions of the measured parameter “Time taken to perform tracheal intubation”. For example, some authors consider that intubation has been successful when the tube passes between the cords, while others believe that the process has been completed when six capnography waveforms are obtained.
c. The RR 95% CI (0.23-0.95) includes the reference threshold value of 0.75. The calculated optimal information size (381 in FB and 377 in VL) for the results obtained is higher than the number of patients contributed by the studies. The low number of events might not allow to adequately assess result size.
d. The RR 95% CI (0.57-1.66) exceeds the reference threshold values of 0.75-1.25. The calculated optimal information size (45,722 in FB and 45,311 in VL) for the results obtained is higher than the number of patients contributed by the studies. The low number of events might not allow to adequately assess result size.
Source: Authors. (gdt.gradepro.org).
Tracheal intubation on first attempt
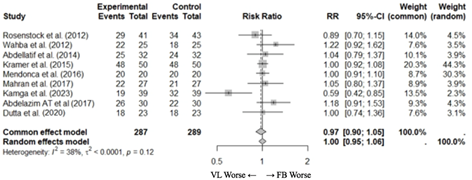
Nine studies (23-27,29-32) with 576 patients reported the percentage of patients intubated on first attempt. Two studies did not report this outcome, but the information was obtained after contacting the authors (26,27). It was impossible to get in touch with the authors of one of the studies (22). The pooled meta-analysis of the included studies did not show statistical difference between VL and FB in terms of the percentage of patients with tracheal intubation on first attempt (RR [95% CI] 1.00 [0.95-1.06]) (Figure 2a).
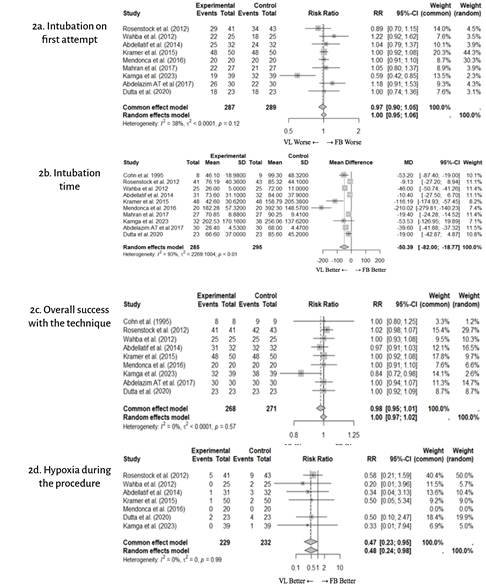
Intubation time
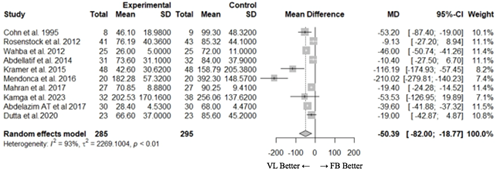
All ten included studies (22-27,29-32) with 580 patients described tracheal intubation time. The pooled meta-analysis of the included studies found a statistically significant difference for this parameter. Intubation times with VL were shorter when compared with FB (mean difference [95% CI]: -50.39 [-82.0;-18.8] seconds) (Figure 2b). Considerable heterogeneity was found among the studies (12 = 93%), a potential explanation being differing definitions of intubation time among the included studies: from the time of introduction of the device into the mouth to one capnography waveform (23,27,30); from introduction to three capnography waveforms 5; from device introduction to six capnography waveforms (31); from VL introduction into the mouth or introduction of the FB inside the tube to cuff inflation (26); from the introduction of the device into the mouth to endtidal CO2 > 20 mm Hg (29); from the introduction of the device into the mouth to capnography waveform display, auscultation, and verification of chest movement with ventilation, tidal volume and airway pressures (32). No answer was obtained from one author to the request for detailed information regarding the criteria for measuring intubation time (22).
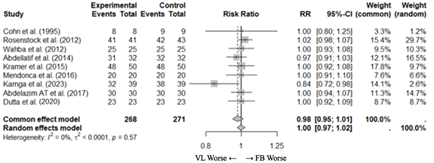
Overall success with the technique
Nine studies (22-27,30-32) with 539 patients reported details on the success of the technique. This information was not provided in only one study (29) whose authors we attempted to contact unsuccessfully. The pooled meta-analysis of the included studies did not show a statistically significant difference between VL and FB (RR [95% CI] 0.99 [0.97; 1.02]) in terms of the percentage of patients with overall ATI success (Figure 2c).
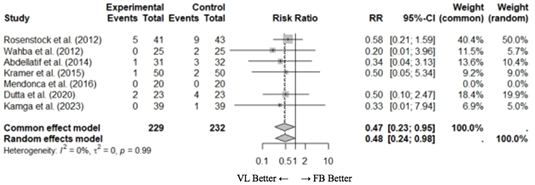
Hypoxia
Seven studies (23-27,31-32) with 461 patients described the incidence of hypoxia during tracheal intubation. The pooled meta-analysis of the included studies showed a higher incidence of hypoxia during ATI with FB compared with VL (RR [95% CI] 0.48 [0.24; 0.98]) (Figure 2d). Hypoxia was defined as SaO2 of less than 90% in five studies, less than 92% in one study, and less than 94% in another study.
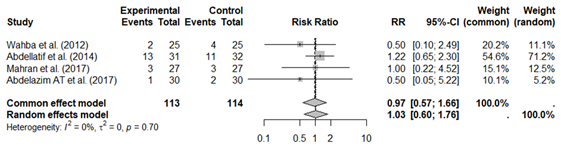
Sore throat, hoarseness
Four studies (24,25,29,30) with 227 patients described the incidence of sore throat or hoarseness following the procedure. The pooled meta-analysis of the included studies did not show a statistically significant difference in the incidence of sore throat or hoarseness after ATI with either VL or FB (RR [95% CI] 1.03 [0.60; 1.76]) (Figure 2e).
Satisfaction with the technique
Satisfaction with the technique was described in six studies and was adequate in most cases. Differences across scales and criteria used to assess patient satisfaction precluded a pooled analysis of the data, hence our inability to give an opinion regarding potential differences between both techniques (Table S1, Supplementary material).
DISCUSSION
The aim of this systematic review and meta-analysis conducted in 2024 was to inquire into the efficacy of VL as an alternative to FB in ATI. We did not find a significant difference between the two devices in terms of the percentage of patients intubated on first attempt or overall success with the technique. However, we observed found shorter intubation times with VL, associated, in turn, with a lower incidence of hypoxia.
Until recently, FB was considered the gold standard for ATI. This meta-analysis found that VL is as effective in terms of success and intubation on first attempt. It is important to bear in mind that this is a comparison of randomized, controlled studies which included nonurgent surgical procedures (22-32). In each of these studies, patients had to meet a range of conditions such as neck surgery due to instability (22,24,27,32), obesity (25,28,30), or maxillary-pharyngeal surgery (26,29), and had to have adequate mouth opening (22-32). However, in clinical practice, the situation is not usually as controlled, with patients having a wide range of airway characteristics and specific clinical conditions which could influence the clinician's choice of one device over the other (6-11). For example, in patients with limited mouth opening, the use of FB could be more advisable, while VL could be a better choice in patients with blood or secretions in the pharynx. Of the studies included in this meta-analysis, only the one by Kamga et al. (31) found a higher number of intubations on first attempt with the use of FB (82% vs. 49%) and higher overall success with this technique (97% vs. 82%) as compared with VL. Kamga et al. (31) used the oral approach when intubating with the Airtraq® VL, and the nasal approach when using the FB device. In their discussion, the authors report that their findings could be explained, at least in part, by the fact that a high percentage of Airtraq® intubations had been performed by staff without previous experience using the device (31).
The primary endpoint of most of the studies included in our review was intubation time (2-30), maybe because in many cases the authors assumed no differences would be found in terms of success with the technique with either of the devices. In our meta-analysis, shorter intubation time of close to 50 seconds was observed with the use of VL, although the degree of heterogeneity among the studies was high (I2=93%). This high degree of heterogeneity could be due to the differences in the definition of intubation time used across the studies, variations in terms of inclusion and exclusion criteria, or the different clinical situations included in each of the studies (15,22-32). We have no knowledge of the clinical implication of a shorter awake intubation time but, in theory, sedation and airway anesthesia, recommended in awake intubation, could diminish laryngeal reflex (2), limit inspiratory flow (33), increase the odds of gastric aspiration (2) and even fully obstruct the airway (11). Shorter awake intubation time could reduce the incidence of these complications and lessen patient discomfort. Moreover, given the need to perform urgent awake intubation due to airway compromise, shorter performance time could be crucial.
In this meta-analysis, we observed that ATI using VL was associated with a lower incidence of hypoxia (3.9%) when compared with the use of FB (9.0%). In two meta-analyses published in 2018, despite a trend towards a decrease in hypoxia in the VL group, the authors of those studies did not find significant differences (15,16). The reviewed meta-analyses included five studies (23-27) and 337 pacientes. This meta-analysis included an additional two studies (31,32) with 461 patients. The higher incidence of hypoxia in the FB group could be due to the longer time needed for intubation using the FB device and the fact that its introduction into the trachea reduced airflow, even more so when the tube is advanced between the vocal cords. The difficulty of passing the tube into the trachea over the FB, impacting the epiglottis, the arytenoids, or other laryngeal or pharyngeal structures (6,9-11) could also explain this higher incidence of hypoxia. It is important to bear in mind that the majority of the studies in the meta-analysis include patients scheduled for elective surgery who are, in theory, in adequate clinical condition. It may be that in patients with airway compromise as a result of tumors or abscesses, urgent surgery or unstable clinical conditions, the variation in the incidence of hypoxia between the two devices could be higher, in favor of VL due to shorter intubation times.
In this study a problem we found when comparing FB vs. VL was the wide range of VL devices available in the market. Two of the studies included in the meta-analysis used a channelled VL (27,31) while the rest used non-channeled VL devices (22-26,28-30,32). A recent study (24) has compared both types of VL devices for awake intubation, with no difference found between the two in terms of glottis visualization, success with the technique, complications or patient satisfaction. Only the percentage of intubated patients on first attempt was higher with the non-channelled blade VL.
In this work, no differences were found between FB and VL in terms of sore throat or hoarseness. As for patient satisfaction, adequate sedation and airway anesthesia are key (2) when performing awake intubation. This review did not find differences in terms of patient comfort, although measurements of this parameter varied considerably across the different studies, making it impossible to conduct a meta-analysis.
This meta-analysis has several limitations. The first one has to do with the fact that patient inclusion criteria and the types of surgeries were different across the various studies (22-32). This diversity could be considered a source of bias, although it can also be viewed as a more representative sample of the clinical reality pertaining to the use of VL and FB in clinical practice. Second, the majority of the studies included surgical patients taken to elective surgery in a controlled environment, so results should no be extrapolated to urgent surgery and physiologic difficult airway cases, considering that the incidence of complications, such as hypoxia, could increase in such situations. Third, all the studies excluded patients with restricted mouth opening, perhaps underestimating the role of FB in the management of these patients who require awake intubation. Fourth, there was great variability in terms of the VL devices used. Two studies used channeled blade VL (27,31) and nine studies used non-channelled blade devices (22-26,28-30,32). Among the latter, the GlideScope® was used in four studies, the C-MAC® in four, the McGrath® in two and the Bullard®, Pentax AWS® and Airtraq® in one study each (Table 2). Additional studies comparing different VL devices are required in order to recommend the best option for ATI (34,35). Fifth, the definitions of some of the parameters varies across studies, in particular as relates to intubation time, possibly explaining the high heterogeneity as far as this outcome is concerned. Finally, although in the majority of the studies included in the review the operators performing tracheal intubation were "experts", the definition of what "expert" meant varied across the studies (Table 1). For example, in the study by Cohn et al. (22) experts referred to anesthetists who had successfully performed more than 10 tracheal intubations, while for Abdellatif et al. (25) the bar was set at 100 tracheal intubations. It has been estimated that an anesthetist would have needed 25 FB intubations to acquire competency with this technique, as compared with only 6 VL intubations (13,14). This advantage of VL over FB in terms of acquiring and maintaining competency might mean that new practitioners will choose VL when lacking experience with either type of device, and in particular in urgent situations which were not assessed in any of the included studies.
CONCLUSIONS
ATI with either VL or FB is equally effective in terms of successful intubation on first attempt (Certainty of the evidence: Moderate) or overall success with the technique (Certainty of the evidence: Moderate). The use of VL was associated with shorter intubation time (Certainty of the evidence: Low) and a lower incidence of hypoxia (Certainty of the evidence: Moderate).
Further studies designed to assess patient and operator satisfaction are needed in order to determine if there are any differences between the two techniques in the awake patient.
ACKNOWLEDGEMENTS
Authors' contributions
JF: Planning, literature search, interpretation of the results, drafting and review of the manuscript, analysis of the quality of the evidence.
MT: Planning, data collection, interpretation of the results, drafting and review of the manuscript, evidence and bias analysis.
MB: Planning, data collection, interpretation of the results, bias analysis.
BCS: Literature search, data collection, drafting of the manuscript.
PLC: Literature search, data collection.
JA: Planning, final review of the manuscript.
TSP: Statistical analysis of the results.