











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Graft-versus-host disease affects 30 to 80% of hematopoietic stem cell transplantation recipients 1, and it is the principal cause of non-relapse mortality after this type of transplantation 2,3. This pathology produces a severe inflammatory process, affecting the skin, the gastrointestinal system, and the liver 4.
The standard treatment is systemic steroids; however, approximately in 50% of patients the disease will be steroid-refractory 5,6. Different second- line systemic therapies have been used 7. All these agents increase immunosuppression and predispose the patient to infections and secondary neoplasms 8. The prognosis of steroid-resistant or dependent graft-versus- host disease tends to be poor, independently of the choice of systemic treatment 9,10.
There is a critical need to establish a standard treatment for severe graft- versus-host disease and to continue advancing in prevention strategies 11,12. Various groups have demonstrated that infusing steroids directly into the artery supplying the organ affected by the disease (such as the liver or intestine) is safe and can induce its remission 2,13-15. The localized injection of steroids aims to deliver a higher dose of the drug to the target organ, achieving low systemic levels and avoiding related unwanted effects 16-19.
Our institution is a reference center in the country for performing hematopoietic stem cell transplantation in pediatric patients. Since 2016, we have used intra-mesenteric steroid injections for pediatric patients post- transplantaion with gastrointestinal graft-versus-host disease, administered by pediatric interventional cardiologists. Currently, in patients diagnosed with moderate-to-severe disease who do not respond to the initial management, we use early intra-mesenteric steroid injection.
Limited data exists on using steroids to manage refractory graft-versus- host disease in children 20. This study aimed to describe the clinical outcomes and our experience with 21 pediatric patients diagnosed with steroid-refractory graft-versus-host disease who received intra-mesenteric steroid treatment. To our knowledge, this is the largest pediatric cohort reported in Latin America.
Materials and methods
Patients
This is a retrospective observational case series that included patients under 18 years who received allogenic hematopoietic stem cell transplantation for any indication and required intra-mesenteric steroid injection for therapy-resistant moderate to severe gastrointestinal graft- versus-host disease between January 2016 and December 2021.
Steroid-refractory was defined as the progression of the disease after three days, lack of response after seven days, or incomplete response after 14 days of initiating the standard treatment. Steroid dependence was defined as a response that reappears when the steroid dose is decreased 21.
Graft-versus-host disease prophylaxis was assigned according to the donor type: cyclophosphamide for haploidentical donors 21; and calcineurin inhibitors, and methotrexate or mycophenolate, for identical donors 22.
Methylprednisolone was administered via intra-mesenteric injection into the celiac trunk and the superior and inferior mesenteric arteries, at 1 mg/kg (up to a maximum of 60 mg per artery) diluted in 10 ml of 0.9% saline solution.
Thrombocytopenia did not contraindicate the procedure. Patients with platelet counts below 50,000 cells/μΙ were transfused on the day of the procedure to achieve a safe value before the intervention.
Technique used
Using the Seldinger technique, the femoral artery was catheterized using 4- or 5-Fr introducers, depending on the patient’s age and weight. A 4- or 5-Fr pigtail catheter was then advanced to perform aortic angiography and locate the celiac trunk, and the superior and inferior mesenteric artery.
Once these arteries were located, a 4- or 5-Fr Cobra catheter was used to catheterize individually the celiac trunk and the superior mesenteric artery. If catheterization of the inferior mesenteric artery was not feasible with the cobra catheter, a Sigmon 1 catheter was used as an alternative. Then, methylprednisolone was injected into each artery for three minutes per injection 4,23 (figure 1).
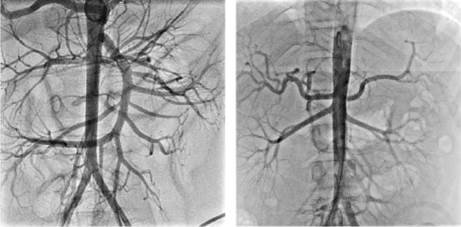
Figure 1 Intra-arterial steroid injection. Proof of correct catheter placement during intra-arterial steroid injection: celiac trunk (left), inferior mesenteric artery (right).
After the procedure, the patients continued receiving the front-line management established for graft-versus-host disease. Patients with partial response received a second dose two weeks after the first application. Patients were on bed rest with restricted limb flexion for two to six hours after the injection. Associated complications were addressed after the intervention (hematoma, arterial bleeding, dissection or thrombosis, arterial spasm, and cellulitis).
Variables
Clinical and demographic characteristics of the patients were collected, along with outcomes associated with the intra-mesenteric steroid injection procedure and with the post-treatment of gastrointestinal graft-versus-host disease, overall survival and mortality related to relapse 24 months after hematopoietic stem cell transplantation.
Response time was defined as the period between the day of the intramesenteric steroid treatment and the observed response in the next two weeks. Each affected organ was evaluated according to the following criteria:
Hepatic: A decrease of 25% in serum bilirubin levels from their baselines was called “partial response”, and reaching normal bilirubin levels was denominated “complete response”.
Gastrointestinal: A subjective improvement of diarrhea with reduced volume, frequency, and abdominal pain or the disappearance of bleeding was denominated “partial response”. The resolution of diarrhea and all other gastrointestinal symptoms was denominated “complete response”.
Statistical analysis
Data distribution was assessed using the Shapiro-Wilk test, with a p value ≤ 0.05 considered significant. The null hypothesis was assumed if the data followed a normal distribution, while the alternative hypothesis was accepted if the data did not follow a normal distribution. When the variable followed a normal distribution, it was summarized using the mean as a central tendency measure and the standard deviation as a dispersion measure. Variables without a normal distribution were summarized using the median as a central tendency measure and the interquartile range as a dispersion measure. Univariate analysis of qualitative variables was summarized as percentages.
Furthermore, the bivariate analysis was used to explore possible associations, relations, or dependence among the exposure and outcome variables (improvement of the gastrointestinal graft-versus-host disease).
When the variables were nominal dichotomous, relative risk (RR) or odds ratio (OR) were used to measure association with their respective 95% confidence intervals. Statistical tests were applied to confirm a statistically significant association depending on the variables.
Event-free survival [death, overall survival (OS), graft failure, and incidence of moderate-to-severe gastrointestinal graft-versus-host disease) was assessed using the Kaplan-Meier method.
We used the log-rank test to compare transplant and diagnosis types. Finally, exploratory analysis of the entire database was conducted using the Stata™, version 12 statistical package.
Results
During the study, 21 pediatric patients with hematopoietic stem cell transplantation and a diagnosis of steroid-refractory graft-versus-host disease were referred for an intra-mesenteric steroid injection. The mean age at the time of transplantation was 10 ± 5 years. Of these transplantations, 90.5% were haploidentical, with peripheral blood being the primary source for transplantation (62%). Most patients had a malignant disease as a primary diagnosis (57%) (table 1).
Table 1 Clinical and demographic characteristics (n = 21)
| Variable | Value n (%) | |
|---|---|---|
| Age (years) | ||
| Mean | 10 ± 5 | |
| Range (min-max) | 1-16 | |
| Sex (male) | 14 (67) | |
| Type of transplant | ||
| Matched sibling donors | 2 (9.5) | |
| Haploidentical | 19 (90.5) | |
| Transplant source | ||
| Bone marrow | 7 (33) | |
| Peripheral blood | 13 (62) | |
| Bone marrow + peripheral blood | 1 (5) | |
| Diagnosis | ||
| Malignant | 12 (57) | |
| Conditioning, n (%) | ||
| Myeloablative | 12 (57) | |
| Non-myeloablative | 9 (43) | |
Of the 21 patients, 38% required blood products before the procedure. Nineteen (90%) patients had some degree of response to the steroid injection, including a subjective decrease in fecal output and reductions in bilirubin and transaminases within the two weeks following the application (table 2).
Table 2 Characteristics and complications of intramesenteric steroid injection (n = 21)
| Variable | Value n (%) | |
|---|---|---|
| Intra-mesenteric steroid injection #1 | 21 | |
| Initial response to the procedure | ||
| Complete | 19 (90) | |
| Partial | 2 (10) | |
| Subjective decrease in diarrhea | 18 (86) | |
| Intramesenteric steroid injection #2 | 7 | |
| Response to the procedure | ||
| Complete | 6 (86) | |
| Partial | 1 (14) | |
Seven patients required a second intra-mesenteric steroid injection several weeks after the first application due to the recurrence of symptoms, with complete response in 85% of these cases (table 2).
Regarding complications related to hematopoietic stem cell transplantation, three patients experienced associated cytopenia. The overall survival rate was 67% at 100 days and 43% at 24 months (figure 2). Two of the patients were diagnosed with graft-versus-host disease in their second transplant. Out of all the patients, 12 (57%) died. Among the causes of death, seven cases were associated with infections; one was due to hemorrhagic cystitis, one was related to disease progression, and one was secondary to graft-versus-host disease (table 3).
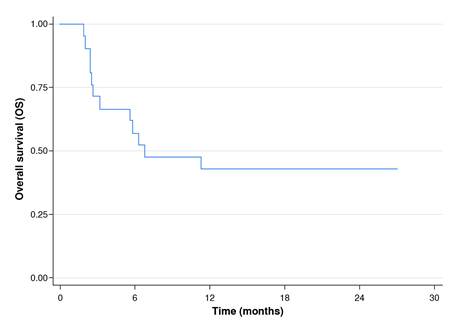
Figure 2 Overall survival in pediatric hematopoietic stem cell transplantation receptors subjected to intra-mesenteric steroid injection to treat graft-versus-host disease
Table 3 Complications related with hematopoietic stem cell transplantation (n = 21)
| Variable | Value n (%) | |
|---|---|---|
| Infection | ||
| Viral | 17 (81) | |
| Bacterial | 15 (71) | |
| Fungal | 6 (28) | |
| Parasitic | 3 (14) | |
| Veno-occlusive hepatic disease | 4 (19) | |
| Mucositis | 12 (57) | |
| Slight | 3 | |
| Moderate | 5 | |
| Severe | 4 | |
| Hemorrhagic cystitis | 9 (43) | |
| Cytopenia | 3 (14) | |
| Death | 12 (57) | |
Discussion
Mortality rates up to 90% have been reported in patients with graft- versus-host disease refractory to steroids despite using different therapeutic strategies, including etanercept, infliximab, alemtuzumab, thymoglobulin, high doses of steroids, and others 24. However, several of these medications are not broadly available and have regulatory limitations for pediatric use. High mortality is widely associated with secondary infections 25; therefore, no consensus has been established for a standard second-line treatment 9,10.
Intra-mesenteric steroid injection has proven effective in patients diagnosed with severe ulcerative colitis 26. Some authors have extrapolated their use in patients with moderate-to-severe graft-versus-host disease, given its similar pathophysiological characteristics 2.
Reports in adult populations with hematopoietic stem cell transplantation and intra-mesenteric steroid injection show an approximately 50% response rate, with a low percentage of complications; thus, some institutions have adopted this therapy as a standard second-line management 4,14. Multiple reports demonstrate its safety and efficacy 2,13,19; however, there are few cases in pediatric patients 4,20.
In this case series study, we observed similar outcomes in pediatric patients at a high-complexity institution with low rates of complications. The survival rates of patients in this study were comparable to those reported for this intra-mesenteric injection therapy 2,4. Additionally, with only one patient experiencing local complications, the rate of such complications was low and consistent with findings from other studies.
In our patients, and as described globally, there was a significant decrease in overall survival percentage within the first 100 days after transplantation. However, there were no treatment-related deaths.
According to our results, all patients reported subjective improvement in symptoms, including a reduced frequency of bowel movements and a decreasing trend in direct bilirubin and transaminases. These findings are consistent with those reported in the literature, which suggests that intramesenteric steroid injection may also improve hepatic graft-versus-host disease 2,9.
Several limitations exist in our study, including its non-randomized design, its nature as a case series, and the fact that it was conducted in a single center.
Based on our findings, we consider that intra-mesenteric steroid administration for the management of hepatic or gastrointestinal graft-versus- host disease is a feasible option and can be considered as an early adjuvant to the initial treatment in patients with moderate-to-severe refractory graft- versus-host disease. Recently, promising results have been reported with the ruxolitinib use in some patients; however, its availability is still limited 27.
Further studies are necessary in the region to gather more evidence and develop protocols for managing refractory graft-versus-host disease in pediatric patients.

