











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Studies in Latin America linking resilience with empathy are quite rare, considering that resilience may be a modulator of empathy.1) Empathy is a broad and multidimensional construct. No complete consensus exists regarding its definition.2 In general, it is possible to find two approaches about empathy: cognitive and affective. In the first, the definition is associated with adopting the cognitive perspective “about the other ", and constitutes an attempt to understand what goes on in the minds of others. The second case consists in emphasizing the affective component over the cognitive, defining it as a shared feeling (vicarious). The division into a strictly cognitive or affective empathy did not provide a satisfactory explanation with the observational findings, requiring an integrative definition of this construct.3 This situation constitutes the origin of different theories about empathy and explain, in part, the presence of several types of instruments that measure it.
There is agreement in that empathy is an attribute that permits an intersubjective connection between health professionals and patients.4 This interaction contributes positively to the development of the patient's overall care process and treatment.5 When these processes are carried out with empathy, patient care is humanized. With respect to resilience, many definitions have also been proposed. Nevertheless, no agreement has been reached regarding the concept’s essential comprehension.6 Overall, resilience may be defined as “the capacity of a dynamic system to adapt successfully to the challenges that threaten the system’s function, survival, or development”.7 The problem is that no common theoretical construct exist underlying resilience research. This concept is used in many ways in function of the area of application and of the theoretical-practical support achieved. This situation prevents obtaining a common definition of the concept and said absence hinders its objective measurement (6 and makes its operationalization difficult.
So far, there are two general approaches: by buffering and by features.8 The buffering or state approach measures resilience via a bipolar scale. The traits approach examines how individuals confront events they experience as negative and takes into account their capacity to recover.9 It must be considered that both approaches are not mutually exclusive. However, the lack of a complete theory of resilience does not permit ensuring which of the instruments can best measure this construct. The characteristics of the constructs of empathy and resilience, already described, constitute complex systems in themselves. First, between the dimensions of each system and, second, the interactions between the dimensions of a construct with respect to the dimensions of the other. Consequently, if the theoretical inference or the empirical evidence (or both) allow verifying that a deficit in any of the dimensions would result in a loss of stability of the “system” and the construct loses its essentiality.3 For example, in case of a critical deficit of the emotional dimension in empathy determines the presence of psychopathy.4 Hence, trying to establish causal relationships between empathy and resilience leads us to a problem consisting of relating two complex systems whose possible solution is also complex. In this sense, the question emerges whether resilience constitutes an independent variable in relation with empathy. Various studies start with the work hypothesis consisting in that empathy can be modulated directly by resilience or conclude, with empirical evidence, that effectively resilience modulates and can predict empathy or resilience acts as mediator between another factor and empathy 10. Consequently, it is inferred theoretically and with certain empirical evidence that the formation of empathy in nursing students cannot be conducted in separate manner from the training in resilience.
Based on these antecedents, the aim of this work was to determine if resilience can predict empathy. If it does, explain what would be the effect (overall) of the dimensions of resilience over the dimensions of empathy in the nursing students examined in the study herein.
Methods
Population and sample. The population corresponded to Nursing students in the Faculty of Health Sciences at Corporación Universitaria Rafael Núñez in Cartagena de Indias, Colombia. The sample was made up by all the nursing students registered in the Faculty of Health Sciences who accepted voluntarily to participate in this research and who were taking classes on the moment of the application of the instruments. The nursing student population consisted of 371 students, with 340 being evaluated, representing 92% of the total. The sample included 46 men and 294 women (13.5% and 86.5%, respectively, of the total sample). The ages of the nursing students had a mean of 22 years (SD = 4.75).
Instruments. (i) Jefferson Empathy Scale for Health Professionals, student version (JSE-HPS).11 this instrument measures the levels of empathy with Health Sciences patients, in general, and it has 20 items. The questions are constructed in a Likert-type scale with responses numbered from 1 to 7, where 1 means totally disagree and 7 totally agree. It comprises three dimensions or underlying variables: Compassionate Care (CC); Adoption of the Patient’s Perspective (PA); and Walking in the patient’s shoes (WIPS). This instrument has demonstrated internal consistency (α > 0.80), cultural and structural validity (CFI = 0.925; TLI = 0.914; RMSEA = 0.048) and it is one of the most used to measure non-pathological levels of empathy in students with patients. (ii) Resilience-Trait Scale (RTS),12 which is structured by three dimensions: Engineering (4 items), Ecological (4 items), and Adaptative (4 items). It has a Likert-type format with 12 items, with five response levels per item, going from totally disagree to totally agree. The RTS has shown adequate reliability (α > 0.85), a cross-culturally stable factor structure (CFI = 0.95; TLI = 0.94; RMSEA = 0.075; SRMR = 0.06), construct and convergent validity in terms of associations with personality, and a positive contribution to clinical and non-clinical states of psychological health.13
Data collection procedure. Data were collected by non-participating professors, duly trained for the application, belonging to the Faculty of Health Sciences at the Corporación Universitaria Rafael Núñez in Colombia. The informed consent, together with the instrument used to measure empathy and resilience, was administered and signed on paper format and during the hours before or after the professors taught their classes. The data were tabulated in an Excel spreadsheet by administrative staff in the Faculty of Health Sciences who had been trained for this purpose.
Data analysis. The data analysis used a structural equations model (SEM). The robust maximum likelihood (RML) estimator was used, and the comparative fit index (CFI) (>0.95), the Tucker-Lewis Index (TLI) (>0.95), the root mean square error of approximation (RMSEA) (<0.08), and the standardized root mean square (SRMR) (<0.08) were used to evaluate the fit of the proposed model. Regarding the measurement models, a confirmatory factor analysis (CFA) was performed using the RML estimator, and the same fit indicators were considered as in the SEM. A p value <0.05 was considered to estimate a result as significant. IBM SPSS 27 was used to calculate descriptive statistics, and R in its RStudio environment for the CFA, using the Lavaan package (0.6-18) and semTools (0.5-6) packages. To determine reliability, Cronbach's alpha and McDonald's omega coefficients were used.
Ethical aspects. This research is part of a Project that studies empathy in Latin America. The project that supports this research was approved by the Institutional Bioethics Committee at Universidad Andrés Bello (Chile), Approval Minutes No. 020/2022. The participants signed the informed consent prior to starting the study.
Results
Empathy Scale. It was found that the empathy scale has adequate indices of fit to the data (χ2 = 269.62; gl = 167; p < 0.001; RMSEA = 0.046 [90%CI 0.035 - 0.057]; CFI = 0.94; TLI = 0.94; SRMR = 0.061), evidencing that the instrument shows validity based on the internal structure. It also demonstrated adequate reliability levels in all its dimensions: Adoption of the perspective (ω = 0.85; α = 0.85), Compassionate Care (ω = 0.83; α = 0.83), and Placing themselves in the patient’s shoes (ω = 0.69; α = 0.69). The factorial structure of the scale has shown evidence of being strictly invariant according to the sex of the participants, in the sequence of invariance models proposed: metric (ΔCFI = 0.000; ΔRMSEA = -0.001), scalar (ΔCFI = -0.004; ΔRMSEA = 0.000), and strict (ΔCFI = -0.010; ΔRMSEA = 0.002) invariance.
Resilience Scale. With respect to the resilience scale, it was found that this instrument shows strong evidence in favor of validity based on the internal structure (χ2 = 83.64; gl = 51; p = 0.003; RMSEA=0.053 [90%CI 0.030 - 0.073]; CFI=0.97; TLI=0.97; SRMR =0.046). Additionally, it evidenced adequate reliability levels in all its dimensions: Engineering (ω = 0.88; α = 0.88), Ecological (ω = 0.84; α = 0.84), and Adaptative (ω = 0.73; α = 0.72). Moreover, The factorial structure of the scale has shown evidence of being strictly invariant according to the sex of the participants, in the sequence of invariance models proposed: metric (ΔCFI = -0.003; ΔRMSEA = -0.001), scalar (ΔCFI = 0.000; ΔRMSEA = -0.003), and strict (ΔCFI = 0.002; ΔRMSEA = -0.005). All these results show that both measurement models (empathy and resilience) are adequately represented and are suitable for the structural model.
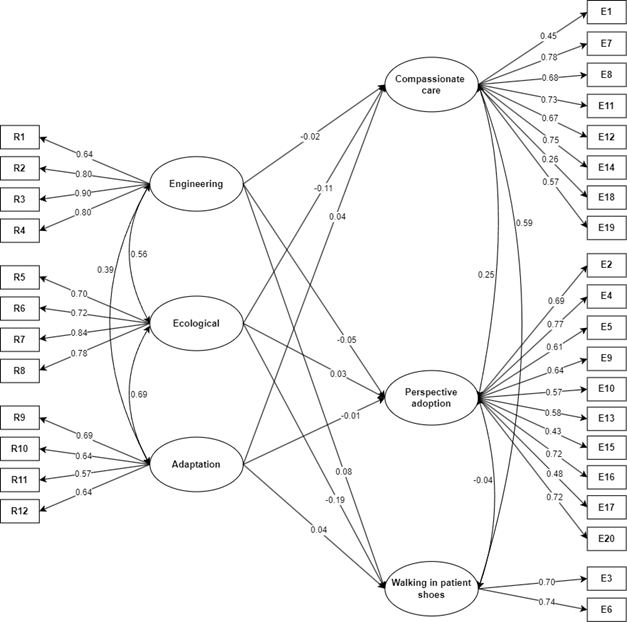
Explanatory model. This study evidenced that the structural model has adequate fit indices (χ2 = 651.17; gl = 449; p < 0.001; RMSEA = 0.038 [90%CI 0.031 - 0.045]; CFI = 0.95; TLI = 0.94; SRMR = 0.043). Figure 1 shows that the Engineering dimension managed to predict positively the dimension “walking in the patient’s shoes” (β = 0.08). Regarding the Ecological dimension, it is noted that it predicts negatively the dimensions “Compassionate Care” (β = -0.11) and “walking in the patient’s shoes” (β = -0.19) of empathy. The Adaptive dimension did not manage to predict the empathy components in nursing students.
Discussion
The results of the reliability tests, factorial structure of the data, adjusted to the underlying three-factor model, and invariance in the two constructs studied were all found satisfactory. The fact that the psychometric premises are met indicates that there are no biases derived from the measurement models, thus, it is possible to trust the results.
From the theoretical point of view, Ecological Resilience is characterized by the system’s ability to withstand an alteration, before applying the capacities that allow reordering the psychological procedures and "mechanisms" that will subsequently enable recovery of the stable state in relation to the functional structure and identity of the system that existed prior to the disturbance. Hence, Ecological Resilience focuses on the fact of “understanding the nature and magnitude of the disturbance nursing students will have to resist and absorb. The negative prediction of Ecological Resilience about the CC and WIPS dimensions observed could be the consequence of the confrontation of a disturbance caused by a deficiency in the capacity to resist it: negative coping. This situation would lead to a lack of emotional connection with the patient and, simultaneously, reduce the ability to understand what the patient thinks and feels. In this sense, the effect of “empathic erosion”3 in nursing students is known as a result of their role in patient care and the responsibility they assume, adding, the academic load itself, among other factors. Thereby, students undergo a complex adjustment14 due to existing exogenous and/or endogenous pressures, which can persist discretely throughout their career. Within this context, when coming into contact with patients in the clinical area, these pressures are even greater.15 Existence of factors influencing upon this adjustment has been proposed:16 emotional regulation, self-concept, meaning of life and depression,17-20 burnout and self-efficacy,21,22 among others.
These antecedents and, considering that this research is cross-sectional and does not account for the dynamics of the phenomenon over time, the existence of decreased CC levels - due to the lack of or deficiency of the necessary traits to confront, resist, and absorb the disturbance, could constitute only a snapshot of the relationship between resilience and empathy in the sample studied, but in the absence of a well-founded empathic intervention,13,14 This deficit could remain active in the remaining process of these students' training, with the relevant consequences. The deficit could be explained by the focus and effort students make to resist and absorb the disturbances derived from the health status (severity of the disease) of the patients whom they could care for daily without the necessary mechanisms to successfully cope and they do so at the expense of being emotionally affected. This situation could become one of the mechanisms that could explain, in part, the presence of empathic erosion.
It could also happen that, besides the aforementioned focus, diminished emotionality (CC) might be associated with a possible preexistence of a deficit in emotional regulation that would affect the ability to understand the subjectivity of the patient’s thinking (WIPS), but without affecting the patient’s capacity for intellectual comprehension (PA). Engineering resilience (ER), however, predicts a slight WIPS increase. A likely explanation is that the traits associated with this engineering dimension enhance the ability to regain balance in the students in the sample, but said effect would occur after the students were able to resist and absorb the disturbance. Thus, these results propose that the nursing students examined would have a low threshold to withstand exogenous or endogenous disturbances, but a certain capacity to recover from the initial disturbing impact upon resolving the ecological stage of resilience.
Despite the strengths of this work, it is pertinent to consider some limitations; for example, these types of studies must consider that the possible relationship (prediction) of a construct, like resilience over empathy, cannot fully explain the observed empathic response, given the empirical evidence and theoretical reasons that empathy could be the “product” of the influence of several independent factors or modulators of empathy.3,12-14,23 This situation must necessarily imply predictive estimations with relatively low values. In this context, obtaining high prediction values could be considered “suspicious” of a biased evaluation. Further, statistical significance should not be taken as a “gold standard” in these types of research processes. Inferring that data analysis only seeks to find “significant” or “insignificant” results may represent a typical case of reductionism.24 Consequently, the fact that no statistical significance was found could not be interpreted as a result of low interest given the foregoing. In the context of results with complex variables (empathy and resilience), it is possible to find insignificant values more often than expected; however, these may have an association strength that must be considered based on the nature of the object being analyzed, as is the case with the complex variables in this study.25
The findings observed in this study permit concluding that empathy is not an independent attribute and that it can be predicted from resilience. Therefore, the positive development of empathy formation also depends, in part, on the development of resilience in the students examined. The teaching-learning processes that involve empathy formation must necessarily be intertwined with the formation of resilience.

