











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
INTRODUCTION
The nervous system plays an integral role in the human body, and its interactions with other systems are crucial for maintaining overall health. When the nervous system is compromised, it can lead to a myriad of symptoms that can be difficult to diagnose. Although neurological symptoms are often associated with primary nervous system disorders, they can also be caused by systemic diseases that affect other organs in the body. As such, it is essential to understand the complex relationships that exist between the nervous system and other organ systems to provide an earlier diagnosis and effective treatment for patients exhibiting neurological symptoms. This review focuses on how diverse cardiac, gastrointestinal, endocrine, and other conditions manifest in the neurological system. Figure 1 summarizes key neurological manifestations related to the systemic diseases mentioned in this paper.
The review was conducted by researching academic articles published in the past 20 years in leading online databases such as MEDLINE, Embase, Scopus, Science Direct, Scielo, and Google Scholar. It included different types of studies published in English and Spanish, including systematic reviews, meta-analyses, review articles, case reports, and observational studies, as well as articles identified through bibliographic references. The search utilized terms such as neurologic or neurological manifestation and systemic diseases, renal disease, cardiac disease, hepatic disease, rheumatology disease, endocrine disease, and gastrointestinal disease.
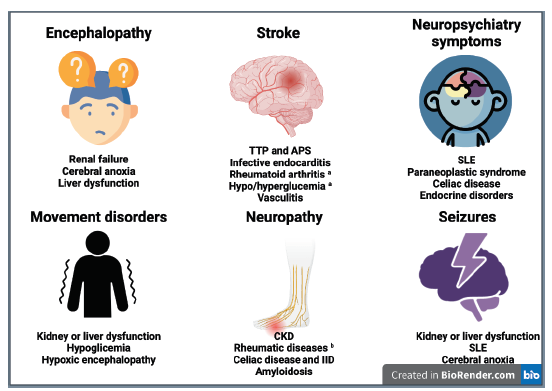
Source: self-made
a Stroke-like (acute focal deficits)
b Mainly Sjögren syndrome, ANCA vasculitis, SLE and RA.
APS: antiphospholipid syndrome; CKD: chronic kidney disease; IID: inflammatory intestinal disease; RA: rheumatoid arthritis; SLE: systemic lupus erythematosus; TTP: thrombotic thrombocytopenic purpura.
Figure 1 Key neurological manifestations of selected systemic diseases.
KIDNEY DISEASES
1. Renal Failure
Neurological involvement in chronic kidney disease (CKD) has a slow progression, while in acute kidney failure and acute decompensation of CKD, changes are more accentuated [1].
Initial symptoms are nonspecific and fluctuating; these include fatigue, apathy, irritability, headache, and altered states of consciousness that change throughout the day. Afterwards, emotional lability, personality changes, sleep disorders, and memory impairment appear.
Advanced stages manifest with delirium, hallucinations, stupor, and coma [1]. Always bear in mind the possibility of renal encephalopathy in a patient with kidney disease who develops fluctuating consciousness or cognitive impairment.
Cognitive deficits can occur in up to 80% of the patients with CKD, and they manifest with memory and executive function disorders, such as problem-solving or calculating difficulties [2]. Movement disorders can also be seen and include tremor, restless legs syndrome, asterixis, paratonia (semi-voluntary increase in muscle tone), and multifocal myoclonus [3]. A third of the patients can present with focal, generalized, and non-convulsive epileptic seizures, particularly in patients that develop posterior reversible encephalopathy syndrome (PRES) [4]. Sixty percent of the patients develop polyneuropathy with pruritus, dysesthesias, impaired vibration, and temperature sense, hyporeflexia, distal weakness, and autonomic symptoms [5].
Dialysis disequilibrium syndrome is a complication that occurs in patients undergoing renal replacement therapy, typically presenting at the end of dialysis, and resolving within a few hours. It is more common in first-time dialysis patients, or in those who skip sessions [1].
2. Microangiopathy
Around 60% of patients with thrombotic thrombocytopenic purpura experience initial neurological symptoms such as headache, confusion, focal deficits, seizures, and coma [6]. Hemolytic uremic syndrome is characterized more by renal compromise rather than neurological symptoms (25%-30%), with patients presenting with lethargy, irritability, seizures, and, less frequently, focal deficits, cortical blindness, and coma [7]. PRES can be present in both diseases and should be considered when a patient with kidney failure develops acute neurological symptoms and has fluctuating blood pressure, a history of cytotoxic drug use, autoimmune alterations, or pre-eclampsia-eclampsia [4].
RHEUMATIC DISEASES
1. Systemic Lupus Erythematosus (SLE)
Neuropsychiatric manifestations can occur in 28-40% of patients, either before or at the time of diagnosis, and it usually manifest as a first psychotic episode in patients without a psychiatric history [8]. Other central nervous system (CNS) symptoms could be attributed to SLE, complications derived from therapy, or coexisting pathologies such as antiphospholipid syndrome. These symptoms include headache (37%), mood disorders (15%), cognitive dysfunction (23-60%), seizures (8%), and cerebrovascular diseases (CVD) (7%). Involvement of the peripheral nervous system (PNS) is less frequent, and it can manifest as symmetric or asymmetric distal sensorimotor neuropathy, cranial neuropathy, or mononeuritis multiplex [12].
2. Rheumatoid Arthritis (RA)
In advanced stages of RA, involvement of the cervical spine is common. This can lead to atlanto-axial or subaxial subluxation resulting from the inflammatory process. While it is usually asymptomatic, it may present with occipital pain, stiffness, and loss of cervical lordosis [10]. Vertical subluxation can lead to low cranial nerve involvement, paresthesia, and pyramidal syndrome [10]. Although infrequent, CNS involvement can also manifest as psychiatric disorders, cognitive dysfunction, depression, anxiety, headache, an increased risk of epilepsy, and, in rare cases, aseptic meningitis, or stroke-like episodes [9]. Neuropathy is common, occurs in 20% of patients, and can present as entrapment (such as carpal tunnel syndrome), mononeuritis multiplex, or senso-rimotor distal neuropathy [9,10].
3. Sjögren Syndrome (SS)
Neurological involvement occurs in 20% of cases with SS, and it typically appears before the onset of xerostomia and xerophthalmia [9, 11]. PNS involvement is quite common and should always be suspected in patients with SS and sensory symptoms. Symmetric-sensitive polyneuropathy manifests with paresthesia in the lower limbs, loss of sensitivity, and hyporeflexia [11]. Other forms of PNS involvement include sensorimotor polyneuropathy, multiple mononeuropathy, sensory ganglionopathy, small fiber neuropathy, cranial neuropathy, myositis, and autonomic alterations. CNS involvement is less frequent and includes cognitive alterations, meningitis, symptoms like multiple sclerosis, optic neuritis, and transverse myelitis [9,11].
4. Systemic Sclerosis and Scleroderma
In localized scleroderma, there is often significant muscular involvement (90%), and nearly half of patients with coup de sabre present epileptic seizures with altered consciousness that may progress to bilateral tonic-clonic seizures [12]. Neurological manifestations of systemic sclerosis include epileptic seizures, depression, anxiety, headaches, cognitive decline, peripheral sensorim-otor neuropathy, carpal tunnel syndrome. Systemic sclerosis should be suspected in patients with bilateral trigeminal neuropathy [12].
5. Mixed Connective Tissue Disease
The CNS involvement in mixed connective tissue disease is like that of SLE. Around 10-17% of patients may present with neuropsychiatric manifestations such as psychosis. Other neurological manifestations are trigeminal neuropathy, headaches, aseptic meningitis, epileptic seizures, peripheral neuritis, and cerebrovascular disease [13].
6. Vasculitis
The neurological manifestations of systemic vasculitis are summarized in Table 1. Non-systemic vasculitic neuropathy (organ-specific vasculitis) is not a rare form of vasculitis and most often presents as multiple mononeuritis, distal symmetric polyneuropathy, or pure sensory neuropathy [14]. Vasculitis should be suspected in any patient with multiple mononeuritis or polyneuropathy that begins insidiously and with progressive involvement of different territories [15].
Table 1 Systemic vasculitis [19]
| Vasculitis | Neurological Manifestation |
|---|---|
| Takayasu Arteritis | Dizziness, blurred vision, headache, ischemic stroke, PRES |
| Giant cell arteritis | Headache, ophthalmoplegia, mandibular claudication, ear pain, vision loss |
| Polyarteritis nodosa | Great PNS involvement: mononeuritis multiplex and symmetric polyneuropathy |
| Granulomatosis with polyangiitis | Mononeuritis multiplex Cranial neuropathy (I and II) Headache |
| Eosinophilic granulomatosis with polyangiitis | Asymmetric painful sensory polyneuropathy Mononeuritis multiplex |
| Microscopic polyangiitis | PNS compromise in up to 50%: mononeuritis multiplex, symmetric polyneuropathy, or pure sensory neuropathy |
| Behçet Disease | Headache, cognitive deficit, behavior changes |
Source: self-made
PRES: Posterior reversible encephalopathy syndrome; PNS: peripheral nervous system.
7. ANTIPHOSPHOLIPID SYNDROME (APS)
Headache is the most common manifestation, with migraine being the most prevalent type (20%). CVD is the most severe and frequent complication, particularly in young patients. In some cases, venous sinus thrombosis can cause headache, nausea, focal deficit, seizures, and intracranial hypertension, as well as reversible cerebral vasoconstriction syndrome (RVCS) with thunderclap headaches [16]. APS should be suspected in young patients with CNS arterial or venous thrombosis without risk factors or genetic causes. Ocular syndromes, such as amaurosis fugax, occur in 15-88% of cases. Other manifestations include cognitive deficits, seizures, syndromes like multiple sclerosis, and psychiatric syndromes [17]. PNS involvement is rare.
ENDOCRINE DISEASES
1. Pituitary/hypothalamic Disorders
Hypopituitarism typically presents with asthenia, apathy, and decreased cognitive function. Functional adenomas can cause Cushing's disease with myopathy, behavioral changes, or acromegaly with apathy, depression, and sleep apnea/hypersomnia [18].
Pituitary apoplexy commonly presents with thunder retro orbital headaches (80%) and visual symptoms such as decreased visual acuity, visual field defects, and ophthalmoplegia [19]. Other symptoms may include fever, nausea, vomiting, altered consciousness, and meningeal signs [20]. In diabetes insipidus, the development of hypernatremia can lead to encephalopathy [21]. Always suspect diabetes insipidus in a critically ill patient that develops excessive thirst.
2. Adrenal Disorder
Neurological manifestations of adrenal insufficiency are nonspecific and can include neuropsychiatric symptoms such as depression, apathy, or delirium. Some patients may also experience muscle pain and weakness, as well as symptoms of intracranial hypertension like headaches. In cases of adrenal crisis, patients may develop seizures, severe encephalopathy, and myopathy [22]. Adrenal hyperfunction, such as Cushing's syndrome, can lead to intracranial hypertension, encephalopathy, and mood disorders such as mania-depression, insomnia, anxiety, and psychosis, along with associated myopathy [23]. Pheochromocytoma can cause explosive headaches, anxiety, psychosis, cognitive decline, tremors, and seizures [24].
Patients with neuropsychiatric symptoms who are young are frequently misdiagnosed with primary psychiatric illnesses or conversion/somatization syndromes. It is important to consider endocrine disorders as a possible cause of atypical psychiatric symptoms, especially in patients without known risk factors or with unexplained systemic symptoms.
3. Hypothyroidism and Myxedema Coma
Neurological complications of hypothyroidism can develop gradually and may initially present as cognitive impairment, neuromuscular deficits, or headache, with fatigue, apathy, drowsiness, and lack of concentration being common [26]. Hypothyroidism should always be ruled out in elderly patients with a recent onset of cognitive decline.
In myxedema coma, myopathy can cause weakness, slow contraction, and relaxation (pseudomyotonia), asthenia, and fatigue. Other symptoms may include hearing loss and hoarseness [25]. The most severe cases can result in hypothermia and altered consciousness, with delirium, stupor, or coma [26]. Additional symptoms can include cerebellar signs and seizures [27].
4. Hyperthyroidism and Thyroid Storm
Thyrotoxicosis may often present with symptoms of motor restlessness such as akathisia, postural tremor, as well as psychiatric symptoms including anxiety, insomnia, mania, and less frequently seizures [27]. In elderly patients, it may present in the opposite way, with lethargy, stupor, or coma, which is known as 'apathetic hyperthyroidism'. In Grave-Basedow disease, ophthalmoplegia may appear and the involvement of the optic nerve is usually late [28]. Some patients may manifest neuromuscular disorders such as myopathy, periodic paralysis, and neuropathy, which often manifest insidiously.
In thyroid storm, encephalopathy commonly presents as agitation, emotional lability, confusion, paranoia, psychosis, and eventually coma. Additionally, cases of patients with epileptic status and cardiovascular disease have been reported [29].
5. Hyperglycemia
One neurological complication of diabetic ketoacidosis are cerebral edemas. Headache is one of the first symptoms, followed by rapid deterioration including lethargy, seizures, pupillary changes, respiratory distress, and manifestations of intracranial hypertension such as papilledema, high blood pressure, and bradycardia [30]. In hyperosmolar crisis, three neurological conditions can be recognized: focal deficits with crisis in the form of continuous focal seizure (epilepsia partialis continua), hemicorea/hemiballismus syndrome, and stupor/coma without neurological focus [31]. Always assess serum or capillary glucose in patients with focal deficits (stroke-like) or acute-onset abnormal movements.
In diabetes, it is common to have both PNS and autonomic involvement. The most frequent form is distal symmetric polyneuropathy, while other manifestations include cardiac autonomic neuropathy, gastrointestinal dysmotility, and impotence. Focal neuropathies, such as isolated mononeuropathies, radiculopathy, or polyradiculopathy, are less common but may also occur. In the CNS, diabetes is associated with stroke and cognitive impairment. Due to the complexity of the underlying mechanisms and the extensive manifestations of diabetic neuropathy, a detailed review is beyond the scope of this article, and we recommend further reading for a more comprehensive understanding. [32].
6. Hypoglycemia
In hypoglycemia, initial neurologic symptoms can include dizziness, fatigue, visual disturbances, and cognitive changes such as irrational and erratic behavior. If left untreated, hypoglycemia can lead to seizures and coma. In rare cases, hypoglycemia can cause focal neurologic deficits that mimic symptoms of stroke, so the previous advice for measuring serum or capillary glucose stands [33].
CARDIAC AND PULMONARY DISEASE
1. Ischemic and Hypoxic Encephalopathy
In cases of global cerebral ischemia, the first symptom is typically a change in consciousness, which can progress to coma after more than 4 minutes of hypoxia. Subsequently, decorticate or decerebrate postures, myoclonus, and seizures may appear [34].
Cerebral anoxia can lead to different movement disorders, including action myoclonus (Lance-Adams syndrome), parkinsonism, chorea, dystonia, ataxia, and seizures. Late hypoxic enceph-alopathy may develop after apparent recovery from cerebral anoxia. Symptoms such as listless-ness, confusion, irritability, occasional agitation, or mania may appear over a period of one to four weeks and may persist in a minority of patients [34].
2. Pulmonary Encephalopathy
Unspecific signs, such as headache, attention deficits, drowsiness, and cognitive deficits, may appear in chronic obstructive pulmonary disease (COPD) and cases of alveolar hypoventilation. If left untreated, these signs can progress to psychomotor agitation, nocturnal delirium, and ultimately confusion and coma in states of sustained hypercapnia [35]. Additionally, in some cases, asterixis and myoclonus may occur [35].
Around two years after resuscitation, approximately half of the patients who develop acute respiratory distress syndrome (ARDS) may experience neurocognitive disorders, including emotional disorders, anxiety, apathy, depression, and exacerbation of painful phenomena [36].
3. Infective Endocarditis
Neurological complications occur in 15% to 47% of patients with endocarditis. Among these, strokes are the most frequent and can be the initial presentation in about 20% of cases [37]. While most of these strokes are ischemic, subarachnoid, or intracerebral hemorrhages can also occur due to septic endarteritis, hemorrhagic transformation from an ischemic infarction, or rupture of a fungal aneurysm [38].
In young patients with risk factors for bacteremia who develop acute neurological deficits, it is important to always keep a high suspicion of septic embolism. This is because septic embolism can result not only in strokes but also in the direct infection of the central nervous system, potentially leading to meningoencephalitis, cerebritis, or abscess formation. These conditions can be recognized by the appearance of meningeal signs and sensory/motor deficits [37].
4. Aortic Dissection
Neurological complications occur in 25% of patients with aortic dissection [39]. In a small percentage of patients, neurological manifestations may be the initial finding or may be preceded by chest pain and eventually lead to the diagnosis of an extensive arterial dissection. Ischemic stroke is the most common neurological complication associated with type A dissections, but other potential complications include Horner syndrome (when the dissection extends to the carotid artery), left recurrent laryngeal nerve palsy, and spinal cord ischemia [40].
GASTROINTESTINAL DISEASES
1. Hepatic Encephalopathy (HE)
HE is a neurological complication that can occur in patients with liver dysfunction, particularly in those with cirrhosis. The initial and mild stages form of the disease may go unnoticed due to subtle manifestations that include changes in mental state, attention, and behavior. There are mainly two forms of presentation: acute and chronic encephalopathy. Acute encephalopathy is characterized by acute recurrent confusion episodes, while the chronic form, also known as non-wilsonian hepatocerebral degeneration, is characterized by cognitive decline and motor disorders such as parkinsonism, chorea, dystonia, asterixis, and myelopathy [41].
In patients with cirrhosis, mild HE with minimal changes occurs in 20% to 80% of the cases, and the main symptoms include work-related memory impairment and executive function impairment [42]. Always consider HE in a patient with liver disease or risk factors who develops fluctuating consciousness or cognitive impairment.
2. Celiac Diseases and Gluten Sensibility
Neurological dysfunction can be present in up to 22% of the patients, even without clear gastrointestinal symptoms [43]. Many symptoms are related to vitamin deficiencies (B1, B12, B6, E, B2, and B3), including cognitive decline, behavior disorders, attention deficit, chronic headache, and seizures. 33% of patients can develop distal symmetric peripheral neuropathy [44].
Other manifestations include myelopathy, cerebellar ataxia, and restless legs syndrome [43].
3. Intestinal Inflammatory Disease
The incidence of neurological complications in Crohn's disease and ulcerative colitis patients ranges from 0.25% to 37%. The most common neurological complication is axonal peripheral neuropathy. Both Crohn's disease and ulcerative colitis can present with focal or diffuse myositis before the onset of gastrointestinal symptoms. Due to a secondary deficiency of vitamin B12, progressive myelitis can be observed. Furthermore, patients with these diseases are at a higher risk for autoimmune events such as multiple sclerosis and CNS vasculitis [45].
OTHER DISEASES:
1. Sarcoidosis
Around 10% patients have neurological manifestations, 15% without systemic manifestation. Half of these patients develop cranial neuropathy, with the facial, optic, and vestibulocochlear nerve being the most affected. It is not uncommon for patients to also present with aseptic meningitis, acute encephalopathy, and hypothalamic dysfunction. Other neurological manifestations of sarcoidosis include myelopathy, myopathy, peripheral neuropathies with mononeuritis multiplex and Guillain-Barré syndrome [46].
2. Amyloidosis
Neuropathy is the most common neurological manifestation of light chain amyloidosis, affecting both small and large nerve fibers. Patients typically report paresthesia and burning pain in the lower limbs, which progresses to impairment of vibration and proprioception [47]. Facial cranial neuropathies and plexopathies have also been reported, and 65% to 75% of patients experience autonomic dysfunction, including diarrhea, postural hypotension, gastroparesis, and erectile dysfunction [48]. Hereditary forms of amyloidosis could manifest as familial bilateral carpal tunnel syndrome in patients without risk factors or comorbidities.
3. IgG4-related Disease
There is usually involvement of the orbit, pachymeningitis, hypophysis, and peripheral nervous system. The orbital disease is characterized by progressive chronic lacrimal gland and periorbital edema, which can progress to palpebral ptosis and diplopia. Meningeal impairment causes symptoms of intracranial hypertension and cranial neuropathy. Hypophysis involvement is associated with decreased libido, hypogonadism, hypothyroidism, and hypoadrenalism [49].
4. Lymphoma
About one-third of patients have some involvement of the nervous system. When the tumor directly invades the nervous system, symptoms depend on the location of the tumor and may include focal deficits, seizures, meningitis, intracranial hypertension, and syndrome of inappropriate antidiuretic hormone secretion. Indirect nervous system complications include paraneo-plastic syndromes. Subacute encephalitis could cause personality changes, seizures, psychosis, behavioral alterations, and sleep disturbances, while cerebellar degeneration could lead to symptoms such as ataxia.
Hypercoagulability complications, such as arterial and venous thrombosis can present with focal deficits and headaches. When the PNS is involved, it typically manifests as cranial neuropathy or lumbar radiculopathy. It is always crucial to consider other potential complications in the CNS and PNS that may be associated with chemotherapy or radiation therapy [50].
CONCLUSIONS
The nervous system can be affected by various conditions, including gastrointestinal, endocrine, rheumatic, lung, kidney, and heart diseases, among others. As a result, neurological symptoms are commonly seen in clinical practice due to systemic diseases, and conversely, common systemic diseases can frequently cause neurological manifestations. Therefore, it is crucial to keep in mind that a wide range of potential diagnoses should be considered when approaching neurological symptoms and signs. This approach can lead to an earlier diagnosis and more effective treatment for patients experiencing neurological symptoms.

