











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Parkinson's disease (PD) is a progressive neurodegenerative disorder classically associated with motor symptoms, including bradykinesia, tremor, and rigidity. However, beyond these motor manifestations, PD is increasingly recognized for a wide range of non-motor symptoms that contribute substantially to overall disease burden. Over the past three decades, PD has become the fastest-growing neurological condition globally, affecting approximately 5-7.3% of individuals over the age of 65 1. The neuropatho-logical hallmarks of PD include the degeneration of dopaminergic neurons in the substantia nigra pars compacta, resulting in striatal dopamine depletion, along with the presence of intracellular α-synuclein aggregates forming Lewy bodies 2.
Non-motor symptoms can appear during the prodromal phase, preceding the onset of classical motor signs, and persist throughout the disease course 3-5. These symptoms encompass a broad spectrum, including neuropsychiatric disturbances, cognitive decline, autonomic dysfunction, sleep disorders, and sensory-perceptual abnormalities. The most common non-motor symptoms and features in PD are shown in Figure 1. Recognizing their clinical relevance, the Movement Disorder Society (MDS) diagnostic criteria for PD incorporate olfactory loss as a supportive criterion, while also considering the absence of common non-motor features beyond five years of disease as a red flag 6.
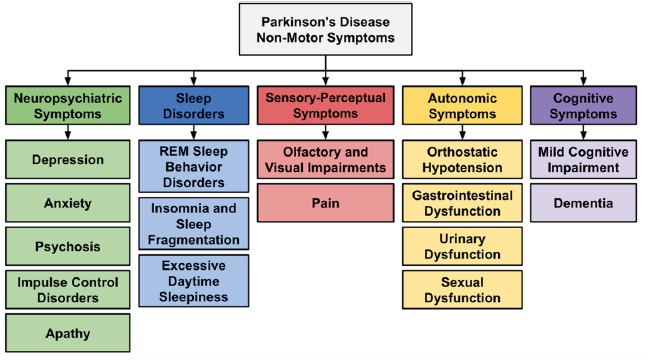
Source: Own elaboration.
Figure 1 Most common non-motor symptoms and features in Parkinson's disease
The underdiagnosis of non-motor symptoms, due to gaps in their assessment and treatment, leads to poor disease control, diminished quality of life, and complications at various stages of the disease 7. A thorough understanding of non-motor symptoms is therefore essential for accurate diagnosis, timely therapeutic intervention, and the development of comprehensive, individualized care strategies. This review synthesizes current evidence on the clinical presentation, assessment, and management of nonmotor symptoms in PD, underscoring their critical role in shaping patient outcomes.
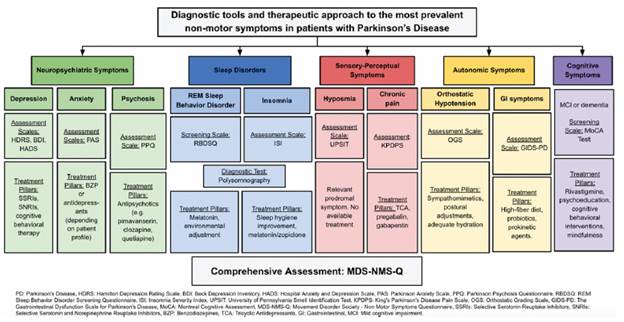
Figure 2 provides an overview of the most commonly used diagnostic tools and therapeutic approaches for the most prevalent non-motor symptoms in patients with PD.
Materials and methods
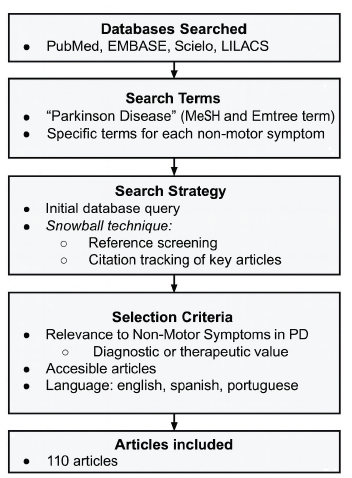
A comprehensive literature search was conducted using PubMed, EMBASE, and SciELO databases. The search strategy combined Medical Subject Headings (MeSH), Emtree terms, and relevant free-text keywords, including "Parkinson Disease" and specific terms for each non-motor symptom, such as "Depression", "Anxiety", "Psychosis", "Disruptive, Impulse Control, and Conduct Disorders", "Apathy", "Sleep Wake Disorders", "Dyssomnias", "REM Sleep Behavior Disorder", "Sensation Disorders", "Pain", "Autonomic Nervous System Diseases", "Hypotension, Orthostatic", "Gastrointestinal Diseases", "Urinary Bladder, Neurogenic", "Urinary Incontinence", "Sexual Dysfunction, Physiological", and "Cognitive Dysfunction". The complete systematic search strategy, separated by database and organized by each group of non-motor symptoms, is detailed in Appendix A.
An initial set of studies was identified through database queries, and additional relevant literature was retrieved using a snowball approach, which involved screening the reference lists of selected articles and tracking citations of key publications.
Studies were included if they addressed the prevalence, assessment, diagnosis, clinical impact, or management of non motor symptoms in PD, regardless of study design. Selection was based on the authors' criteria, not systematically. Articles published in English, Spanish, and Portuguese were considered eligible. Studies focusing only on motor manifestations or unrelated topics and without full-text access or available only in abstract form were excluded.
A total of 110 studies were selected according to the mentioned criteria, based on their relevance to non-motor symptomatology in PD and their contribution to understanding its clinical implications and therapeutic approaches. The quality of the included studies (grouped by subsection) was stratified according to the Oxford Centre for Evidence-Based Medicine classification and is detailed in Appendix B. The flowchart outlining the search strategy is presented in Figure 3.
1. Neuropsychiatric symptoms
1.1 Depression
In PD, depression manifests in subtypes such as minor depression, dysthymia, and others 8,9. Major depressive disorder affects approximately 17% of PD patients, minor depression 22%, and dysthymia 13% 10. While numerous studies have addressed depression in PD, many patients exhibit depressive symptoms without meeting the criteria for a specific depressive disorder 11. Subsyndromal depression in PD includes excessive pessimism, rumination, and hopelessness, which are common in this condition 12. Anxiety often coexists with depressive disorders, requiring thorough evaluations in PD patients. These symptoms can emerge during the prodromal stages and tend to worsen in advanced stages 13. Depression is the most common neuropsychiatric symptom prior to diagnosis 14 and is associated with non-motor fluctuations during "off" periods in PD 13,15.
Evaluating depression in PD is challenging due to overlapping symptoms 8, emotional responses to diagnosis, and medication side effects 16. Early assessment in primary care is crucial, with tools such as the Hamilton Depression Rating Scale, Beck Depression Inventory, and Hospital Anxiety and Depression Scale aiding in screening depressive symptoms in PD. Non-pharmacological interventions such as cognitive-behavioral therapy (CBT) and aerobic exercise have shown utility 17,18. Pharmacological options include selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), and tricyclic antidepressants (TCAs), each with varying efficacy and side-effect profiles 16,19. SNRIs are considered the safest option for depressive symptoms but do not improve other PD symptoms 16,19. Medications like pramipexole (dopamine agonist), primarily used for motor symptoms, may also benefit patients with specific depressive symptoms 20. First-line pharmacological management recommendations include SSRIs or SNRIs at standard doses, with regular evaluations for efficacy and adverse effects 21.
1.2 Anxiety
Anxiety is characterized by excessive worry and distress, which may become pathological in the absence of a clear stimulus. According to the DSM-5, while anxiety symptoms are common and may be transient, an anxiety disorder is diagnosed when these symptoms are persistent, excessive, and cause significant impairment in social, occupational, or other important areas of functioning, which may occur in PD 9,22. Anxiety symptoms are common in PD patients 22 and can manifest as generalized anxiety disorder (apprehension, fear, worry), separation anxiety disorder, selective mutism, specific phobias, social anxiety disorder, and panic disorder, among others 9. Anxiety frequently coexists with depression and may emerge during the prodromal stage of PD, becoming more prevalent during "off" periods 13,23.
Early evaluation in primary care is essential due to the negative impact of anxiety on quality of life. Assessment tools like the Parkinson Anxiety Scale, which specifically evaluates persistent and episodic anxiety through 12 items, are helpful for clinical screening 24. Although current evidence is limited, higher doses of antidepressants, particularly SSRIs, have been associated with adequate responses in treating anxiety in PD 25,26. Non-pharmacological strategies such as CBT have been shown to have an impact on this symptom 27.
1.3 Psychosis
Psychotic disorders in both the general population and PD include symptoms such as hallucinations, delusions, and alterations in language (e.g., impaired discourse organization, reduced verbal fluency, and difficulties with pragmatic language use) and thought 9,28. Hallucinations may present as fleeting phenomena and illusions (45%), visual hallucinations (15%), or non-visual hallucinations (35%) 29. Their prevalence increases in advanced PD stages 30, typically beginning with fleeting perceptions or feelings of presence that progress to hallucinations as the disease evolves 30. The Parkinson Psychosis Questionnaire is used to assess the frequency and severity of these symptoms 24.
Treatment involves reducing dopaminergic therapy, particularly dopaminergic agonists, identifying potential triggers such as infections, and avoiding pro-hallucinatory medications, including anticholinergics 24. When pharmacological intervention is required, pimavanserin has demonstrated efficacy in reducing psychotic symptoms in PD. 31. Alternative options include quetiapine and clozapine 32,33, and rivastigmine may be beneficial in cases associated with dementia 34. Electroconvulsive therapy can be useful in severe cases 35. Other strategies such as CBT, psychoeducation, and environmental modifications (e.g., minimizing sensory overload and improving lighting, among others) can also be beneficial 36,37.
1.4 Impulse control disorders (ICDs)
Defined in the DSM-5 as the inability to resist impulses that may harm the patient or others, these disorders encompass behaviors such as pathological gambling, compulsive shopping, and binge eating 9. Other characteristic behaviors include punding (engagement in purposeless repetitive motor activities) and hobbyism (excessive preoccupation with hobbies or activities) 24. The prevalence of ICDs in PD is approximately 14%, with a 5-year cumulative incidence of up to 46% 38,39.
The primary risk factor is the use of dopaminergic agonists, followed to a lesser extent by levodopa and amantadine 40. The Questionnaire for Impulsive-Compulsive Disorders Rating Scale, along with the MDS Non-Motor Symptoms -Questionnaire (MDS-NMS-Q), aids in evaluating these symptoms in PD 24,41. Primary interventions involves reducing dopaminergic agonists and monitoring withdrawal symptoms 42.
1.5 Apathy
Apathy in PD manifests as a loss of motivation without cognitive impairment, characterized by reduced goal-directed behavior and thought. Its prevalence ranges between 15 and 70% in PD patients 24. Assessment tools include the Apathy Evaluation Scale (AES), Apathy Scale, and Apathy Inventory, with the AES-12PD being specific for PD 43. Treatment options are limited; evidence suggests that cholinesterase inhibitors and levodopa during "on" periods may be beneficial 44,45.
2. Sleep disorders
Up to 71% of PD patients are affected by sleep disturbances, significantly impacting their quality of life 46. These symptoms occur at all stages of the disease and are associated with other psychiatric and cognitive manifestations 47.
2.1 Rapid Eye Movement (REM) Sleep Behavior Disorder
REM behavior disorder (RBD) is characterized by the loss of REM sleep atonia, allowing patients to physically act out their dreams 48. It is a key prodromal symptom, appearing 10-15 years before a PD diagnosis 49,50. Studies show that over 90% of patients with isolated RBD progress to PD or other α-synucleinopathies, with PD being the most common 51,52. RBD is confirmed via polysomnography and treated with melatonin (up to 12 mg) or clonazepam (0.25-4 mg) to regulate the sleep cycle, alongside environmental modifications to prevent injuries 48,53. Early detection is crucial for patient safety and quality of life.
2.2 Insomnia and sleep fragmentation
Insomnia in PD involves difficulty initiating or maintaining sleep, affecting 30-80% of patients 54. Initiation insomnia is linked to psychiatric disorders, while maintenance insomnia-affecting 70% of PD patients-is the most common, exacerbated by nocturnal "off" periods due to symptoms like pain, sweating, and nocturia 50. Other triggers include obstructive sleep apnea syndrome, restless legs syndrome, and periodic limb movement disorder, which cause sleep fragmentation and excessive daytime sleepiness (EDS) 50. The Insomnia Severity Index aids in diagnosing and monitoring insomnia. Initial treatment includes melatonin (3-5 mg), adjustments in dopaminergic medications, and sleep hygiene measures 47,53.
2.3 Excessive daytime sleepiness
EDS, affecting approximately 35% of PD patients, is characterized by the need for daytime naps, often linked to dopaminergic dysfunction and insomnia 55,56. The Epworth Sleepiness Scale, with scores above 10, is commonly used to identify EDS 47. Management strategies involve stimulants like coffee and evening exercise, which promote wakefulness and provide antioxidant benefits 57. Modafinil or methylphenidate is reserved for specific cases, with risk assessments 48. Non-pharmacological treatments such as bright light therapy and sleep hygiene measures can help regulate circadian rhythms, improving sleep schedules 58. Identifying coexisting insomnia and EDS can substantially improve patients' quality of life.
3. Sensory-perceptual symptoms
The majority of PD patients experience sensory-perceptual disturbances, which are often under-diagnosed and receive limited clinical attention, despite potentially preceding motor symptoms by up to five years. This highlights their value for early detection 59.
3.1 Olfactory and visual impairments
Olfaction and vision are the most commonly affected senses in PD, with alterations reported in up to 80% of patients 60,61. Hyposmia, which may precede motor symptoms by several years, indicates disease progression and suggests invasion of Lewy bodies into olfactory circuits 60,62. Studies indicate that this symptom results from the loss of cholinergic and dopaminergic neurons in the olfactory bulb 60. Assessment tools include the University of Pennsylvania Smell Identification Test 63,64.
Visual changes include difficulties with contrast sensitivity, color discrimination, diplopia, and blurry vision, affecting up to 82% of patients 65. Dopaminergic cell loss in the retina, associated with a reduction in synaptic contacts with melanopsin-containing retinal ganglion cells, has been linked to visual dysfunction and impaired contrast sensitivity in PD 66.
3.2 Pain
Pain affects up to 85% of PD patients, with both nociceptive and neuropathic pain fluctuating during "on" and "off" periods, being associated with an increase of pain when dopamine levels drop, as there is increased rigidity, bradykinesia, and abnormal postures, which may contribute to mechanical strain and inflammation 67. The pathophysiology of pain in PD involves complex, multifactorial disruptions in dopaminergic, glutamatergic, serotonergic, nor-adrenergic, and cholinergic systems that alter pain modulation, perception, and transmission throughout disease progression 67.
Neuropathic pain, which may result from small fiber neuropathy, manifests as burning or prickling sensations, particularly during "off" periods and on the more affected side 68,69. Management includes tricyclic antidepressants and neuromodulators such as pregabalin and gabapentin 67. Options like lidocaine (off-label) and safinamide might be effective in cases of inadequate response and persistence of radicular pain 70,71. Safinamide has demonstrated a reduction in pain levels when used as an adjunct to levodopa, especially during "off" periods 72. Regarding other strategies, physical exercise, yoga, or tai chi might help to improve pain 73. Evaluation involves a detailed anamnesis and the use of the MDS-NMS-Q to assess pain severity and its psychological impact 41. More advanced diagnostic methods, such as microneurography and evoked potentials, may also be employed but are not routinely used due to high costs 67,68.
4. Autonomic Symptoms
4.1 Orthostatic hypotension (OH)
Orthostatic hypotension in PD refers to a drop in blood pressure upon standing, associated with α-synuclein deposits and loss of efferent sympathetic neurons 74. It affects up to 30% of patients, increasing the risk of falls 75. Distinguishing neurogenic from non-neurogenic OH is essential, as the former reflects the underlying pathophysiology of PD, while the latter often stems from reversible factors such as dehydration or physical deconditioning 76. Dopaminergic treatment may exacerbate OH 77.
This symptom in PD is clinically diagnosed by a sustained drop of ≥20 mmHg systolic or ≥10 mmHg diastolic within 3 minutes of standing, after ruling out other causes. The MDS-NMS-Q and the Orthostatic Grading Scale are useful tools for diagnosis 41,78. Non-pharmacological strategies include lifestyle modifications, such as postural adjustments, adequate hydration, and avoiding large meals 76. Pharmacological treatment, when needed, involves sympathomimetic agents such as droxidopa, midodrine, and fludrocortisone 79.
4.2 Gastrointestinal dysfunction
Gastrointestinal (GI) symptoms in PD, such as dysphagia, early satiety, and constipation, often emerge early and are linked to α-synuclein accumulation in the GI tract 80. The frequency of these symptoms in PD patients varies: dysphagia may develop in more than 80% of patients as the disease progresses 81; sialorrhea affects up to 80% 82; and symptoms of gastroparesis (such as nausea, vomiting, and abdominal bloating) occur in up to 45% of patients 83, impacting nutrition and quality of life. Small intestinal bacterial overgrowth, observed in around 50% of patients, exacerbates GI symptoms and may worsen motor dysfunction 84.
Management includes probiotics to regulate intestinal microbiota, dietary adjustments emphasizing high fiber intake, coffee intake, and adequate hydration 85-87. Additional treatments involve prokinetic agents like domperidone, though dopamine D2 receptor antagonists that cross the blood-brain barrier, such as metoclopramide, are contraindicated in PD 88. Domperidone should be administered with caution, as it has been associated with cardiac electrophysiological abnormalities and an increased risk of mortality 89. In severe cases, laxatives may be employed, with careful monitoring of levodopa absorption and efficacy 90. Other treatment strategies, such as gastric electrical stimulation or botulinum toxin injections into the pyloric or anal sphincters and submandibular glands, have been studied but currently have limited evidence 83,86.
4.3 Urinary dysfunction
Approximately 27-85% of PD patients experience urinary dysfunction early on, with detrusor hyperactivity linked to central dopaminergic degeneration, autonomic dysfunction, and impaired inhibitory control by the basal ganglia 91-93. Symptoms include increased frequency and incontinence, which are associated with increased fall risk and potentially worse motor and cognitive prognosis 94. The International Consultation for Incontinence Questionnaire and the Over Activity of the Bladder Questionnaire facilitate clinical evaluation 95. Management includes anti-muscarinic agents, α-3 adrenergic agonists, intravesical botulinum toxin, and lifestyle adjustments such as scheduled voiding and controlled fluid intake 93,96. Deep brain stimulation of the subthalamic nucleus may also improve detrusor hyperactivity and nocturia 97.
4.4 Sexual dysfunction
Sexual dysfunction affects over 50% of early-stage PD patients and includes reduced libido, erectile and ejaculatory disorders, and vaginal dryness, primarily due to dopaminergic depletion 92. Tools like the International Index of Erectile Function and Female Sexual Function Index assess these symptoms 98. Management is individualized and may involve CBT and sex therapy and pharmacological treatment such as sildenafil and apomorphine (for erectile disorder in men) 98.
5. Cognitive symptoms
Cognitive impairment in PD spans from early to advanced stages. Between 24.5% and 31.1% of patients develop dementia, rising to 46% after 10 years and up to 83% after 20 years post-diagnosis (99,100. Approximately 20% of patients exhibit mild cognitive impairment (MCI) at diagnosis 99. Risk factors include hallucinations, advanced age, low educational attainment, and depression, with up to 40% of cases potentially preventable through early lifestyle interventions 101,102. Mitochondrial dysfunction, amyloid deposition, and cerebrovascular alterations contribute to cognitive decline, alongside dysfunction in frontotemporal neural networks 99. Affected domains include visuospatial, attentional, memory, and executive functions 103.
Cognitive phenotypes in PD include subjective cognitive decline (SCD), MCI, and dementia. SCD refers to self-perceived decline without objective impairment on standardized tests 104. MCI involves deficits in one or more cognitive domains, with preserved functional independence 103. Dementia is characterized by impairment in at least two domains, severe enough to interfere with daily life beyond the impact of motor symptoms 99,105.
The Montreal Cognitive Assessment (MoCA) is the most commonly used screening tool for cognitive impairment in PD, offering good sensitivity for early deficits and guiding the need for further neuropsychological evaluation 99,106. Treatments include rivastigmine for PD dementia, while non-pharmacological strategies are employed for MCI, though long-term outcomes remain uncertain 107. Psychoeducation, cognitive-behavioral interventions, and mindfulness-based approaches show promising results, but their efficacy remains under investigation 108,109. Physical exercise, especially resistance and aerobic training, improves memory, attention, and processing speed, positively impacting quality of life 110.
Conclusions
PD presents a multidimensional clinical challenge, with non-motor symptoms contributing substantially to functional decline, reduced quality of life, and increased healthcare complexity. These symptoms, spanning neuropsychiatric, cognitive, autonomic, and sensory domains, require continuous and personalized management beyond initial diagnosis. Tools like the MDS-NMS-Q 41) provide structured frameworks for symptom evaluation, while domain-specific instruments support more precise clinical assessment and therapeutic decision-making. Moreover, motor fluctuations deserve particular attention, as "off" and "on" periods in PD can contribute to the exacerbation of non-motor symptoms.
Despite growing awareness of the relevance of non-motor symptoms, significant gaps persist in their systematic assessment and integration into routine care. Advancing multidisciplinary, patient-centered strategies requires not only early detection but also ongoing reassessment and therapeutic plans tailored to evolving patient needs. Future research should focus on identifying and validating biomarkers capable of detecting and monitoring non-motor symptoms at early stages, facilitating prompt and targeted interventions.
In parallel, the development of disease-modifying therapies suitable for early use, along with more effective and individualized symptomatic treatments, remains a key objective for improving long-term outcomes. Enhancing the understanding and management of non-motor symptoms is essential to advance the quality of care in PD, not only by improving clinical outcomes but also by alleviating the broader personal and societal burden associated with the disease 7.

