










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.25 no.3 Bogotá July/Sept. 2010
The role of ileocolonoscopy in Inflammatory Bowel Disease (IBD)
Rodrigo Castaño Llano, MD (1)
(1) Gastrointestinal Surgery and Endoscopy-Hospital Pablo Tobón Uribe. Gastro Hepatology group-Universidad de Antioquia. Professor Universidad Pontificia Bolivariana. Medellín, Colombia..
Received: 14-01-10 Accepted: 10-08-10
Abstract
Ileocolonoscopy plays a critical role in the diagnosis and treatment of inflammatory bowel disease (IBD) This article reviews the utility of ileocolonoscopy in the diagnosis of the ulcerative colitis and Crohns Disease (CD). It emphasizes recommendations for monitoring cancer and the use of the most recent techniques to increase detection of dysplasia. It discusses the latest diagnostic techniques such as colonoscopy with narrow band imaging (NBI), the role of colonoscopy in management of IBD complications, and the current role of endoscopic capsules and balloon assisted enteroscopy in patients with Crohns disease.
Keywords
Colonoscopy, Inflammatory bowel disease, Crohns disease, Ulcerative colitis, Capsule Endoscopy.
Introduction
Ileocolonoscopy, supported by the magnification available with narrow band imaging (NBI), is the principal method used for diagnosing inflammatory bowel disease (IBD). It is also the fundamental support for managing these patients. Recent improvements in endoscopic techniques such as capsule endoscopy and enteroscopy permit a detailed evaluation of areas of the small intestine which were previously unexplored.
Based on current literature, ileocolonoscopy is considered pertinent to the case of IBD whenever it is performed with the following purposes:
1. For the initial diagnosis and in order to differentiate UC from CD (1, 2).
2. To evaluate the extension of the activity of the entity (1, 2).
3. To investigate lack of response to treatment (1).
4. To evaluate patients with severe or acute ailments (3).
5. To investigate symptoms suggesting complications or neoplasia (1).
6. To screen for colorectal cancer after 10 years of illness in patients suffering pancolitis, or after 15 years in patients with left-sided colitis (4).
7. To evaluate the ileal pouch and ileorectal anastomosis (5).
8. To provide endoscopic therapy for stenosis, bleeding, or polyps (6, 7).
Ileocolonoscopy is not considered to be appropriate for:
1. Patients in stable condition
2. Evaluations of patients with a mild to moderate recurrences (8).
The importance of the rational use of ileocolonoscopy in this context lies in the fact that it is an invasive and expensive procedure. The inappropriate use due to excess or lack of this resource could redound in unnecessary expenses or negative outcomes for the patient, with potential legal implications for the treating physician.
Initial endoscopic evaluation of IBD
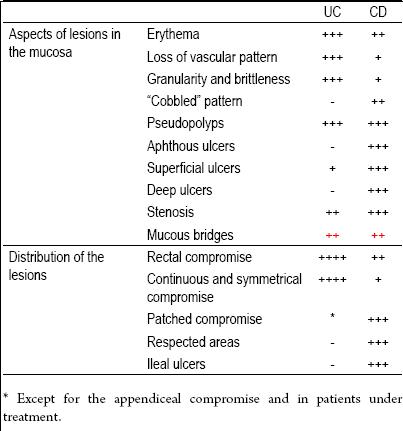
When IBD is suspected, endoscopic evaluation is obligatory in order to confirm or discard the diagnosis and establish the appropriate medical procedure. Since a number of conditions can simulate IBD, the unnecessary use of medicines, possibly toxic, must be avoided. Additionally, endoscopic evaluations are important in order to distinguish ulcerative colitis (UC) from Crohns disease (CD), as well as to determine the extension of the illness. Medical treatment may on some occasions hinder the distinction between UC and colonic CD because it can induce segmented healing with no rectal compromise in patients that suffer UC. Thus, it is important that initial evaluation endoscopies are carried out prior to initiation of any medical treatment. Similarly, systemic treatments can veil compromises of the small intestine in patients with CD. While the difference between UC and CD may not be evident in the initial stages of procedure, a case-history of the inflammation of the small intestine can become a particularly important factor if surgery becomes necessary during the course of the illness (Table 1).
Table 1. Differences in the colonoscopy between CD and UC.
In the absence of extracolonic disease, certain endoscopic findings could suggest a diagnosis of colitis due to CD rather than UC. The most telling of these findings is the presence of microscopically normal areas patched with macroscopic mucosa. Apparently, the endoscopic aspect of the inflamed mucosa can be useful in order to differentiate the two ailments. The definition of "ulcerative" colitis is, as a matter of fact, mistaken; the great majority of patients with UC develop granular and brittle mucosa, the more severe forms with deeper errosions (Figures 1a and 1b).The characteristic feature of demarcation of inflamed and normal colonic mucosa is often evident in CD (Figure 1c). Endoscopic findings of deep, stellar, linear, or serpiginous ulcers hint at a colonic CD diagnosis (Figure 1d). Pseudopolyps and the adenomatous polyps most often suggest a UC diagnosis (figure 1e, 1f). Stenoses are extremely rare in UC and are a reason to suspect the possibility of CD or malignancy (Figure 1g). Similarly, recognition of an open internal fistula during endoscopy will often establish a diagnosis of CD (Figures 1h and 1ij). Also the fibrotic lesions of UC (Figure 1J) or CD may become evident, or endoscopy or a simple examination may permit detection of perianal fistulas which point more to a CD diagnosis (Figure 1k).
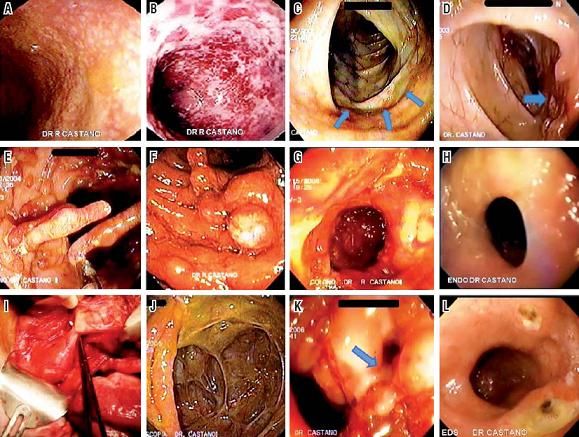
Figure 1. Endoscopic characteristics of Ulcerative Colitis and Crohn’s disease. A. Endoscopic characteristics of mild UC. B. Endoscopic characteristics of severe UC. C. Limit between healthy colonic mucosa and inflamed mucosa in CD. D. Linear ulcer in CD. E. Pseudopolyps in UC. F. Adenomatous polyps in UC. G. Rectal stenosis in CD. H. Duodenocolic fistula associated with CD. I. Surgery of Duodenocolic fistula. J. Consequences of UC with cecal fibrosis. K. Anal duct fistula in CD. L. CD of the esophagus.
The significant proportion of patients with CD which might present symptoms and a colonoscopy indistinguishable from a UC has been minimized. In clinical practice, patients with constant rectal inflammation, tested by means of sigmoidoscopy, is often incorrectly classified as UC without performing any further exams such as an ileoscopy. As the ability to evaluate the mucosa of the small intestine has increased, the number of patients with UC (which is similar to CD), for whom it has been demonstrated that they suffered from inflammation of the small intestine, has significantly improved (9). There have been patients with CD that present symptoms of proctitis, with constant rectal inflammation without patched areas, deep ulcers, or granulomas in the biopsy. In these cases the findings from an ileal intubation can offer an important contribution to the final diagnosis. As patients may also have a compromise in the superior digestive tract, an upper endoscopy is recommended in order to establish a diagnosis of CD in the superior digestive tract, especially in pediatric patients and the young (Figure 1L).
Although the histopathological characteristics of biopsy specimens obtained during endoscopy may be similar for cases of UC and CD, certain findings may be very useful for differentiating between the two entities. Non-caseous granulomas pathognomonic of CD are found in close to 30% of the biopsies and in close to 50% of specimens obtained surgically (10). In order to provide convincing evidence of CD, the granulomas have to be separated from the crypts, as occasional mucinous granulomas may be seen in other illnesses. Likewise, it is important that biopsies of the colon are taken from the compromised areas as well as from the uncompromised areas in order to determine the microscopic extension of the ailment (11).
Certain mistakes in the interpretation of the endoscopic findings in patients with IBD are common. In patients with treated UC, the inflammation often seems segmented, with no relative rectal compromise. This has been described in de novo UC, mainly in the pediatric population (12). Likewise, a subgroup of patients with uncomplicated UC was found to have small areas of mucosa with chronic inflammation around the appendiceal orifice (cecal patch). Although technically these are patchy lesions, these cecal patches are not predictive since they are a typical finding in both ailments (13). Finally, the concept of "reflux" ileitis has been confusing for the endoscopists. A minority of patients with pancolitis occasionally present short, not larger than a few centimeters in length, mildly inflamed segments in the terminal ileum, usually without ulceration. More severe inflammation, more extensive compromise, or ileal inflammation in the absence of pancolitis may indicate a diagnosis of CD (14). The presence of "focal gastritis" is another source of confusion. While it was initially described as in cases of CD, it has also been seen in patients with UC. Thus its presence does not help differentiate between the two diagnoses. Diffuse duodenitis, particularly in younger patients has also been reported in association with UC. An official diagnosis of UC or CD is debatable in these cases as they often have a benign development after a colectomy with reconstruction of the ileal pouch (15).
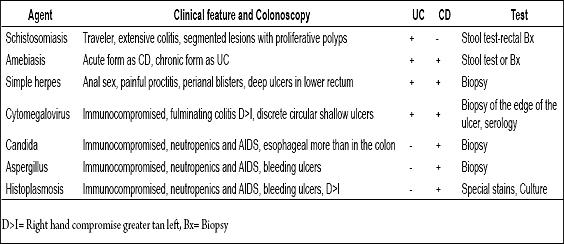
Tables 2 and 3 show differential diagnoses in cases of IBD.
Table 2. Differential diagnoses of IBD and bacterial ailments.

Table 3. Differential diagnosis of IBD and parasitic, viral and fungal ailments.
Evaluation of patients with IBD during the development of their illnesses
Patients with well established diagnosis of CD or UC often develop a secondary diagnosis which can potentially imitate IBD. Irritable bowel syndrome (IBS), bacterial overgrowth, colitis produced by cytomegalovirus (CMV), C difficile or other enteric infections, ischemic colitis and colorectal cancer all have the potential to cause diagnostic confusion (10). Colonoscopies of patients with IBD are carried out to evaluate the activity of the illness and exclude any other secondary diagnoses. Unfortunately, the C reactive protein (CRP) and the speed of glomerular sedimentation (SGS) are unresponsive and non-specific markers with regard to IBD activity (16). Endoscopic evaluations are invaluable for patients with different symptoms or for those that do not respond as expected to therapy. In those patients in whom immunosuppressant therapy fails, particularly corticosteroids, one must think of a secondary CMV infection. While noninvasive tests such as the polymerase chain reaction (PCR) and antigen tests exist, their responsiveness and specificity for evaluating colonic compromise is not clear (17). The best test for a evaluating an invasive of the tissue by CMV in colitis is the documentation of included bodies and the cytopathic effects of CMV in colon biopsies. Thus, prior to escalating into treatment or surgery, a colonoscopic biopsy must be considered for all patients for whom immunosuppressant therapy has failed. A CMV infection can be discarded if this procedure verifies the presence of mucosal inflammation. Occasionally, elderly patients with IBD may present abdominal pain and rectal bleeding and, if we do not diagnose a worsening of their IBD, we could come up with a diagnosis of ischemic colitis (Figure 2A). It is imperative these patients be evaluated endoscopically, before beginning any immunosuppressive treatment such as corticosteroids, which are dangerous in such a scenario. Amebic colitis also has to be ruled out (Figure 2B). Among patients who are refractory to treatment the physician should consider the diagnosis of colitis caused by CMV (Figure 2C).
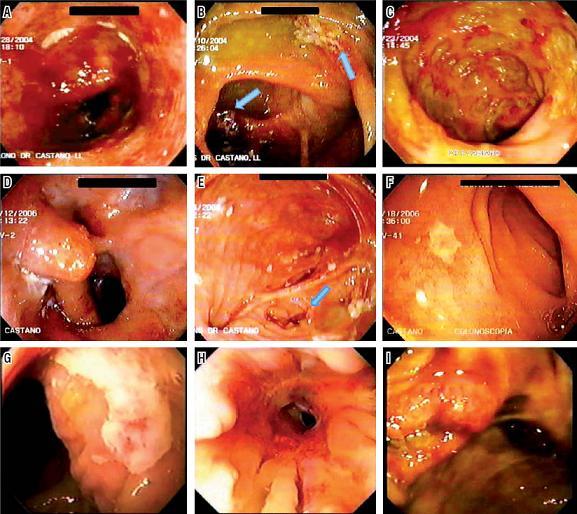
Figure 2. Differential diagnoses of Ulcerative Colitis and Crohn’s Disease. A. Differential diagnosis of ischemic colitis resembles UC. B. Differential diagnosis of amoebic typhlitis. C. Proctocolitis due to CMV in patients with history of HIV. D. Stenosis and inflammation due to ileorectal anastomosis. E. Deep ulcers in the ileal pouch due to unrecognized CD. F. Superficial ulcers of the afferent loop due to unrecognized CD. G. Superficial ulcers of the afferent loop due to unrecognized CD. H. Cuffitis and local stenosis. I. Actively bleeding cecal ulcer meriting sclerotherapy.
One of the least used applications of endoscopy is the evaluation of ileorectal anastomosis after resection (Figure 2D). Recurrence of illnesses occurs frequently in the natural history of patients who require surgery. An almost inexorable progression can occur leasing to an important stenosis prior to the development of symptoms. The endoscopic appearance of ileocolonic stenosis six months after surgery can be used to identify patients at high risk for recurrence of stenosis. This helps identify those who could benefit from early intervention (Table 4).
Table 4. Rutgeerts Score classification of CD recurrence after surgical resection (18).
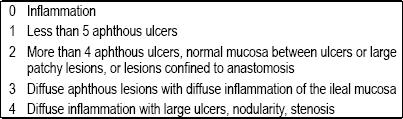
A Rutgeerts score of 0 or 1 indicates low risk of recurrence of the illnesss symptoms in the future. A higher Rutgeerts score is associated with a risk of complications. In Rutgeerts original studies (18) almost all of the patients given 3 or 4 points during a six month check-up had recurrences of their symptoms the following year. In addition, one third of the patients who received 4 points required a second resection within three years of the original surgery. Although sufficiently powerful studies have not yet been conducted, early evaluation and appropriate treatment can prevent the recurrence of symptoms and the necessity of surgical intervention.
A well documented subgroup of patients with CU who had had surgery treatment of their ileal pouch often develop recurrence of symptoms suggestive of pouchitis (19)An endoscopic evaluation of the ileal pouch is mandatory to confirm this diagnosis and initiate appropriate treatment.
During follow up a small subgroup of patients develop refractory pouchitis which is diagnosed as CD because of the presence of the type of ulcers which are typical in this disease (Figure 2E) and in the afferent ileal loop (Figures F and G). In medical centers which do not perform mucosectomies of the rectal reservoir, a diagnosis of cuffitis (inflammation of the remnant rectal cuff) should be considered (Figure 2H). Treatment with 5-ASA suppositories is effective (20). Many years after colectomies with terminal ileostomies have been performed to treat UC, some patients may begin to suffer from inflammation of the small intestine with characteristics of CD. Colonoscopies for severe UC can also be used to indicate the prognosis when there are severe lesions such as when the endoscopy encounters denuded mucosa indicating the imminent need for surgery.
Occasionally patients with CD present extremely aggregated bleeding due to the depth of the ulcers which can expose the bleeding blood vessels. These patients can initially be managed with endoscopic treatment and sclerotherapy, although some require surgical treatment (Figure 21). An interesting aspect of endoscopic evaluation of IBD is the effect that treatment has on endoscopic healing. It is well known that corticosteroids generally do not induce healing of the mucosa despite clinical improvements which they produce in the majority of patients (21). This is one of the reasons that steroids may not be effective as a maintenance treatment. On the other hand all of the thiopurines such as infliximab can induce healing of the mucosa and are of great value as maintenance agents for treating IBD (22). The healing effect of the mucosa on the natural history of an illness is currently being investigated (23). As of this date the use of endoscopic evaluations of asymptomatic patients should not be routine practice for following up on clinically effective treatment of IBD.
In the context of noninvasive evaluations and monitoring of the illness, two tests have been developed to measure inflammatory activity: the lactoferrin stool test and the fecal calprotectin assay. Both are very sensitive but not very specific (24).
Vigilance against cancer in IBD patients
As a consequence of chronic inflammation, patients with UC and colitis associated with CD have a high risk of colorectal carcinoma (CRC). A metaanalysis estimated that the accumulated incidence of adenocarcinoma in patients with UC after onset is 2% at 10 years, 8% at 20 years, and 18% at 30 years (25). Although there are no publications with random assignment of endoscopic monitoring, retrospective studies have demonstrated that patients whose cancer is detected in early stages have good chances of survival. In the face of scanty comparative information from screening tests, the experts have developed various guides which are available to physicians (26-29). Although their recommendations are similar to each other, there are some significant differences.
Duration and extension are the two factors with greatest impact on individual risk of developing CRC. Moreover, they are the principal determinants of when screening should begin. Estimating the duration of the illness is simple for UC since its onset is accompanied by bloody diarrhea. On the other hand, the onset of Crohns disease can be silent, so it is often diagnosed late. Care should be taken at the moment of diagnosis to measure the duration of the illness from the onset of symptoms rather than from the moment of diagnosis. The four articles recommend that the first follow-up colonoscopy be performed 8 to 10 years after onset of the disease. One group of authors suggests that follow-up examinations of patients with left colitis should be deferred until 15 years after onset. (29) Others recommend follow-up colonoscopy every one or two years when colitis affects both sides and pancolitis is present. Patients with proctitis and proctosigmoiditis have not been shown to have high risks of developing CRC, so only routine screening is recommended (26, 27).
Other important factors that increase the risk of CRC are coexisting primary sclerosing cholangitis (30), a family history of CRC (31), and possibly the degree of inflammation seen in the biopsy (32). However, disagreements exist over how these factors should influence vigilance in practice. Two of the four guides mentioned recommend beginning observation of patients with PSC as soon as they are diagnosed with UC (26, 27) with a group of authors recommending annual colonoscopies to monitor this population. The other two guides have not formally incorporated these factors.
The frequency with which dysplasia develops in patients with chronic colitis makes monitoring these patients with colonoscopies even more important of a goal than it is among other patients. A complete endoscopic examination with a prolonged evaluation and cleaning of the occult mucosa is essential. Biopsies must be taken from all types of polyps, masses, stenoses and irregular mucosas. Although this approximation will identify a large number of dysplastic lesions, a significant number will remain unseen (33). Consequently, biopsies should be taken from every 10 cm of affected mucosa in the four quadrants. It has been estimated that a minimum of 33 biopsies are required to have a 90% chance of detecting a dysplasia (34). Despite this approximation, the malignance can still develop within a relative short time after a follow-up colonoscopy (35). It is not clear whether this is a reflection of the rapid progression of the incidental neoplasia or is simply the reflection of the inefficiency of the colonoscopic study. Independent of the answer to this question, it subsequent follow-up colonoscopies are recommended at intervals of one or two years.
The presence of low grade dysplasia (LGD) is a worrisome finding because it is commonly multifocal (36). Because of the relatively low sensitivity and specificity of colonoscopy for finding LGD, the discovery of this entity in one area could indicate a more advanced neoplasia at that site, or at another location in the colon. When information from many studios was compiled, it was found that the prevalence of cancer in patients upon whom colectomies had been performed because of LGDs without lesions was 22%, with an additional 11% with high grade dysplasias (37). In a comparison of patients with LGD who did not undergo colectomies and patients who had not been diagnosed with dysplasias, the odds ratio was 9.0 for the development of cancer. Despite implementing surveillance almost half of the tumors encountered were in advanced stages at the moment of diagnosis (38). Based on this information, colectomies should be offered to all patients with LGDs, particularly to those with multifocal dysplasia. Dysplastic polyps originating in the context of chronic colitis are related to lesions or masses associated with dysplasia (LMAD). In the same systematic review, 41% of the patients among whom LMAD with LGD was found demonstrated that they had CRC at the follow-up after the colectomy (38). In the subgroup of patients who did not undergo surgery, 64% developed scaled high grade dysplasia and cancer. LMADs typically have been considered to be B indications for colectomies. Many authors, using ample data, have tried to determine which dysplastic polyps can be safely removed endoscopically from patients with colitis. In one initial article biopsies were taken from the mucosa around the site of a polypectomy and the patients were monitored prospectively. Adenocarcinomas developed in 3 patients around whose polyps dysplasias had been detected whereas none of the 5 patients with negative findings developed cancer (38). An earlier article reported a series of 48 patients, who had undergone colonoscopic polypectomies. These patients had a total of 60 sessile and pedunculated lesions, and patients showed no dysplasias in the mucosa around the lesions. After being monitored for an average of 4.1 years, no cancers were detected (39, 40). A similar report studied 24 patients with dysplastic polyps which appeared to be adenomas. After monitoring for an average of 3.5 years no cancers were found (40). These two studies suggest that dysplastic lesions originating in areas affected by colitis should be treated endoscopically rather than surgically.
A number of recent techniques have been used in the attempt to increase the sensitivity of colonoscopy in monitoring for dysplasia. One of these, methylene blue chromoendoscopy (MBC) has shown itself to be promising. Methylene blue colors the normal colonic mucosa with less stain than for dysplastic epethilium. In addition, it creates lakes of color in areas with irregular surfaces. Both effects allow potentially improved identification of occult colonic neoplasias. In a randomized study of 165 patients with quiescent UC quiescent routine surveillance colonoscopies or MBCs were performed with magnification (41). 0.1% methylene blue was spread in segments, and then after one minute the excess was removed by suction. The pit pattern was used to direct biopsies in areas that appeared to be normal. In addition, biopsies were taken at random every 10 cm from both groups of patients. 32 intraepithelial neoplasias were discovered among the 84 patients who were examined with MBC while only 10 lesions were found in the 81 patients who were conventionally screened (p=0.003). It is worth noting that 2 areas of dysplasias were found by random biopsies in patients in the group examined with MBC, suggesting that examinations should not rely only on directed biopsies (41).
The same author has recently published another similar study. This time it compares standard surveillance with MBC using confocal microscopy (42). Biopsies were taken as described above from the group upon which standard surveillance techniques were used. Directed biopsies were taken from the MBC group. Again intraepithelial neoplasias were discovered among the 80 patients examined using MBC. 12 areas of dysplasias were encountered among them, compared to only 2 which were discovered from among the 73 patients screened with conventional techniques (42). Because of the study design it is not possible to determine if it would have been possible to identify additional cases of dysplasia if random biopsies had also been taken in the group examined with MBC. In both studies the use of methylene blue chromoendoscopy added 11 minutes to the total time required for colonoscopies (41, 42). Promising, but preliminary, information exists about the use of chromoendoscopy with indigo carmine (43) and fluorescent colonoscopy (44). The only study done of images taken with narrow band imaging (NBI) failed to demonstrate any increase in detection of dysplasia (45).
Unfortunately information that would allow a comparison among the different diagnostic modalities does not exist. It is worth noting that many of these studies compare standard endoscopy with high definition chromoendoscopy. We remain without clarity about whether high definition chromoendoscopy without staining can achieve the same results as does MBC. In addition, the fact that these were not blind studies combined with the increased procedure times raises the possibility that these factors, rather than those under study, could be responsible for the increased rates of detection. Very few studies have been published with respect to the learning curves associated with these techniques. Moreover it is not clear if it would be practical to try to implement the use of these techniques generally. We should consider what the sensitivity and specificity of these techniques might be in the hands of practitioners who are not experts (46). At the minimum physicians who are neophytes in the use of these techniques should be counseled that they should continue to take random biopsies during surveillance for cancer until they are certain that their rate of errors is very low. Finally, in the context of active inflammation reactive changes can imitate dysplasia. For this reason surveillance colonoscopies are conducted in periods of remission (47). Despite this there are several points at which certainty does not exist in the interpretation of a biopsy. These results are described as being indefinite for dysplasia. In this context it is important that biopsies be reviewed by pathologists who are experts in the gastrointestinal tract. Endoscopies should be repeated at short intervals of time (for example every 3 to 6 months) obtaining multiple biopsies of the area in question. Ideally this period will be after the complete suppression of inflammation.
RECENT ENDOSCOPIC TECHNIQUES
Endoscopic Balloon Dilation (EBD)
Different articles describe endoscopic balloon dilation (EBD) as an alternative to surgery for treatment of stenosis resulting from Crohns disease (48, 49). Proposed counterindications for this technique include internal fistulas, long stenoses, and ulcers at the site of the stenosis (50). In these articles the typical diameter of the objective is between 15mm and 20 mm. Some authors try to accomplish dilation in multiple sessions, while others complete the dilation the first day. Empirical injections of corticosteroids are advised in these articles, however the only supporting information demonstrated is retrospective (51). Reports of results from this technique vary among studies, with recurrence of symptoms common after only one procedure. Many patients can apparently avoid or delay surgery with this technique, however multiple sessions may be required and perforations appear to be relatively common. Rates of complications vary between 0% and 11% in the majority of series reported (50).
In light of these rates of complications a conservative approach is indicated. Dilation should be considered only for short stenoses (maximum three cm). We should also carry out rigorous radiological examinations to be certain that the target of dilation is in fact the source of the patients symptoms. If the endoscopic examination shows an ulcer, and the symptoms permit, it should be treated initially with systemic corticosteroids. If the patient improves, treatment with infliximab or adalimumab should be considered, bearing in mind that these medications can, in some particular cases, narrow the stenosis. Only when these interventions have failed should endoscopic intervention be considered.
Capsule endoscopy
Capsule endoscopy (CE) facilitates complete evaluation of the small intestine. It is more sensitive than conventional radiology and much less invasive than previously available option (intraoperative endoscopy). Despite this uncertainty exists about its role when IBD has already been confirmed. While the exact role of CE is still under study, this technique has proven itself useful in certain contexts. Similar to conventional endoscopy, the principal indication for a diagnosis of IBD when using CE is the evaluation of activity. A recent metaanalysis concluded that CE was substantially more sensitive to CD than traditional diagnostic modalities like barium radiology, ileoscopy, CT scans, and enteroscopy (52). The similarities of findings for IBD with those of other entities make biopsies necessary for the evaluation of these patients, and for this task endoscopies are preferable. Nevertheless, when a definitive diagnosis of IBD is no possible, CE is very useful (53).
An evaluation of the small intestine becomes particularly important when a colectomy of the ileal pouch is under consideration, as a history of CD in the small intestine can predict a complicated course of development after surgery (54). CE should be considered for all patients that are having ileal pouch evaluations and who have had prior ileoscopic evaluation (55). In addition, it could be useful to define the extent of the disease with a detailed evaluation of the small intestine of patients with endoscopic findings suggestive of CD such as linear ulcers, deep patchy lesions or paving stone pattern of lesions (56). Finally, patients with clinical characteristics suggesting CD, such as initial presentation without bloody diarrhea or significant weight loss, should be considered for CE. Findings of CD in the small intestine vary broadly from extremely nonspecific patchy erythema and aphthous ulcerations to broad superficial ulcers. Classically the indications seen most often include nodulation (Figure 3A), erosion (Figure 3 B), superficial ulcers (Figure 3 C), linear ulcers, deep hole punch ulcers (Figure 3D), and stenosis (Figure 3E). Many other conditions may be the cause of ulcers in the small intestine, and differential diagnoses should be considered. Non steroid anti-inflammatory drugs (NSAIDs) are a common cause of lesions in the small intestine. While ulcers induced by NSAIDs can have any form, the most form most commonly seen have a diaphragm like appearance accompanied by stenosis (Figure 3F) (57). Occasionally mucosas with lesions can be seen in patients without identifiable risk factors. Although not frequently seen, when they are, they are typically rounded. Other illnesses can produce ulcers in the small intestine, so a biopsy of the affected area is preferable.
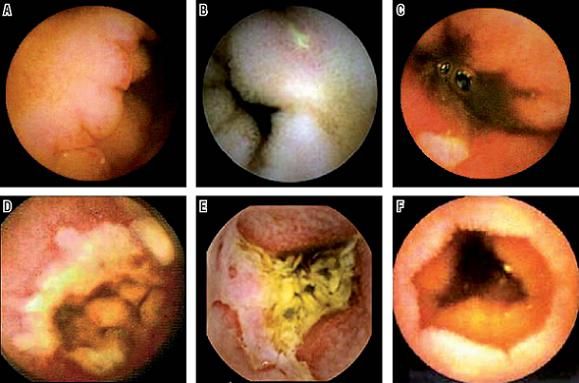
Figure 3. Findings from Capsule Endoscopy for Crohns disease and NSAID caused Enteropathies. A. Nodules in patients with known CD. B. Superficial Erosion in patients with CD. C. Superficial Ulcers in patients with CD. D. Linear Ulceration in CD. E. Deep Ulcers and Stenosis in CD. F. Diaphragms and ingestion of NSAIDs.
Capsule endoscopy can also be used to evaluate the activity and the degree of inflammation in patients with known CD (56). It is more useful for patients whose illness does not involve the terminal ileum, or for patients whose history of illness is well known after a complete resection. CE can be particularly useful in the evaluation of patients with anastomoses which are outside of the normal range of conventional endoscopy, such as Jejunal anastomoses. While there is little information available about the risk of patients retaining capsules with this procedure, it appears that this risk is higher with patients undergoing procedures outside the normal range of endoscopy than it is among other patients who undergo capsule endoscopy. Among patients who have no indications in radiographic images of the small intestine prior to undergoing CE, the rates of retention reported for patients with known cases of CD have been between 4% and 6% (58). A certain degree of individual risk for a particular patient can be estimated based on prior behavior of the illness and current symptoms. Currently consensus does not exist about whether or not x-rays should be taken of all patients with suspected or confirmed diagnoses of CD prior to capsule endoscopy. At the minimum, a careful history of the patients set of symptoms should be obtained, and this should suggest the whether or not there is any kind of obstruction. A capsule which can verify permeability and which dissolves after forty hours in the digestive tract (Agile Patency System; Given Imaging, Yoqneam, Israel) has been developed to evaluate patient risk of capsule retention (59). This device is the same size as the video capsule. It is radio-opaque and can be identified by radio frequency which permits it to be located through radiography and a sensor. It appears to be very useful for identifying patients with low risks of retaining video capsules: those whom the capsule passes completely through within the first 30 hours after ingestion are likely to have low risk for video capsule retention (60, 61). A minority of patients with stenoses report pain during the passage of the capsule. In addition a very few cases of obstruction of the small intestine, some of which required surgery, have been reported. The exact rate of these complications is not clear. Results from large series of cases which are currently being done have yet to be published (62).
Enteroscopy
Although it is more invasive than single balloon enteroscopy (SBE), double balloon enteroscopy (DBE) allows a more complete evaluation of the small intestine than does single balloon enteroscopy. It is very useful as a complement to CE. Its principal use is found in the bleeding GI tract, and it can help select groups of patients with CD. Occasionally CE or contrast x-rays can identify patients with suspected CD outside of the range of conventional endoscopy in the small intestine. For many other illnesses with similar appearances DBE with biopsy has been used as a tool for diagnostic confirmation. DBE is not necessary when the question is simply finding out the activity or extension of the illness, if the diagnosis of IBD has already been confirmed (63). Two other potential indications for DBE when patients have CD are dilation of a stenosis in the small intestine (64) and recovery of a retained video capsule (65). Nevertheless, the potential risk of perforation from this procedure must be weighed. This risk could be greater when the small intestine is inflamed. Figure 4 shows endoscopic aspects of the different phases of CD.

Figure 4. Enteroscopy in different phases of Crohns Disease. A. Superficial Jejunal Erosion in CD. B. Initial Nodular Pattern in CD. C. Jejunal Stenosis caused by CD.
Conclusions
Endoscopic biopsies remain the gold standard for diagnosis and management of patients with IBD. Endoscopy´s greatest use is for the initial evaluation of patients suspected of having IBD in order to establish an adequate diagnosis and to initiate appropriate treatment. Patients with CD can benefit from early colonoscopic or endoscopic staging of their illness and a study of the small intestine, preferably by endoscopic video capsule in addition to an ileocolonoscopy. Endoscopic biopsies are also critical for monitoring for cancer and in detection of dysplasia in patients with UC or long term CD with colitis. The application of new technology such as chromoendoscopy with staining or digital chromoendoscopy (FICE by Fuji, iScan by Pentax or NBI by Olympus) in the evaluation of dysplasia in patients with IBD requires more and better research. New technologies like capsule endoscopy and double balloon endoscopy have improved the use and yield of traditional techniques allowing a more detailed approximation of the complex management required for patients with IBD.
References
1. Anonymous. ASGE guideline: endoscopy in the diagnosis and treatment of inflammatory bowel disease. Gastrointest Endosc Clin N Am 2006; 63: 559 -65.
2. Abreu MT, Harpaz N. Diagnosis of colitis: making the initial diagnosis. Clin Gastroenterol Hepatol 2007; 5: 295-301.
3. Carbonnel F, Lavergne A, Lemann M, et al. Colonoscopy of acute colitis. A safe and reliable tool for assessment of severity. Dig Dis Sci 1994; 39: 1550-7.
4. Eaden JA MJ. British Society for Gastroenterology, Association of Coloproctology for Great Britain and Ireland. Guidelines for screening and surveillance of asymptomatic colorectal cancer in patients with inflammatory bowel disease. Gut 2002; 51: V10 -2.
5. Sandborn WJ, Tremaine WJ, Batts KP, Pemberton JH, Phillips SF. Pouchitis after ileal pouch-anal anastomosis: a Pouchitis Disease Activity Index. Mayo Clin Proc 1994; 69: 409-15.
6. Hommes DW, van Deventer SJ. Endoscopy in inflammatory bowel diseases. Gastroenterology 2004; 126: 1561-73.
7. Chutkan RK, Scherl E, Waye JD. Colonoscopy in inflammatory bowel disease. Gastrointest Endosc Clin N Am 2002; 12: 463-83, viii.
8. Higgins PD, Schwartz M, Mapili J, Zimmermann EM. Is endoscopy necessary for the measurement of disease activity in ulcerative colitis? Am J Gastroenterol 2005; 100: 355-61.
9. Castaño R, Puerta J, Álvarez O, et al. Papel de la intubación ileal rutinaria durante la colonoscopia. Rev Col Gastroenterol 2008; 23: 240-9.
10. Nikolaus S, Schreiber S. Diagnostics of inflammatory bowel disease. Gastroenterology 2007; 133: 1670-89.
11. Fefferman DS, Farrell RJ. Endoscopy in inflammatory bowel disease: indications, surveillance, and use in clinical practice. Clin Gastroenterol Hepatol 2005; 3: 11-24.
12. Bousvaros A, Morley-Fletcher A, Pensabene L, Cucchiara S. Research and clinical challenges in paediatric inflammatory bowel disease. Dig Liver Dis 2008; 40: 32-8.
13. Ladefoged K, Munck LK, Jorgensen F, Engel P. Skip inflammation of the appendiceal orifice: a prospective endoscopic study. Scand J Gastroenterol 2005; 40: 1192-6.
14. Goldstein N, Dulai M. Contemporary morphologic definition of backwash ileitis in ulcerative colitis and features that distinguish it from Crohn disease. Am J Clin Pathol 2006; 126: 365-76.
15. Simpson P, Papadakis KA. Endoscopic evaluation of patients with inflammatory bowel disease. Inflamm Bowel Dis 2008; 14: 1287-97.
16. Desai D, Faubion WA, Sandborn WJ. Review article: biological activity markers in inflammatory bowel disease. Aliment Pharmacol Ther 2007; 25: 247-55.
17. Hommes DW, Sterringa G, van Deventer SJ, Tytgat GN, Weel J. The pathogenicity of cytomegalovirus in inflammatory bowel disease: a systematic review and evidence-based recommendations for future research. Inflamm Bowel Dis 2004; 10: 245-50.
18. Rutgeerts P, Geboes K, Vantrappen G, Beyls J, Kerremans R, Hiele M. Predictability of the postoperative course of Crohns disease. Gastroenterology 1990; 99: 956-63.
19. Puerta J, Castaño R, Arismendi I. Experiencias clínico quirúrgicas con 51 bolsas ileales. Rev Col Gastroenterol 2004; 19: 78/95.
20. Shen B, Lashner BA, Bennett AE, et al. Treatment of rectal cuff inflammation (cuffitis) in patients with ulcerative colitis following restorative proctocolectomy and ileal pouch-anal anastomosis. Am J Gastroenterol 2004; 99: 1527-31.
21. Vermeire S, van Assche G, Rutgeerts P. Review article: Altering the natural history of Crohns disease--evidence for and against current therapies. Aliment Pharmacol Ther 2007; 25: 3-12.
22. Rutgeerts P. Review article: recurrence of Crohns disease after surgery - the need for treatment of new lesions. Aliment Pharmacol Ther 2006; 24 Suppl 3: 29-32.
23. Sturm A, Dignass AU. Epithelial restitution and wound healing in inflammatory bowel disease. World J Gastroenterol 2008; 14: 348-53.
24. Sipponen T, Karkkainen P, Savilahti E, et al. Correlation of faecal calprotectin and lactoferrin with an endoscopic score for Crohns disease and histological findings. Aliment Pharmacol Ther 2008; 28: 1221-9.
25. Canavan C, Abrams KR, Mayberry J. Meta-analysis: colorectal and small bowel cancer risk in patients with Crohns disease. Aliment Pharmacol Ther 2006; 23: 1097-104.
26. Itzkowitz SH, Present DH. Consensus conference: Colorectal cancer screening and surveillance in inflammatory bowel disease. Inflamm Bowel Dis 2005; 11: 314-21.
27. Kornbluth A, Sachar DB. Ulcerative colitis practice guidelines in adults (update): American College of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol 2004; 99: 1371-85.
28. Rodriguez SA, Collins JM, Knigge KL, Eisen GM. Surveillance and management of dysplasia in ulcerative colitis. Gastrointest Endosc 2007; 65: 432-9.
29. Winawer S, Fletcher R, Rex D, et al. Colorectal cancer screening and surveillance: clinical guidelines and rationale-Update based on new evidence. Gastroenterology 2003; 124: 544-60.
30. Terg R, Sambuelli A, Coronel E, et al. Prevalence of primary sclerosing cholangitis in patients with ulcerative colitis and the risk of developing malignancies. A large prospective study. Acta Gastroenterol Latinoam 2008; 38: 26-33.
31. Askling J, Dickman PW, Karlen P, et al. Family history as a risk factor for colorectal cancer in inflammatory bowel disease. Gastroenterology 2001; 120: 1356-62.
32. Gupta RB, Harpaz N, Itzkowitz S, et al. Histologic inflammation is a risk factor for progression to colorectal neoplasia in ulcerative colitis: a cohort study. Gastroenterology 2007; 133: 1099-105; quiz 340-1.
33. Rubin DT, Rothe JA, Hetzel JT, Cohen RD, Hanauer SB. Are dysplasia and colorectal cancer endoscopically visible in patients with ulcerative colitis? Gastrointest Endosc 2007; 65: 998-1004.
34. Ahmadi A, Polyak S, Draganov PV. Colorectal cancer surveillance in inflammatory bowel disease: the search continues. World J Gastroenterol 2009; 15: 61-6.
35. Lutgens MW, Vleggaar FP, Schipper ME, et al. High frequency of early colorectal cancer in inflammatory bowel disease. Gut 2008; 57: 1246-51.
36. Nguyen GC, Frick KD, Dassopoulos T. Medical decision analysis for the management of unifocal, flat, low-grade dysplasia in ulcerative colitis. Gastrointest Endosc 2009.
37. Rubin DT. An updated approach to dysplasia in IBD. J Gastrointest Surg 2008; 12: 2153-6.
38. Connell WR, Lennard-Jones JE, Williams CB, Talbot IC, Price AB, Wilkinson KH. Factors affecting the outcome of endoscopic surveillance for cancer in ulcerative colitis. Gastroenterology 1994; 107: 934-44.
39. Rubin PH, Friedman S, Harpaz N, et al. Colonoscopic polypectomy in chronic colitis: conservative management after endoscopic resection of dysplastic polyps. Gastroenterology 1999; 117: 1295-300.
40. Engelsgjerd M, Farraye FA, Odze RD. Polypectomy may be adequate treatment for adenoma-like dysplastic lesions in chronic ulcerative colitis. Gastroenterology 1999; 117: 1288-94; discussion 488-91.
41. Kiesslich R, Fritsch J, Holtmann M, et al. Methylene blue-aided chromoendoscopy for the detection of intraepithelial neoplasia and colon cancer in ulcerative colitis. Gastroenterology 2003; 124: 880-8.
42. Kiesslich R, Goetz M, Lammersdorf K, et al. Chromoscopy-guided endomicroscopy increases the diagnostic yield of intraepithelial neoplasia in ulcerative colitis. Gastroenterology 2007; 132: 874-82.
43. Rutter MD, Saunders BP, Schofield G, Forbes A, Price AB, Talbot IC. Pancolonic indigo carmine dye spraying for the detection of dysplasia in ulcerative colitis. Gut 2004; 53: 256-60.
44. Messmann H, Endlicher E, Freunek G, Rummele P, Scholmerich J, Knuchel R. Fluorescence endoscopy for the detection of low and high grade dysplasia in ulcerative colitis using systemic or local 5-aminolaevulinic acid sensitisation. Gut 2003; 52: 1003-7.
45. Dekker E, van den Broek FJ, Reitsma JB, et al. Narrow-band imaging compared with conventional colonoscopy for the detection of dysplasia in patients with longstanding ulcerative colitis. Endoscopy 2007; 39: 216-21.
46. Emura F, Saito Y, Ikematsu H. Narrow-band imaging optical chromocolonoscopy: advantages and limitations. World J Gastroenterol 2008; 14: 4867-72.
47. Kudo T, Matsumoto T, Esaki M, Yao T, Iida M. Mucosal vascular pattern in ulcerative colitis: observations using narrow band imaging colonoscopy with special reference to histologic inflammation. Int J Colorectal Dis 2009; 24: 495-501.
48. Ferlitsch A, Reinisch W, Puspok A, et al. Safety and efficacy of endoscopic balloon dilation for treatment of Crohns disease strictures. Endoscopy 2006; 38: 483-7.
49. Koltun WA. Endoscopic dilatation in Crohns disease. Aliment Pharmacol Ther 2008; 27: 994-5; author reply 5.
50. Erkelens GW, van Deventer SJ. Endoscopic treatment of strictures in Crohns disease. Best Pract Res Clin Gastroenterol 2004; 18: 201-7.
51. Brooker JC, Beckett CG, Saunders BP, Benson MJ. Long-acting steroid injection after endoscopic dilation of anastomotic Crohns strictures may improve the outcome: a retrospective case series. Endoscopy 2003; 35: 333-7.
52. Triester SL, Leighton JA, Leontiadis GI, et al. A meta-analysis of the yield of capsule endoscopy compared to other diagnostic modalities in patients with non-structuring small bowel Crohns disease. Am J Gastroenterol 2006; 101: 954-64.
53. Maunoury V, Savoye G, Bourreille A, et al. Value of wireless capsule endoscopy in patients with indeterminate colitis (inflammatory bowel disease type unclassified). Inflamm Bowel Dis 2007; 13: 152-5.
54. Reese GE, Lovegrove RE, Tilney HS, et al. The effect of Crohns disease on outcomes after restorative proctocolectomy. Dis Colon Rectum 2007; 50: 239-50.
55. Mehdizadeh S, Chen G, Enayati PJ, et al. Diagnostic yield of capsule endoscopy in ulcerative colitis and inflammatory bowel disease of unclassified type (IBDU). Endoscopy 2008; 40: 30-5.
56. Papadakis KA, Lo SK, Fireman Z, Hollerbach S. Wireless capsule endoscopy in the evaluation of patients with suspected or known Crohns disease. Endoscopy 2005; 37: 1018-22.
57. Kelly ME, McMahon LE, Jaroszewski DE, Yousfi MM, De Petris G, Swain JM. Small-bowel diaphragm disease: seven surgical cases. Arch Surg 2005; 140: 1162-6.
58. Cheifetz AS, Kornbluth AA, Legnani P, et al. The risk of retention of the capsule endoscope in patients with known or suspected Crohns disease. Am J Gastroenterol 2006; 101: 2218-22.
59. Spada C, Riccioni ME, Costamagna G. The new, dissolving patency capsule: a safe and effective tool to avoid the complication of retained video capsules. J Clin Gastroenterol 2008; 42: 761-2.
60. Postgate AJ, Burling D, Gupta A, Fitzpatrick A, Fraser C. Safety, reliability and limitations of the given patency capsule in patients at risk of capsule retention: a 3-year technical review. Dig Dis Sci 2008; 53: 2732-8.
61. Herrerias JM, Leighton JA, Costamagna G, et al. Agile patency system eliminates risk of capsule retention in patients with known intestinal strictures who undergo capsule endoscopy. Gastrointest Endosc 2008; 67: 902-9.
62. Ho KK, Joyce AM. Complications of capsule endoscopy. Gastrointest Endosc Clin N Am 2007; 17: 169-78, viii-ix.
63. Mensink PB, Groenen MJ, van Buuren HR, Kuipers EJ, van der Woude CJ. Double-balloon enteroscopy in Crohns disease patients suspected of small bowel activity: findings and clinical impact. J Gastroenterol 2009; 44: 271-6.
64. Pohl J, May A, Nachbar L, Ell C. Diagnostic and therapeutic yield of push-and-pull enteroscopy for symptomatic small bowel Crohns disease strictures. Eur J Gastroenterol Hepatol 2007; 19: 529-34.
65. Kita H, Yamamoto H, Yano T, et al. Double balloon endoscopy in two hundred fifty cases for the diagnosis and treatment of small intestinal disorders. Inflammopharmacology 2007; 15: 74-7.
1. Anonymous. ASGE guideline: endoscopy in the diagnosis and treatment of inflammatory bowel disease. Gastrointest Endosc Clin N Am 2006; 63: 559 -65. [ Links ]
2. Abreu MT, Harpaz N. Diagnosis of colitis: making the initial diagnosis. Clin Gastroenterol Hepatol 2007; 5: 295-301. [ Links ]
3. Carbonnel F, Lavergne A, Lemann M, et al. Colonoscopy of acute colitis. A safe and reliable tool for assessment of severity. Dig Dis Sci 1994; 39: 1550-7. [ Links ]
4. Eaden JA MJ. British Society for Gastroenterology, Association of Coloproctology for Great Britain and Ireland. Guidelines for screening and surveillance of asymptomatic colorectal cancer in patients with inflammatory bowel disease. Gut 2002; 51: V10 -2. [ Links ]
5. Sandborn WJ, Tremaine WJ, Batts KP, Pemberton JH, Phillips SF. Pouchitis after ileal pouch-anal anastomosis: a Pouchitis Disease Activity Index. Mayo Clin Proc 1994; 69: 409-15. [ Links ]
6. Hommes DW, van Deventer SJ. Endoscopy in inflammatory bowel diseases. Gastroenterology 2004; 126: 1561-73. [ Links ]
7. Chutkan RK, Scherl E, Waye JD. Colonoscopy in inflammatory bowel disease. Gastrointest Endosc Clin N Am 2002; 12: 463-83, viii. [ Links ]
8. Higgins PD, Schwartz M, Mapili J, Zimmermann EM. Is endoscopy necessary for the measurement of disease activity in ulcerative colitis? Am J Gastroenterol 2005; 100: 355-61. [ Links ]
9. Castaño R, Puerta J, Álvarez O, et al. Papel de la intubación ileal rutinaria durante la colonoscopia. Rev Col Gastroenterol 2008; 23: 240-9. [ Links ]
10. Nikolaus S, Schreiber S. Diagnostics of inflammatory bowel disease. Gastroenterology 2007; 133: 1670-89. [ Links ]
11. Fefferman DS, Farrell RJ. Endoscopy in inflammatory bowel disease: indications, surveillance, and use in clinical practice. Clin Gastroenterol Hepatol 2005; 3: 11-24. [ Links ]
12. Bousvaros A, Morley-Fletcher A, Pensabene L, Cucchiara S. Research and clinical challenges in paediatric inflammatory bowel disease. Dig Liver Dis 2008; 40: 32-8. [ Links ]
13. Ladefoged K, Munck LK, Jorgensen F, Engel P. Skip inflammation of the appendiceal orifice: a prospective endoscopic study. Scand J Gastroenterol 2005; 40: 1192-6. [ Links ]
14. Goldstein N, Dulai M. Contemporary morphologic definition of backwash ileitis in ulcerative colitis and features that distinguish it from Crohn disease. Am J Clin Pathol 2006; 126: 365-76. [ Links ]
15. Simpson P, Papadakis KA. Endoscopic evaluation of patients with inflammatory bowel disease. Inflamm Bowel Dis 2008; 14: 1287-97. [ Links ]
16. Desai D, Faubion WA, Sandborn WJ. Review article: biological activity markers in inflammatory bowel disease. Aliment Pharmacol Ther 2007; 25: 247-55. [ Links ]
17. Hommes DW, Sterringa G, van Deventer SJ, Tytgat GN, Weel J. The pathogenicity of cytomegalovirus in inflammatory bowel disease: a systematic review and evidence-based recommendations for future research. Inflamm Bowel Dis 2004; 10: 245-50. [ Links ]
18. Rutgeerts P, Geboes K, Vantrappen G, Beyls J, Kerremans R, Hiele M. Predictability of the postoperative course of Crohns disease. Gastroenterology 1990; 99: 956-63. [ Links ]
19. Puerta J, Castaño R, Arismendi I. Experiencias clínico quirúrgicas con 51 bolsas ileales. Rev Col Gastroenterol 2004; 19: 78/95. [ Links ]
20. Shen B, Lashner BA, Bennett AE, et al. Treatment of rectal cuff inflammation (cuffitis) in patients with ulcerative colitis following restorative proctocolectomy and ileal pouch-anal anastomosis. Am J Gastroenterol 2004; 99: 1527-31. [ Links ]
21. Vermeire S, van Assche G, Rutgeerts P. Review article: Altering the natural history of Crohns disease--evidence for and against current therapies. Aliment Pharmacol Ther 2007; 25: 3-12. [ Links ]
22. Rutgeerts P. Review article: recurrence of Crohns disease after surgery - the need for treatment of new lesions. Aliment Pharmacol Ther 2006; 24 Suppl 3: 29-32. [ Links ]
23. Sturm A, Dignass AU. Epithelial restitution and wound healing in inflammatory bowel disease. World J Gastroenterol 2008; 14: 348-53. [ Links ]
24. Sipponen T, Karkkainen P, Savilahti E, et al. Correlation of faecal calprotectin and lactoferrin with an endoscopic score for Crohns disease and histological findings. Aliment Pharmacol Ther 2008; 28: 1221-9. [ Links ]
25. Canavan C, Abrams KR, Mayberry J. Meta-analysis: colorectal and small bowel cancer risk in patients with Crohns disease. Aliment Pharmacol Ther 2006; 23: 1097-104. [ Links ]
26. Itzkowitz SH, Present DH. Consensus conference: Colorectal cancer screening and surveillance in inflammatory bowel disease. Inflamm Bowel Dis 2005; 11: 314-21. [ Links ]
27. Kornbluth A, Sachar DB. Ulcerative colitis practice guidelines in adults (update): American College of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol 2004; 99: 1371-85. [ Links ]
28. Rodriguez SA, Collins JM, Knigge KL, Eisen GM. Surveillance and management of dysplasia in ulcerative colitis. Gastrointest Endosc 2007; 65: 432-9. [ Links ]
29. Winawer S, Fletcher R, Rex D, et al. Colorectal cancer screening and surveillance: clinical guidelines and rationale-Update based on new evidence. Gastroenterology 2003; 124: 544-60. [ Links ]
30. Terg R, Sambuelli A, Coronel E, et al. Prevalence of primary sclerosing cholangitis in patients with ulcerative colitis and the risk of developing malignancies. A large prospective study. Acta Gastroenterol Latinoam 2008; 38: 26-33. [ Links ]
31. Askling J, Dickman PW, Karlen P, et al. Family history as a risk factor for colorectal cancer in inflammatory bowel disease. Gastroenterology 2001; 120: 1356-62. [ Links ]
32. Gupta RB, Harpaz N, Itzkowitz S, et al. Histologic inflammation is a risk factor for progression to colorectal neoplasia in ulcerative colitis: a cohort study. Gastroenterology 2007; 133: 1099-105; quiz 340-1. [ Links ]
33. Rubin DT, Rothe JA, Hetzel JT, Cohen RD, Hanauer SB. Are dysplasia and colorectal cancer endoscopically visible in patients with ulcerative colitis? Gastrointest Endosc 2007; 65: 998-1004. [ Links ]
34. Ahmadi A, Polyak S, Draganov PV. Colorectal cancer surveillance in inflammatory bowel disease: the search continues. World J Gastroenterol 2009; 15: 61-6. [ Links ]
35. Lutgens MW, Vleggaar FP, Schipper ME, et al. High frequency of early colorectal cancer in inflammatory bowel disease. Gut 2008; 57: 1246-51. [ Links ]
36. Nguyen GC, Frick KD, Dassopoulos T. Medical decision analysis for the management of unifocal, flat, low-grade dysplasia in ulcerative colitis. Gastrointest Endosc 2009. [ Links ]
37. Rubin DT. An updated approach to dysplasia in IBD. J Gastrointest Surg 2008; 12: 2153-6. [ Links ]
38. Connell WR, Lennard-Jones JE, Williams CB, Talbot IC, Price AB, Wilkinson KH. Factors affecting the outcome of endoscopic surveillance for cancer in ulcerative colitis. Gastroenterology 1994; 107: 934-44. [ Links ]
39. Rubin PH, Friedman S, Harpaz N, et al. Colonoscopic polypectomy in chronic colitis: conservative management after endoscopic resection of dysplastic polyps. Gastroenterology 1999; 117: 1295-300. [ Links ]
40. Engelsgjerd M, Farraye FA, Odze RD. Polypectomy may be adequate treatment for adenoma-like dysplastic lesions in chronic ulcerative colitis. Gastroenterology 1999; 117: 1288-94; discussion 488-91. [ Links ]
41. Kiesslich R, Fritsch J, Holtmann M, et al. Methylene blue-aided chromoendoscopy for the detection of intraepithelial neoplasia and colon cancer in ulcerative colitis. Gastroenterology 2003; 124: 880-8. [ Links ]
42. Kiesslich R, Goetz M, Lammersdorf K, et al. Chromoscopy-guided endomicroscopy increases the diagnostic yield of intraepithelial neoplasia in ulcerative colitis. Gastroenterology 2007; 132: 874-82. [ Links ]
43. Rutter MD, Saunders BP, Schofield G, Forbes A, Price AB, Talbot IC. Pancolonic indigo carmine dye spraying for the detection of dysplasia in ulcerative colitis. Gut 2004; 53: 256-60. [ Links ]
44. Messmann H, Endlicher E, Freunek G, Rummele P, Scholmerich J, Knuchel R. Fluorescence endoscopy for the detection of low and high grade dysplasia in ulcerative colitis using systemic or local 5-aminolaevulinic acid sensitisation. Gut 2003; 52: 1003-7. [ Links ]
45. Dekker E, van den Broek FJ, Reitsma JB, et al. Narrow-band imaging compared with conventional colonoscopy for the detection of dysplasia in patients with longstanding ulcerative colitis. Endoscopy 2007; 39: 216-21. [ Links ]
46. Emura F, Saito Y, Ikematsu H. Narrow-band imaging optical chromocolonoscopy: advantages and limitations. World J Gastroenterol 2008; 14: 4867-72. [ Links ]
47. Kudo T, Matsumoto T, Esaki M, Yao T, Iida M. Mucosal vascular pattern in ulcerative colitis: observations using narrow band imaging colonoscopy with special reference to histologic inflammation. Int J Colorectal Dis 2009; 24: 495-501. [ Links ]
48. Ferlitsch A, Reinisch W, Puspok A, et al. Safety and efficacy of endoscopic balloon dilation for treatment of Crohns disease strictures. Endoscopy 2006; 38: 483-7. [ Links ]
49. Koltun WA. Endoscopic dilatation in Crohns disease. Aliment Pharmacol Ther 2008; 27: 994-5; author reply 5. [ Links ]
50. Erkelens GW, van Deventer SJ. Endoscopic treatment of strictures in Crohns disease. Best Pract Res Clin Gastroenterol 2004; 18: 201-7. [ Links ]
51. Brooker JC, Beckett CG, Saunders BP, Benson MJ. Long-acting steroid injection after endoscopic dilation of anastomotic Crohns strictures may improve the outcome: a retrospective case series. Endoscopy 2003; 35: 333-7. [ Links ]
52. Triester SL, Leighton JA, Leontiadis GI, et al. A meta-analysis of the yield of capsule endoscopy compared to other diagnostic modalities in patients with non-structuring small bowel Crohns disease. Am J Gastroenterol 2006; 101: 954-64. [ Links ]
53. Maunoury V, Savoye G, Bourreille A, et al. Value of wireless capsule endoscopy in patients with indeterminate colitis (inflammatory bowel disease type unclassified). Inflamm Bowel Dis 2007; 13: 152-5. [ Links ]
54. Reese GE, Lovegrove RE, Tilney HS, et al. The effect of Crohns disease on outcomes after restorative proctocolectomy. Dis Colon Rectum 2007; 50: 239-50. [ Links ]
55. Mehdizadeh S, Chen G, Enayati PJ, et al. Diagnostic yield of capsule endoscopy in ulcerative colitis and inflammatory bowel disease of unclassified type (IBDU). Endoscopy 2008; 40: 30-5. [ Links ]
56. Papadakis KA, Lo SK, Fireman Z, Hollerbach S. Wireless capsule endoscopy in the evaluation of patients with suspected or known Crohns disease. Endoscopy 2005; 37: 1018-22. [ Links ]
57. Kelly ME, McMahon LE, Jaroszewski DE, Yousfi MM, De Petris G, Swain JM. Small-bowel diaphragm disease: seven surgical cases. Arch Surg 2005; 140: 1162-6. [ Links ]
58. Cheifetz AS, Kornbluth AA, Legnani P, et al. The risk of retention of the capsule endoscope in patients with known or suspected Crohns disease. Am J Gastroenterol 2006; 101: 2218-22. [ Links ]
59. Spada C, Riccioni ME, Costamagna G. The new, dissolving patency capsule: a safe and effective tool to avoid the complication of retained video capsules. J Clin Gastroenterol 2008; 42: 761-2. [ Links ]
60. Postgate AJ, Burling D, Gupta A, Fitzpatrick A, Fraser C. Safety, reliability and limitations of the given patency capsule in patients at risk of capsule retention: a 3-year technical review. Dig Dis Sci 2008; 53: 2732-8. [ Links ]
61. Herrerias JM, Leighton JA, Costamagna G, et al. Agile patency system eliminates risk of capsule retention in patients with known intestinal strictures who undergo capsule endoscopy. Gastrointest Endosc 2008; 67: 902-9. [ Links ]
62. Ho KK, Joyce AM. Complications of capsule endoscopy. Gastrointest Endosc Clin N Am 2007; 17: 169-78, viii-ix. [ Links ]
63. Mensink PB, Groenen MJ, van Buuren HR, Kuipers EJ, van der Woude CJ. Double-balloon enteroscopy in Crohns disease patients suspected of small bowel activity: findings and clinical impact. J Gastroenterol 2009; 44: 271-6. [ Links ]
64. Pohl J, May A, Nachbar L, Ell C. Diagnostic and therapeutic yield of push-and-pull enteroscopy for symptomatic small bowel Crohns disease strictures. Eur J Gastroenterol Hepatol 2007; 19: 529-34. [ Links ]
65. Kita H, Yamamoto H, Yano T, et al. Double balloon endoscopy in two hundred fifty cases for the diagnosis and treatment of small intestinal disorders. Inflammopharmacology 2007; 15: 74-7. [ Links ]

