










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.26 no.4 Bogotá Oct./Dec. 2011
Chronic hepatopathy: bleeding vs. thrombosis
Natalia Aristizábal Henao, MD (1), Camilo Alberto Madrid Muñoz, MD (1), Juan Carlos Restrepo Gutiérrez, MD, MSc, PhD. (2)
(1) Third Year Internal Medicine Resident at Universidad Pontificia Bolivariana, Department of Medicine. Medellín, Colombia.
(2) Internist and Hepatologist in the Hepatology and Liver Transplant Unit at the Hospital Pablo Tobón Uribe. Professor in the Department of Medicine and Gastro-hepatology Group at the Universidad de Antioquia in Medellín, Colombia.
Translation from Spanish to English by T.A. Zuur and The Language Workshop
Received: 05-10-11 Accepted: 11-10-11
Abstract
Coagulation alterations in patients with chronic liver disease occur frequently, although they are usually described as auto-anticoagulation phenomena. Changes in hemostasis are broad and diffuse. They include changes in procoagulant and anticoagulant substances, hemodynamic modifications, endothelial dysfunction and platelet malfunction which are the causes of different clinical conditions varying from hemorrhaging to thrombosis. Given the complexity of theses alterations, laboratory tests do not correlate well with the clinical events.
Treatment for these patients has been controversial. Currently we do not have objective methods for determining the hemostatic balance between bleeding and thrombosis in patients with chronic liver disease. In addition to this, the medical literature does not include guidelines for dealing with this special population. Also, the risk of thrombosis indicates the need to consider the use of thromboprophylaxis.
Key words
Chronic liver disease, bleeding, hemorrhaging, coagulopathy and thrombosis.
INTRODUCTION
The liver plays a very important role in the processes of coagulation, anticoagulation, and fibrinolysis; hence pathological alterations of this organ have serious implications for all of these functions.
Recognizing alterations in coagulation in patients with chronic liver disease is becoming very important because of its increasing incidence and prevalence and because it often produces bleeding and thrombosis. Unfortunately, there is little correlation between laboratory studies and clinical evidence of bleeding. Bleeding occurs frequently, especially after invasive medical procedures such as liver biopsies are done. This clinically relevant bleeding is hard to control.
Our intention here is to identify the physiopathological mechanisms that are responsible for alterations in the hemostasis of patients with chronic hepatopathy; to recognize its clinical implications; and to present recommendations for its management which take the evidence into consideration.
EPIDEMIOLOGY
Chronic liver disease is increasingly important. In 2006 it reportedly caused 112,000 hospitalizations and 27,000 deaths in the United States, a rate of 9.2 deaths per 100,000 inhabitants (1).
Traditionally, auto anticoagulation (2, 3) has been attributed to chronic liver disease, but coagulation alterations related to this disease seem to be more complex (4-6). Recent data shows an incidence of 0.5 to 1.9% of venous thromboembolism in patients with this disease.
HEMOSTASIS IN CHRONIC HEPATOPATHY
Any condition that affects liver functioning has potential repercussions for coagulation. In advanced chronic liver disease alterations in hemostasis are even more evident in both procoagulant and anticoagulant substances. Changes in coagulation, fibrinolysis, and platelet functioning processes occur (8, 9).
The main alterations in patients with chronic hepatopathy found in laboratories are:
- Prolonged prothrombin time (PT) 88%
- Prolonged partial thromboplastin time (PTT) 71%
- Thrombocytopenia 37%
- Decreased fibrinogen 15%
Some studies show that patients with variceal bleeding develop more significant abnormalities in their hemostatic systems than do patients who do not bleed (11-13). Nevertheless, estimated relative risks for digestive bleeding are significant when a patient has a low platelet count (10). This implies that laboratory tests results for these patients do not correlate very well with clinical events (14) which suggests that there are additional physiopathological mechanisms producing complex changes in the coagulation system of patients with chronic liver disease.
Case studies and control studies have tried to determine whether or not there is an imbalance in favor of procoagulant substances (15) in the plasma of cirrhotic patients. If so this would demonstrate that patients with cirrhosis generate more thrombin than produced by controls whether or not thrombomodulin is present in the control patients. This would also be evidence of resistance to thrombomodulin which is a powerful anticoagulant. Patients with chronic hepatopathy also show increased levels of factor VIII and reduced levels of natural anticoagulants such as protein C and antithrombin III (ATIII). These alterations became more evident as the liver disease becomes more severe (15).
Hypercoagulability of plasma in cirrhotic patients seems to be the result of increased levels of factor III and reduced levels of protein C concentrations which are typical features in cirrhotic patients. These alterations might explain the risk of venous thromboembolism in patients with chronic hepatopathy (15).
COAGULATION
In general terms, procoagulant factors, with the exceptions of factor VIII and von Willebrand factor (vWF), decrease in patients with chronic liver diseases. At the same time there is a reduction of natural anticoagulants like ATIII and protein C (8, 16).
Because of its relatively short life Factor VII decreases first. Its values in blood are inversely proportional to the degree of cirrhosis. In acute hepatopathy there is also a reduction of factors II, V, and X, and in chronic hepatopathy there is an additional loss of factors IX and XI. Fibrinogen levels are normal in stable liver disease, but they decrease as the hepatopathy becomes more severe.
Given these alterations in the hemostasis of patients with chronic liver disease, it is not surprising to think that isolated measurement of PT is inappropriate for measuring the coagulation condition of these patients. PT only measures the time required for thrombin formation which does relate to procoagulant factors, but its reagents ignore the role of thrombomodulin and the activation of protein C which are also altered in these patients. The result is that thrombin may form even when thrombomodulin is present (8, 16). Consequently, the International Normalized Ratio (INR) turns out to be inadequate. It is important to underline that this test has been validated by measurement of subjects who receive substances which are antagonistic to vitamin K. PTs reagents are not designed for patients with chronic hepatopathy. However, INR is one of the main scores that indicates the severity of the disease (8, 16).
PLATELETS
Under normal conditions platelets have a dual function in the coagulation process: participating in primary hemostasis by sticking to the vascular wall when interacting with VWF, and generating thrombin (7). Their adhesion to the vascular wall by interaction with VWF subsequently allows platelet aggregation and formation of soft primary clots. Platelets participate in the generation of thrombin by adhesion of activated coagulation factors to their surface.
Patients with chronic liver disease show thrombocytopenia, high levels of VWF and reduction of ADAMS 13 (7).
Due to alterations in VWF and ADAMS 13, platelet levels as low as 60,000 platelet /mm3 can be functional and maintain thrombin generation. Nevertheless, the platelet count is directly related to the generation of thrombin (7).
Thrombocytopenia develops because of:
- Splenomegaly
- Bone marrow suppression
- Reduced thrombopoietin
- Platelet destruction by immunological mediation
FIBRINOLYSIS
Fibrinolysis is the process responsible for conversion of plasminogen into plasmin. Through this process clots are destroyed and bleeding occurs. It has been said that patients with chronic hepatopathy suffer a hyperfibrinolysis state which has not yet been measured by the balance of the whole system but only by measuring individual components (7). Clinical studies have yet to clearly show the participation of hyperfibrinolysis in bleeding.
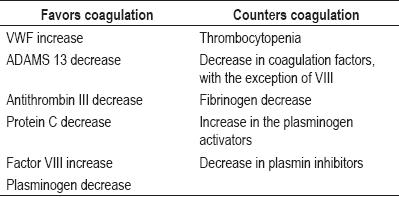
Until this point we have alterations in patients with chronic hepatopathy that favor bleeding and thrombosis (Table 1). The balance can tilt one way or the other depending on the degree of liver insufficiency (2).
Table 1. Factors that alter coagulation in patients withchronic hepatopathy.
The tendency of patients with liver disease to bleed cannot be explained solely by alterations in hemostasis. A partially explanation of hemorrhagic events in patients with decompensated liver disease is provided by haemodynamic alterations such as portal hypertension, endothelial dysfunction, kidney dysfunction, and production of substances similar to heparin released by bacterial infections (8, 16-19).
Decreases of factors favoring coagulation in cirrhotic patients are offset by reductions of anticoagulant factors. These findings help clarify the pathophysiology of hemostasis in cirrhosis and suggest that bleeding is mediated by additional factors that conventional lab tests do not completely reflect the coagulation condition of these patients. In conclusion, although thrombin generation is normal in cirrhosis (20), generation of thrombin also depends upon platelet function. Severe thrombocytopenia (platelet count lower than 50,000/mm3) can limit thrombin generation in patients with cirrhosis (21). These findings justify platelet transfusion in cases in which thrombocytopenia becomes severe and patient is at high risk for bleeding when patients are going to undergo surgery or liver biopsy (3, 21). In these cases use of fresh frozen plasma (FFP) is contraindicated because it is not exempt from risks of complications (21).
Besides the already known risk of bleeding in patients with chronic liver disease, we have very little clinical data about management of this the condition. There are no medical guides for treatment or prevention of bleeding in this patient population (2). There are some centers that support the strategy of waiting and acting which means using only blood components in case of bleeding. Others defend prophylactic transfusions, the effectiveness of which has not yet been demonstrated (22).
Other therapeutic options to be considered for a patient with chronic hepatology include recombinant factor VIIa, prothrombin concentrate, antifibrinolytic agents, and desmopressin (2). Although factor VIIa is very effective in normalizing in prolonged PT in patients with liver disease (23), controlled clinical trials have failed to demonstrate the effectiveness of this drug in reducing blood loss during liver surgery on patients with cirrhosis (24-26) or variceal bleeding (27), and some data suggest that this drug could have thrombogenic potential (28). Experience using prothrombin concentrate for chronic hepatopathy is limited (2). Although antifibrinolytic agents such as tranexamic acid have reduced bleeding during liver transplant procedures (29), there are no studies that demonstrate its usefulness in preventing spontaneous blood loss or blood loss in other types of procedures. Desmopressin has demonstrated effectiveness in improving primary hemostasis according to laboratory parameters (30), but there is not much data regarding its clinical efficacy (2).
Consequently, it is clear that using PT and PPT as isolated laboratory tests to evaluate hemostasis in patients with chronic hepatopathy is inadequate (3). Currently we do not have laboratory tests that can simultaneously evaluate the balance between procoagulant and anticoagulant factors in vivo (20).
Nevertheless, it is possible to calculate the rate of thrombin generation when thrombomodulin is present and when it is absent. It has a negative correlation with levels of protein C, and a positive correlation with levels of factor VIII. Its clinical meaning is not clear yet (8). As the rate increases, the degree of hemostatic alterations also increase favoring a procoagulant state. Its value will increase as the severity of hemostasis increases (8).
Thromboelastography is a dynamic test that evaluates the process of thrombosis. It has been used as a guide for transfusions during transplants, but it is not yet clear if its results predict thrombotic or hemorrhagic complications in cirrhosis (16).
THROMBOSIS IN CHRONIC HEPATOPATHY
Not all haemostatic alterations in patients with hepatopathy favor bleeding. Increased thrombotic risk explains frequent thrombosis in the portal venous system where there is higher risk for patients with thrombophilia (8, 31-33). In addition, conditions such as fatty liver disease, non alcoholic steatohepatitis (NASH), and metabolic syndrome result in states favorable to coagulation.
As mentioned above, patients with chronic hepatopathy have partial resistance to thrombomodulin which is explained by increased factor VIII levels and decreased liver production which reduces levels of protein C and reduces purification of VWF, the protein related to the LDL receptor (8).
Factor VIII is one of the most powerful activators of thrombin generation. Reduction in the purification of factor VIII is mediated by two mechanisms. On one hand high levels of VWF cause it to combine with plasma and protect it from degradation by proteases. On the other hand, the protein related to the LDL receptor, which is in charge of its reception for intercellular degradation, is inadequately expressed in patients with cirrhosis (8).
Fibrosis in chronic liver disease is a consequence of a procoagulable state. It is a process known as parenchymal extinction produced by focal ischemia (34), in which proteases participate in coagulation through the activation of stellate cells (35-37). Patients in states of hypercoagulability, for instance when Leiden factor V is present, have accelerated liver fibrosis. Proposed mechanisms include the appearance of microthrombi in liver and portal veins. These are cellular effects of thrombin mediated by receptors in the stellate cells and by platelet activation (8). The expression of thrombin receptors in stellate cells increases as the liver disease worsens, and it is well known that platelet activation favors progression of fibrosis due to a mechanism with immunological mediation which is evident in animal models with viral hepatitis (8).
PORTAL VEIN THROMBOSIS
The prevalence of portal vein thrombosis increases as the disease becomes more severe (38). This occurs in 1% of patients with compensated cirrhosis and in up to 25% of candidates for liver transplant. The mechanism for thrombosis seems to be mainly mediated by the reduction of protein C, by reduction in the speed of the portal flow, and by abnormalities in the vascular wall.
As the hepatopathy becomes more severe, natural anticoagulant values decrease. However, when factors of confusion are adjusted for, natural anticoagulant values do not seem to predict portal vein thrombosis. The only predictor is reduction in the speed of the portal flow (39). Development of portal vein thrombosis in these patients is independently associated with reduction of proteins C and S and an increase in D-dimer (40). It is not clear if these changes are risk factors or a direct consequence of the acute thrombotic event.
The use of warfarin as an anticoagulant is not ideal because it is antagonistic to vitamin K which could become antagonistic to the small amount of protein C available thus increasing the risk of thrombosis (8).
ARTERIAL THROMBOSIS
Patients with chronic liver disease could develop atherothrombosis. It is not clear if there is an increased risk of coronary heart disease or stroke in these cases (8).
Arterial events such as the obstruction of the hepatic artery following liver transplantation worsen the prognosis. They seem to be related to a hypercoagulable state in the postoperative period (41). Controlled clinical studies should be performed to assess the need for using antiplatelet agents as primary prophylaxis.
A higher frequency of arterial thrombotic events has been found in patients with NASH (2). Similar findings have recently been reported in patients with hepatopathy of alcoholic origin (42).
PERIPHERAL VENOUS THROMBOSIS
Patients with advanced liver disease are not anticoagulated as was once thought. Thrombotic events may occur even when laboratory tests suggest risk of bleeding.
The risk of venous thromboembolism (VTE) in patients with chronic hepatopathy is difficult to determine by looking at laboratory studies retrospectively. Higher incidences of thrombosis can be explained by longer lives and changes in life style which are marked by physical inactivity (8).
There is a higher incidence of thrombotic events among patients with cirrhosis than among patients without cirrhosis (43), but its incidence among patients with cirrhosis is lower than among patients with kidney failure, heart failure and cancer (44).
The incidence of thrombotic events among patients with cirrhosis is between 0.9% and 1.8% (44). Among hospitalized patients the reported figures are between 0.5% (45) and 6.3% (1). Two thirds of the cases are reported as deep vein thrombosis (DVT), 20% as pulmonary embolisms (PEs) and 15% as combined forms (45).
Platelet count, the severity of the underlying liver disease, and other classical factors for thrombotic risk are not good predictors for DVT and PE in this population. Albumin is an independent predictor of thrombotic risk in cirrhotic patients that probably reflects reduced protein production, which also includes natural anticoagulants (44, 45). There are no statistically significant differences regarding the presence of thrombotic events according to INR base values in patients with hepatopathy (1).
It is of concern that thromboprophylaxis was not used for 75% of the patients with chronic liver disease that presented venous thrombosis (1). Standard thromboprophylaxis should be extended to patients with chronic hepatopathy, at least for those exposed to situations of high risk for thrombosis, such as hospitalization, prolonged immobilization or significant surgical procedures (1, 46). Existing guides for thromboprophylaxis do not consider chronic liver disease as a risk factor for thrombosis (47).
The only recommendation for treatment of thrombotic events in patients with hepatopathy is to use small doses of oral anticoagulants. Duration of the treatment should be guided according to the underlying cause (49). There are no differences in INR goals for anticoagulation or suggestions for the use of another kind of anticoagulant. This is because of the difficulty of monitoring antagonistic elements to vitamin K when prolonged PPT values are taken a starting point and because of the unpredictable results from using heparin given that its action directly involves decreased antithrombin III in this population (2). Studies are needed about the effectiveness and safety of using direct thrombin inhibitors and the Xa factor under these circumstances.
Risks and benefits of anticoagulant therapy in patients with thrombosis and portal hypertension should be assessed considering the possibility of thrombosis and recurrence of variceal bleeding. Data from studies to date are contradictory. Esophageal varices should be screened and treated according to guidelines for dealing with cirrhosis (48). There is limited data about the usefulness of thrombophilia screening and about the benefits of anticoagulation in patients with well compensated cirrhosis and acute or chronic portal venous thrombosis. Each case should be treated individually (49, 50).
CONCLUSION
Chronic hepatopathy is not only a clinical condition of hypocoagulability. Changes in hemostasis include procoagulant and anticoagulant alterations which explain why clinically evident bleeding does not only depend upon changes in coagulation but also upon hemodynamic modifications, endothelial dysfunction, bacterial infection, and kidney failure. In addition, there is a risk for thrombosis which reveals the need to consider the use of thromboprophylaxis in these patients and to revise the guidelines regarding anticoagulation in this special population.
REFERENCES
1. Ousama Dabbagh, Aabha Oza, Sumi Prakash, Ramez Sunna, Timothy M Saettele. Coagulopathy does not protect against Venous Thromboembolism in Hospitalized Patients with Chronic Liver Disease. Chest 2010; 137(5): 1145-1149.
2. Ton Lisman, Stephen H Caldwell, Andrew K Burroughs, Patrick G Northup, Marco Senzolo R, Todd Stravitz, Armando Tripodi, James F Trotter, Dominique-Charles Valla, Robert J Porte. Hemostasis and thrombosis in patients with liver disease: The ups and downs. Journal of Hepatology 2010; 53: 362-371.
3. Armando Tripodi. The coagulopathy of chronic liver disease: Is there a causal relationship with bleeding? No. European Journal of Internal Medicine 2010; 21: 65-69.
4. Stefania Basili, Valeria Raparelli, Francesco Violi. The coagulopathy of chronic liver disease: Is there a causal relationship with bleeding? Yes. European Journal of Internal Medicine 2010; 21: 62-64.
5. Reverter JC. Abnormal hemostasis tests and bleeding in chronic liver disease: are they related? Yes. J Thromb Haemost 2006; 4: 717-20.
6. Senzolo M, Burra P, Cholongitas E, Burroughs AK. New insights into the coagulopathy of liver disease and liver transplantation. World J Gastroenterol 2006; 12: 7725-36.
7. Giuseppe Lippi, Giovanni Targher, Emmanuel J. Favaloro, Massimo Franchini. Venous Thromboembolism in Chronic Liver Disease. Seminars in Thrombosis and Hemostasis 2011; 37(1).
8. Armando Tripodi, Pier Mannuccio Mannucci. The Coagulopathy of Chronic Liver Disease. N Engl Med 2011; 365: 147-56.
9. Bosch J, Reverter JC. The coagulopathy of cirrhosis: myth or reality? Hepatology 2005; 41: 434-5.
10. Sohail Ahmed Siddiqui, Mubashir Ahmed, Muhammad Hanif Ghani, Muhammad Anwar Memon, Ghulam Mustafa, Muhammad Aslam Ghori. Coagulation abnormalities in patients with chronic liver disease in Pakistan. JPMA 2011; 61: 363.
11. Violi F, Leo R, Basili S, Ferro D, Cordova C, Balsano F. Association between prolonged bleeding time and gastrointestinal hemorrhage in 102 patients with liver cirrhosis: results of a retrospective study. Haematologica 1994; 79: 61-65.
12. Violi F, Ferro D, Basili S, Quintarelli C, Saliola M, Alessandri C, et al. Hyperfibrinolysis increases the risk of gastrointestinal hemorrhage in patients with advanced cirrhosis. Hepatology 1992; 15: 672-676.
13. Tacke F, Fiedler K, Trautwein C. A simple clinical score predicts high risk for upper gastrointestinal hemorrhages from varices in patients with chronic liver disease. Scand J Gastroenterol 2007; 42: 374-382.
14. Basili S, Ferro D, Leo R, Juliano L, Alessandri C, Cordova C, et al. Bleeding time does not predict gastrointestinal bleeding in patients with cirrhosis. The CALC Group. Coagulation Abnormalities in Liver Cirrhosis. J Hepatol 1996; 24: 574-80.
15. Armando Tripodi, Massimo Primignani, Veena Chantarangkul, Alessandra Dellera, Marigrazia Clerici, Roberto De Franchis, Massimo Colombo, Pier Mannuccio Mannucci. An Imbalance of Pro- vs. Anti-Coagulation Factors in Plasma from Patients with Cirrhosis. Gastroenterology 2009; 137: 2105-2111.
16. Alexander Hodge, Philip Crispin. Coagulopathy in liver disease: The whole is greater than the sum of its parts. J. Gastroenterol. Hepatol 2010; 25: 116-121.
17. Sharara AI, Rockey DC. Gastroesophageal variceal hemorrhage. N Engl J Med 2001; 345: 669-681.
18. Montalto P, Vlachogiannakos J, Cox DJ, Pastacaldi S, Patch D, Burroughs AK. Bacterial infection in cirrhosis impairs coagulation by a heparin effect: a prospective study. J Hepatol 2002; 37: 463-470.
19. Senzolo M, Coppell J, Cholongitas E, Riddell A, Triantos CK, Perry D, et al. The effects of glycosaminoglycans on coagulation: a thromboelastographic study. Blood Coagul Fibrinolysis 2007; 18: 227-236.
20. Armando Tripodi, Francesco Salerno, Veena Chantarangkul, Marigrazia Clerici, Massimo Cazzaniga, Massimo Primignani, Pier Mannuccio Mannucci. Evidence of Normal Thrombin Generation in Cirrhosis despite Abnormal Conventional Coagulation Tests. Hepatology 2005; 41: 553-558.
21. Armando Tripodi, Massimo Primignani, Veena Chantarangkul, Marigrazia Clerici, Alessandra DellEra, Federica Fabris, Francesco Salerno, Pier Mannuccio Mannucci. Thrombin Generation in Patients with Cirrhosis: The Role of Platelets. Hepatology 2006; 44: 440-445.
22. Segal JB, Dzik WH. Paucity of studies to support that abnormal coagulation test results predict bleeding in the setting of invasive procedures: an evidence-based review. Transfusion 2005; 45: 1413-1425.
23. Bernstein DE, Jeffers L, Erhardtsen E, Reddy KR, Glazer S, Squiban P, et al. Recombinant factor VIIa corrects prothrombin time in cirrhotic patients: a preliminary study. Gastroenterology 1997; 113: 1930-1937.
24. Lodge JP, Jonas S, Oussoultzoglou E, Malago M, Jayr C, Cherqui D, et al. Recombinant coagulation factor VIIa in major liver resection: a randomized, placebo-controlled, double-blind clinical trial. Anesthesiology 2005; 102: 269-275.
25. Lodge JP, Jonas S, Jones RM, Olausson M, Mir-Pallardo J, Soefelt S, et al. Efficacy and safety of repeated perioperative doses of recombinant factor VIIa in liver transplantation. Liver Transplant 2005; 11: 973-979.
26. Planinsic RM, van der MJ, Testa G, Grande L, Candela A, Porte RJ, et al. Safety and efficacy of a single bolus administration of recombinant factor VIIa in liver transplantation due to chronic liver disease. Liver Transplant 2005; 11: 895-900.
27. Bosch J, Thabut D, Albillos A, Carbonell N, Spicak J, Massard J, et al. Recombinant factor VIIa for variceal bleeding in patients with advanced cirrhosis: a randomized, controlled trial. Hepatology 2008; 47: 1604-1614.
28. OConnell KA, Wood JJ, Wise RP, Lozier JN, Braun MM. Thromboembolic adverse events after use of recombinant human coagulation factor VIIa. JAMA 2006; 295: 293-298.
29. Boylan JF, Klinck JR, Sandler AN, Arellano R, Greig PD, Nierenberg H, et al. Tranexamic acid reduces blood loss, transfusion requirements, and coagulation factor use in primary orthotopic liver transplantation. Anesthesiology 1996; 85: 1043-1048.
30. Agnelli G, Parise P, Levi M, Cosmi B, Nenci GG. Effects of desmopressin on hemostasis in patients with liver cirrhosis. Haemostasis 1995; 25: 241-247.
31. Valla DC. Thrombosis and anticoagulation in liver disease. Hepatology 2008; 47: 1384-93.
32. Okuda K, Ohnishi K, Kimura K, et al. Incidence of portal vein thrombosis in liver cirrhosis. An angiographic study in 708 patients. Gastroenterology 1985; 89: 279-86.
33. Amitrano L, Brancaccio V, Guardascione MA, et al. Inherited coagulation disorders in cirrhotic patients with portal vein thrombosis. Hepatology 2000; 31: 345-8.
34. Wanless IR, Wong F, Blendis LM, Greig P, Heathcote EJ, Levy G. Hepatic and portal vein thrombosis in cirrhosis: possible role in development of parenchymal extinction and portal hypertension. Hepatology1995; 21: 1238-1247.
35. Fiorucci S, Antonelli E, Distrutti E, Severino B, Fiorentina R, Baldoni M, et al. PAR1 antagonism protects against experimental liver fibrosis. Role of proteinase receptors in stellate cell activation. Hepatology 2004; 39: 365-375.
36. Scotton CJ, Krupiczojc MA, Konigshoff M, Mercer PF, Lee YC, Kaminski N, et al. Increased local expression of coagulation factor X contributes to the fibrotic response in human and murine lung injury. J Clin Invest 2009; 119: 2550-2563.
37. Calvaruso V, Maimone S, Gatt A, Tuddenham E, Thursz M, Pinzani M, et al. Coagulation and fibrosis in chronic liver disease. Gut 2008; 57: 1722-1727.
38. Tsochatzis EA, Senzolo M, Germani G, Gatt A, Burroughs AK. Systematic review: portal vein thrombosis in cirrhosis. Aliment Pharmacol Ther 2010; 31: 366-374.
39. Maria Assunta Zocco, Enrico Di Stasio, Raimondo De Cristofaro, Marialuisa Novi, Maria Elena Ainora, Francesca Ponziani, Laura Riccardi, Stefano Lancellotti, et al. Thrombotic risk factors in patients with liver cirrhosis: Correlation with MELD scoring system and portal vein thrombosis development Journal of Hepatology 2009; 51: 682-689.
40. Zhang Donglei, Hao Jianyu, Yang Ning. Protein C and D-dimer are related to portal vein thrombosis in patients with liver cirrhosis. Journal of Gastroenterology and Hepatology 2010; 25: 116-121.
41. Lisman T, Porte RJ. Hepatic artery thrombosis after liver transplantation: more than just a surgical complication? Transplant Int 2009; 22: 162-164.
42. Kadayifci A, Tan V, Ursell PC,Merriman RB, Bass NM. Clinical and pathologic risk factors for atherosclerosis in cirrhosis: a comparison between NASH related cirrhosis and cirrhosis due to other aetiologies. J Hepatol 2008; 49: 595-599.
43. Sogaard KK, Horvath-Puho E, Gronbaek H, Jepsen P, Vilstrup H, Sorensen HT. Risk of venous thromboembolism in patients with liver disease: a nationwide population-based case-control study. Am J Gastroenterol 2009; 104: 96-101.
44. David Gulley, Evgenia Teal, Attaya Suvannasankha Naga Chalasani, Suthat Liangpunsakul. Deep Vein Thrombosis and Pulmonary Embolism in Cirrhosis Patients. Dig Dis Sci 2008; 53: 3012-3017.
45. Patrick G Northup, Matthew M. McMahon, Parker Ruhl, Scott E. Altschuler, Agata Volk-Bednarz, Stephen H Caldwell, Carl L Berg. Coagulopathy does not Fully Protect Hospitalized Cirrhosis Patients from Peripheral Venous Thromboembolism. Am J Gastroenterol 2006; 101: 1524-1528.
46. Senzolo M, Sartori MT, Lisman T. Should we give thromboprophylaxis to patients with liver cirrhosis and coagulopathy? HPB (Oxford) 2009; 11: 459-464.
47. Charles W. Francis, M.D. Prophylaxis for Thromboembolism in Hospitalized Medical Patients. N Engl J Med 2007; 356: 1438-44.
48. Jack Hirsh, Gordon Guyatt, Gregory W. Albers, Robert Harrington, Holger J Schünemann. American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133: 71S-105S.
49. Andrés Cárdenas, Pere Gines. Management of patients with cirrhosis awaiting liver transplantation. Gut 2011; 60: 412e421.
50. Laurie D DeLeve, Dominique Charles Valla, Guadalupe Garcia Tsao. Vascular Disorders of the Liver. Hepatology 2009.
1. Ousama Dabbagh, Aabha Oza, Sumi Prakash, Ramez Sunna, Timothy M Saettele. Coagulopathy does not protect against Venous Thromboembolism in Hospitalized Patients with Chronic Liver Disease. Chest 2010; 137(5): 1145-1149. [ Links ]
2. Ton Lisman, Stephen H Caldwell, Andrew K Burroughs, Patrick G Northup, Marco Senzolo R, Todd Stravitz, Armando Tripodi, James F Trotter, Dominique-Charles Valla, Robert J Porte. Hemostasis and thrombosis in patients with liver disease: The ups and downs. Journal of Hepatology 2010; 53: 362-371. [ Links ]
3. Armando Tripodi. The coagulopathy of chronic liver disease: Is there a causal relationship with bleeding? No. European Journal of Internal Medicine 2010; 21: 65-69. [ Links ]
4. Stefania Basili, Valeria Raparelli, Francesco Violi. The coagulopathy of chronic liver disease: Is there a causal relationship with bleeding? Yes. European Journal of Internal Medicine 2010; 21: 62-64. [ Links ]
5. Reverter JC. Abnormal hemostasis tests and bleeding in chronic liver disease: are they related? Yes. J Thromb Haemost 2006; 4: 717-20. [ Links ]
6. Senzolo M, Burra P, Cholongitas E, Burroughs AK. New insights into the coagulopathy of liver disease and liver transplantation. World J Gastroenterol 2006; 12: 7725-36. [ Links ]
7. Giuseppe Lippi, Giovanni Targher, Emmanuel J. Favaloro, Massimo Franchini. Venous Thromboembolism in Chronic Liver Disease. Seminars in Thrombosis and Hemostasis 2011; 37(1). [ Links ]
8. Armando Tripodi, Pier Mannuccio Mannucci. The Coagulopathy of Chronic Liver Disease. N Engl Med 2011; 365: 147-56. [ Links ]
9. Bosch J, Reverter JC. The coagulopathy of cirrhosis: myth or reality? Hepatology 2005; 41: 434-5. [ Links ]
10. Sohail Ahmed Siddiqui, Mubashir Ahmed, Muhammad Hanif Ghani, Muhammad Anwar Memon, Ghulam Mustafa, Muhammad Aslam Ghori. Coagulation abnormalities in patients with chronic liver disease in Pakistan. JPMA 2011; 61: 363. [ Links ]
11. Violi F, Leo R, Basili S, Ferro D, Cordova C, Balsano F. Association between prolonged bleeding time and gastrointestinal hemorrhage in 102 patients with liver cirrhosis: results of a retrospective study. Haematologica 1994; 79: 61-65. [ Links ]
12. Violi F, Ferro D, Basili S, Quintarelli C, Saliola M, Alessandri C, et al. Hyperfibrinolysis increases the risk of gastrointestinal hemorrhage in patients with advanced cirrhosis. Hepatology 1992; 15: 672-676. [ Links ]
13. Tacke F, Fiedler K, Trautwein C. A simple clinical score predicts high risk for upper gastrointestinal hemorrhages from varices in patients with chronic liver disease. Scand J Gastroenterol 2007; 42: 374-382. [ Links ]
14. Basili S, Ferro D, Leo R, Juliano L, Alessandri C, Cordova C, et al. Bleeding time does not predict gastrointestinal bleeding in patients with cirrhosis. The CALC Group. Coagulation Abnormalities in Liver Cirrhosis. J Hepatol 1996; 24: 574-80. [ Links ]
15. Armando Tripodi, Massimo Primignani, Veena Chantarangkul, Alessandra Dellera, Marigrazia Clerici, Roberto De Franchis, Massimo Colombo, Pier Mannuccio Mannucci. An Imbalance of Pro- vs. Anti-Coagulation Factors in Plasma from Patients with Cirrhosis. Gastroenterology 2009; 137: 2105-2111. [ Links ]
16. Alexander Hodge, Philip Crispin. Coagulopathy in liver disease: The whole is greater than the sum of its parts. J. Gastroenterol. Hepatol 2010; 25: 116-121. [ Links ]
17. Sharara AI, Rockey DC. Gastroesophageal variceal hemorrhage. N Engl J Med 2001; 345: 669-681. [ Links ]
18. Montalto P, Vlachogiannakos J, Cox DJ, Pastacaldi S, Patch D, Burroughs AK. Bacterial infection in cirrhosis impairs coagulation by a heparin effect: a prospective study. J Hepatol 2002; 37: 463-470. [ Links ]
19. Senzolo M, Coppell J, Cholongitas E, Riddell A, Triantos CK, Perry D, et al. The effects of glycosaminoglycans on coagulation: a thromboelastographic study. Blood Coagul Fibrinolysis 2007; 18: 227-236. [ Links ]
20. Armando Tripodi, Francesco Salerno, Veena Chantarangkul, Marigrazia Clerici, Massimo Cazzaniga, Massimo Primignani, Pier Mannuccio Mannucci. Evidence of Normal Thrombin Generation in Cirrhosis despite Abnormal Conventional Coagulation Tests. Hepatology 2005; 41: 553-558. [ Links ]
21. Armando Tripodi, Massimo Primignani, Veena Chantarangkul, Marigrazia Clerici, Alessandra DellEra, Federica Fabris, Francesco Salerno, Pier Mannuccio Mannucci. Thrombin Generation in Patients with Cirrhosis: The Role of Platelets. Hepatology 2006; 44: 440-445. [ Links ]
22. Segal JB, Dzik WH. Paucity of studies to support that abnormal coagulation test results predict bleeding in the setting of invasive procedures: an evidence-based review. Transfusion 2005; 45: 1413-1425. [ Links ]
23. Bernstein DE, Jeffers L, Erhardtsen E, Reddy KR, Glazer S, Squiban P, et al. Recombinant factor VIIa corrects prothrombin time in cirrhotic patients: a preliminary study. Gastroenterology 1997; 113: 1930-1937. [ Links ]
24. Lodge JP, Jonas S, Oussoultzoglou E, Malago M, Jayr C, Cherqui D, et al. Recombinant coagulation factor VIIa in major liver resection: a randomized, placebo-controlled, double-blind clinical trial. Anesthesiology 2005; 102: 269-275. [ Links ]
25. Lodge JP, Jonas S, Jones RM, Olausson M, Mir-Pallardo J, Soefelt S, et al. Efficacy and safety of repeated perioperative doses of recombinant factor VIIa in liver transplantation. Liver Transplant 2005; 11: 973-979. [ Links ]
26. Planinsic RM, van der MJ, Testa G, Grande L, Candela A, Porte RJ, et al. Safety and efficacy of a single bolus administration of recombinant factor VIIa in liver transplantation due to chronic liver disease. Liver Transplant 2005; 11: 895-900. [ Links ]
27. Bosch J, Thabut D, Albillos A, Carbonell N, Spicak J, Massard J, et al. Recombinant factor VIIa for variceal bleeding in patients with advanced cirrhosis: a randomized, controlled trial. Hepatology 2008; 47: 1604-1614. [ Links ]
28. OConnell KA, Wood JJ, Wise RP, Lozier JN, Braun MM. Thromboembolic adverse events after use of recombinant human coagulation factor VIIa. JAMA 2006; 295: 293-298. [ Links ]
29. Boylan JF, Klinck JR, Sandler AN, Arellano R, Greig PD, Nierenberg H, et al. Tranexamic acid reduces blood loss, transfusion requirements, and coagulation factor use in primary orthotopic liver transplantation. Anesthesiology 1996; 85: 1043-1048. [ Links ]
30. Agnelli G, Parise P, Levi M, Cosmi B, Nenci GG. Effects of desmopressin on hemostasis in patients with liver cirrhosis. Haemostasis 1995; 25: 241-247. [ Links ]
31. Valla DC. Thrombosis and anticoagulation in liver disease. Hepatology 2008; 47: 1384-93. [ Links ]
32. Okuda K, Ohnishi K, Kimura K, et al. Incidence of portal vein thrombosis in liver cirrhosis. An angiographic study in 708 patients. Gastroenterology 1985; 89: 279-86. [ Links ]
33. Amitrano L, Brancaccio V, Guardascione MA, et al. Inherited coagulation disorders in cirrhotic patients with portal vein thrombosis. Hepatology 2000; 31: 345-8. [ Links ]
34. Wanless IR, Wong F, Blendis LM, Greig P, Heathcote EJ, Levy G. Hepatic and portal vein thrombosis in cirrhosis: possible role in development of parenchymal extinction and portal hypertension. Hepatology1995; 21: 1238-1247. [ Links ]
35. Fiorucci S, Antonelli E, Distrutti E, Severino B, Fiorentina R, Baldoni M, et al. PAR1 antagonism protects against experimental liver fibrosis. Role of proteinase receptors in stellate cell activation. Hepatology 2004; 39: 365-375. [ Links ]
36. Scotton CJ, Krupiczojc MA, Konigshoff M, Mercer PF, Lee YC, Kaminski N, et al. Increased local expression of coagulation factor X contributes to the fibrotic response in human and murine lung injury. J Clin Invest 2009; 119: 2550-2563. [ Links ]
37. Calvaruso V, Maimone S, Gatt A, Tuddenham E, Thursz M, Pinzani M, et al. Coagulation and fibrosis in chronic liver disease. Gut 2008; 57: 1722-1727. [ Links ]
38. Tsochatzis EA, Senzolo M, Germani G, Gatt A, Burroughs AK. Systematic review: portal vein thrombosis in cirrhosis. Aliment Pharmacol Ther 2010; 31: 366-374. [ Links ]
39. Maria Assunta Zocco, Enrico Di Stasio, Raimondo De Cristofaro, Marialuisa Novi, Maria Elena Ainora, Francesca Ponziani, Laura Riccardi, Stefano Lancellotti, et al. Thrombotic risk factors in patients with liver cirrhosis: Correlation with MELD scoring system and portal vein thrombosis development Journal of Hepatology 2009; 51: 682-689. [ Links ]
40. Zhang Donglei, Hao Jianyu, Yang Ning. Protein C and D-dimer are related to portal vein thrombosis in patients with liver cirrhosis. Journal of Gastroenterology and Hepatology 2010; 25: 116-121. [ Links ]
41. Lisman T, Porte RJ. Hepatic artery thrombosis after liver transplantation: more than just a surgical complication? Transplant Int 2009; 22: 162-164. [ Links ]
42. Kadayifci A, Tan V, Ursell PC,Merriman RB, Bass NM. Clinical and pathologic risk factors for atherosclerosis in cirrhosis: a comparison between NASH related cirrhosis and cirrhosis due to other aetiologies. J Hepatol 2008; 49: 595-599. [ Links ]
43. Sogaard KK, Horvath-Puho E, Gronbaek H, Jepsen P, Vilstrup H, Sorensen HT. Risk of venous thromboembolism in patients with liver disease: a nationwide population-based case-control study. Am J Gastroenterol 2009; 104: 96-101. [ Links ]
44. David Gulley, Evgenia Teal, Attaya Suvannasankha Naga Chalasani, Suthat Liangpunsakul. Deep Vein Thrombosis and Pulmonary Embolism in Cirrhosis Patients. Dig Dis Sci 2008; 53: 3012-3017. [ Links ]
45. Patrick G Northup, Matthew M. McMahon, Parker Ruhl, Scott E. Altschuler, Agata Volk-Bednarz, Stephen H Caldwell, Carl L Berg. Coagulopathy does not Fully Protect Hospitalized Cirrhosis Patients from Peripheral Venous Thromboembolism. Am J Gastroenterol 2006; 101: 1524-1528. [ Links ]
46. Senzolo M, Sartori MT, Lisman T. Should we give thromboprophylaxis to patients with liver cirrhosis and coagulopathy? HPB (Oxford) 2009; 11: 459-464. [ Links ]
47. Charles W. Francis, M.D. Prophylaxis for Thromboembolism in Hospitalized Medical Patients. N Engl J Med 2007; 356: 1438-44. [ Links ]
48. Jack Hirsh, Gordon Guyatt, Gregory W. Albers, Robert Harrington, Holger J Schünemann. American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133: 71S-105S. [ Links ]
49. Andrés Cárdenas, Pere Gines. Management of patients with cirrhosis awaiting liver transplantation. Gut 2011; 60: 412e421. [ Links ]
50. Laurie D DeLeve, Dominique Charles Valla, Guadalupe Garcia Tsao. Vascular Disorders of the Liver. Hepatology 2009. [ Links ]

