











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Neuroendocrine neoplasms (NENs), previously known as carcinoid tumors, originate from the neuroendocrine cells found in the skin, lungs, gonads, pancreas, and gastrointestinal tract1. They are rare, with an estimated annual incidence of 1.05 cases per 100,000 inhabitants. Although considered a rare disease, the incidence has increased eightfold over the past five decades2. The exact causes of the appearance of these tumors are not known3.
Primary NENs are most frequently located in the gastrointestinal tract (62%-67%) with greater involvement of the small intestine (45%), rectum (20%), appendix (16%), colon (11%), pancreas (5%-10%) and stomach (7%)4. NENs arising from the small bowel (SB-NEN) are considered rare malignant neoplasms, which are further classified as well-differentiated neuroendocrine tumors (NETs) and poorly differentiated neuroendocrine carcinomas (NECs), according to the 2022 World Health Organization (WHO) classification5.
This case presents a NET in the distal ileum in a patient with nonspecific symptoms, diagnosed during a colonoscopy with ileocecal intubation.
Clinical case
This is a 56-year-old female patient with a history of difficult-to-manage hypertension (HTN) since 2022. In the search for the origin of the HTN, she underwent various studies: a normal total abdominal ultrasound, an abdominal and pelvic MRI with contrast, which revealed pancreatic cysts, and an endoscopic ultrasound with biopsy, which provided a histological diagnosis of mucinous pancreatic cysts. She was referred to gastroenterology due to diffuse colicky abdominal pain associated with bloating and two soft stools per day, which had been present for two years. A colonoscopy with ileal intubation was performed, revealing a 15 mm sessile polypoid elevated lesion in the distal ileum, 5 cm from the ileocecal valve (Figure 1). The pathology report from the lesion biopsies showed the presence of a well-differentiated, low-grade NET (Grade I), with a mitotic count of 0-1 per mm2, CKAE1/AE3: positive, focal, extranodal extension, and strong positivity for synaptophysin, chromogranin, and enolase (Figure 2).

Figure 1 Ileocolonoscopy. Sessile polypoid lesion (Paris classification: 0-Is) in the distal ileum. A. Image with white light. B. Image with digital chromoendoscopy. Images property of the authors.
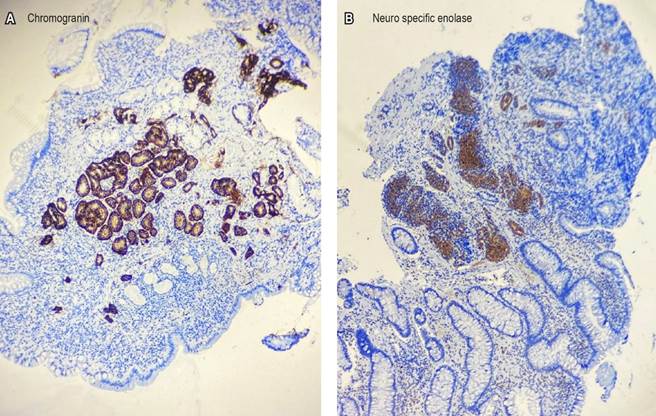
Figure 2 Biopsy of the ileal sessile polypoid lesion. A. Positive chromogranin. B. Positive enolase. Images property of the authors.
An endoscopic capsule was ordered to rule out other lesions in the small intestine, which confirmed the lesion in the distal ileum, with no other significant findings (Figure 3).
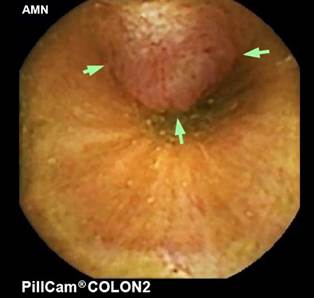
Figure 3 Endoscopic capsule. Sessile polypoid lesion (Paris classification: 0-Is) in the distal ileum. The image is the property of the authors.
The patient underwent other paraclinical tests: hemoglobin: 12 g/dL, platelets: 424,000, glycemia: 90 mg/dL, creatinine: 0.68 mg/dL, alkaline phosphatase: 92 U/L, γ-glutamyl transferase (GGT): 56 U/L, alanine aminotransferase (ALT): 31 U/L, aspartate aminotransferase (AST): 20 U/L, total bilirubin: 1.10 mg/dL, direct bilirubin: 0.29 mg/dL, indirect bilirubin: 0.72 mg/dL, albumin: 4.8 g/dL, lactate dehydrogenase (LDH): 168 U/L, insulin: 7 mU/L , 5-hydroxyindoleacetic acid: 6.8 mg/24 hours, chromogranin A: 7.8 ng/mL, fecal calprotectin: 80 μg/g.
She was evaluated by oncological surgery, where an octreotide scan was ordered. This imaging showed the endoluminal lesion in the distal ileum with somatostatin receptor overexpression and an ileocolic right lymphadenopathy (Figure 4). A chest CT scan showed no evidence of metastasis. The patient underwent laparoscopic surgery, which included a right hemicolectomy with retroperitoneal lymphadenectomy.

Figure 4 Octreotide scan shows focal nodular uptake in the right flank. The image is the property of the authors.
The final histopathological diagnosis was a grade 2 ileal NET, measuring 1.5 x 1 cm in diameter, with extension into the muscularis propria without lymphovascular or perineural invasion, and tumor-free resection margins. A total of 3 of the 22 resected lymph nodes showed tumor involvement, with extranodal extension present at 1 mm and metastasis size measuring 6 mm. Immunohistochemistry of the surgical specimen revealed positive synaptophysin, positive chromogranin, CD56+, Ki-67: 4%-5%, and a mitotic index of 3 mitoses per 10 high-power fields. The patient has not required adjuvant treatment during follow-up to date and has had good clinical progression, with improvement in abdominal pain and better control of HTN.
Discussion
The first description of a small bowel NET was made by Lanchas in 1867, who described a polypoid tumor in the small intestine. In 1890, Ransom described the symptoms of diarrhea and dyspnea in a patient with a lesion in the ileum and hepatic metastases, which would later be known as carcinoid syndrome6. NETs are classified according to their signs and symptoms into non-functional and functional types. On the one hand, non-functional NETs present with signs and symptoms related to the tumor’s location, such as abdominal pain or obstruction. Functional NETs, on the other hand, have symptoms associated with the secretion of amines and peptides, particularly serotonin, as seen in “carcinoid syndrome,” which presents with facial flushing, a sensation of heat in the face and neck, chronic diarrhea, and dyspnea. However, functional NETs may present with other symptoms depending on the hormone secreted, such as in cases of gastric overproduction leading to Zollinger-Ellison syndrome, or the secretion of adrenocorticotropic hormone (ACTH), which causes Cushing’s syndrome6. In our case, the patient presented with a non-functional NET and nonspecific symptoms, such as abdominal pain.
The WHO classifies NETs based on their histopathology into three grades: Grade 1: low grade, well-differentiated with a mitotic count of <2 per 10 HPF or Ki-67 index <3%; Grade 2: intermediate grade, well-differentiated with a mitotic count of 2-20 per 10 HPF or Ki-67 index 3%-20%; and Grade 3: high grade, poorly differentiated with a mitotic count of >20 per 10 HPF or Ki-67 index >20%. NECs are characterized by poor differentiation and a mitotic count >20 per 10 HPF or Ki-67 index >20%7. According to the tumor’s extent, it is classified into stages based on the TNM system (Table 1).
Table 1 American Joint Committee on Cancer (AJCC) TNM classification and survival rates of ileal NEN
| Stage | TNM | Description | 5-year survival rate |
|---|---|---|---|
| Stage 1 | T1, N0, M0 | T1 = invades lamina propria or submucosa and measures ≤1 cm. | 87.37% |
| Stage 2 |
|
. |
84.16% |
| Stage 3 |
|
|
90.62% |
| Stage 4 |
|
. |
76.67% |
Adapted from: Chauhan A, et al. CA Cancer J Clin. 2024;74(4):359-672.
Patients in stage 3 paradoxically had better survival rates than those in stages 1 and 2. However, this lack of a hierarchical prognosis by stage may be due to insufficient lymph node dissection, which can lead to poor staging. Furthermore, survival analyses of patients with these tumors are limited because the data include cases diagnosed between 2010 and 2016, during the seventh edition of the American Joint Committee on Cancer (AJCC) staging system. With significant changes in the eighth and ninth editions, such as the inclusion of the pathological category (pN2), it is expected that this prognostic stratification will improve2.
NETs can be sporadic or associated with genetic syndromes, such as multiple endocrine neoplasia (MEN1, MEN2A, MEN2B), von Hippel-Lindau disease, or neurofibromatosis type 17. The majority of SB-NENs are asymptomatic, and 80% to 90% present with hepatic metastases at the time of diagnosis. Among these, 20% will develop carcinoid syndrome8. Diagnostic aids for detecting SB-NEN include multi-phase contrast-enhanced computed tomography (CT), contrast-enhanced magnetic resonance imaging (MRI), and somatostatin receptor studies, such as somatostatin receptor scintigraphy, positron emission tomography-computed tomography (PET/CT), or positron emission tomography-magnetic resonance imaging (PET/MRI), with the latter providing higher diagnostic performance. In cases of suspected SB-NET, ileocolonoscopy, deep enteroscopy, and capsule endoscopy are useful for diagnosis, staging, and detecting synchronous lesions5,9.
In patients with functional NETs, biochemical tests are performed to identify the causal substance of the symptoms: serum or 24-hour urinary 5-hydroxyindoleacetic acid (5-HIAA), plasma chromogranin A (CgA), and tests for Cushing’s syndrome10. However, CgA should not be used for detection purposes, as elevated levels are found in patients with chronic kidney disease, atrophic gastritis, and inflammatory bowel disease. It is, however, useful for monitoring5.
The treatment for non-metastatic SB-NETs consists of open intestinal resection with regional lymphadenectomy of at least eight lymph nodes, along with bimanual palpation of the entire small intestine to rule out synchronous lesions. In patients with unresectable metastatic disease, a conservative approach is preferred, including imaging follow-up, treatment with somatostatin analogs (octreotide), and surgical intervention in cases of intestinal obstruction4,10,11. For SB-NETs that do not respond to first-line therapy, second-line treatments such as everolimus or peptide receptor radionuclide therapy with lutetium Lu 177-dotatate (177Lu) are available10. Treatment algorithms are presented in Figures 5 and 6.
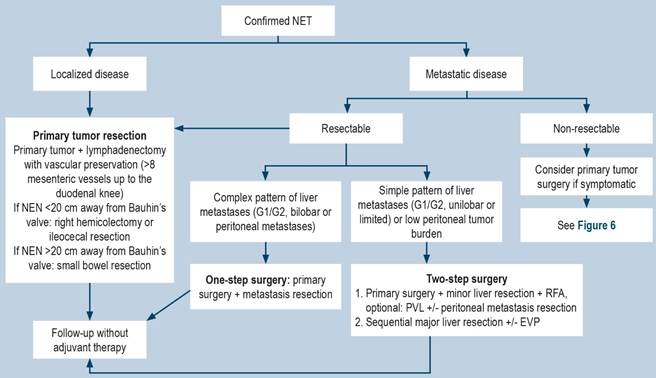
Figure 5 Treatment algorithm for SB-NETs. PVE: portal vein embolization; PVL: portal vein ligation; RFA: radiofrequency ablation. Adapted from: Oronsky B, et al. Neoplasia. 2017;19(12):991-10024.
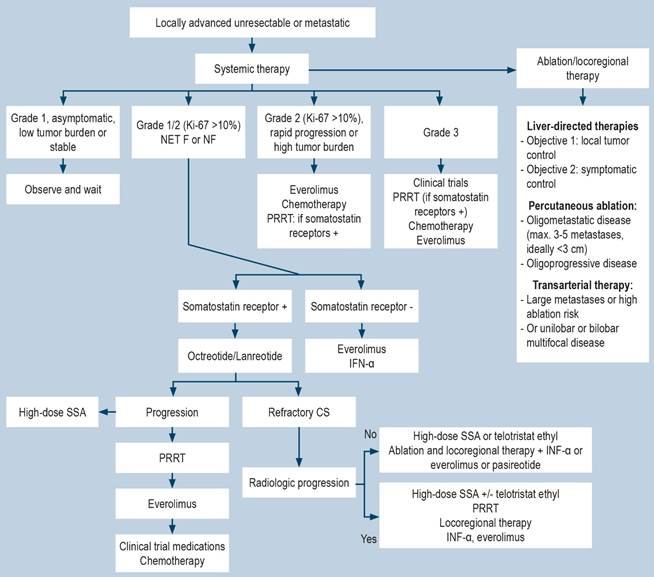
Figure 6 Treatment algorithm for SB-NETs. CS: carcinoid syndrome; PRRT: peptide receptor radionuclide therapy; SSA, somatostatin analogues. Adapted from: Oronsky B, et al. Neoplasia. 2017;19(12):991-10024.
For patients treated with surgery and complete tumor resection (curative surgery), follow-up for grade 1 and 2 tumors should be performed every 6 to 12 months, while for grade 3 tumors, it should be done every 6 months. In cases of unresectable metastatic SB-NETs, follow-up should be every 3 to 6 months for grade 1 and 2 tumors, and every 3 months for grade 3 tumors. During follow-up, measurements of CgA, 5-HIAA, three-phase CT scan, or somatostatin receptor-based imaging studies are required if recurrence or metastasis is suspected11.
In the present clinical case, a grade 2 neuroendocrine neoplasm was diagnosed incidentally in a patient with nonspecific gastrointestinal symptoms (abdominal pain). This highlights the importance of routine colonoscopy with ileocecal intubation in the early detection of lesions, which allows for timely therapy and positively impacts patient prognosis.

