











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Video capsule endoscopy (VCE) has transformed gastroenterology practice by providing a minimally invasive method for evaluating the small bowel. Since its introduction in 2000, this technology has demonstrated high diagnostic yield in clinical scenarios such as obscure gastrointestinal bleeding, inflammatory bowel disease (IBD), celiac disease, polyposis syndromes, and other small bowel and colonic disorders. It offers important advantages over conventional techniques, as it does not require sedation, is well tolerated, and is associated with low complication rates1-3.
Technological advances in capsule endoscopy systems have improved image quality, recording time, lesion detection, and patient acceptability. Among the most widely used devices are the PillCam SB3 and PillCam Colon systems, both extensively validated in international studies. More recent technologies, such as the CapsoCam SV-1, which provides a 360° panoramic view, offer additional diagnostic opportunities. However, clinical experience remains limited and is still evolving4-7.
In the Latin American context, and particularly in Colombia, published studies evaluating the clinical utility of VCE are scarce and have focused primarily on outpatient populations8,9. Evidence regarding its implementation in hospitalized patients is even more limited, despite the greater clinical complexity of this population, characterized by comorbidities, reduced mobility, and a potentially different risk profile. Robust evidence in this setting is essential to optimize timely diagnostic and therapeutic decision-making, particularly for common indications such as obscure gastrointestinal bleeding and IBD.
In this context, a multicenter experience in Colombia using capsule endoscopy in hospitalized patients is presented. The study employed PillCam SB3, PillCam Colon, and CapsoCam SV-1 technologies. It represents the first national series describing diagnostic yield, bowel preparation quality, and safety profile in this patient population and provides locally relevant clinical evidence to support improved management in this setting.
Materials and methods
Study design and data extraction
A descriptive observational cross-sectional study was conducted using convenience sampling between November 2019 and December 2021 in two referral centers for gastroenterology and digestive endoscopy in Bogotá, Colombia. The study population included patients aged ≥18 years with an indication for capsule endoscopy (CE) for any reason, according to the treating physician’s clinical judgment, and with initial negative endoscopic studies for a bleeding source in both the upper and lower gastrointestinal tract (including ileoscopy with evaluation of the distal 15 cm of the ileum). Eligible patients had no obstructive symptoms or known intestinal stenosis and were hospitalized in general inpatient wards. Patients who had used nonsteroidal anti-inflammatory drugs (NSAIDs) within two months prior to the endoscopic procedure were excluded. Additional exclusion criteria included absence of ileocolonoscopy and the presence of obstructive symptoms, such as abdominal distension, nausea, vomiting, or recurrent episodes of intestinal obstruction.
Data collection
Medical records and official procedure reports were used as primary sources of information. Sociodemographic and clinical variables were collected, and a descriptive analysis was conducted to assess diagnostic effectiveness, endoscopic findings, bowel preparation quality, and adverse events. Collected variables included age, sex, clinical indication, endoscopic findings, findings suggestive of small bowel Crohn’s disease (CD), and clinical and technical complications.
Definitions
The quality of bowel preparation for capsule endoscopy was assessed using the small bowel cleansing scale described by Hooks et al.10, based on overall evaluability. This scale incorporates qualitative and quantitative criteria, ease of assessment, reduced time requirements, and endoscopist preference. In this classification, excellent preparation is defined as the presence of small fragments of adherent solid material with clear or lightly colored fluid; good preparation as the presence of small amounts of liquid, minimal solid material, or dark fluid that does not interfere with the examination; fair preparation as the presence of sufficient solid material or dark fluid to impair reliable examination; and poor preparation as the presence of a large volume of food residue or fecal material that precludes complete examination. Findings suggestive of small bowel CD were defined according to criteria established by the Japanese Society, specifically the presence of at least one major criterion proposed by Matsui et al.11 and validated by Hisabe et al.12. These criteria included longitudinal ulcers, cobblestone appearance, or non-caseating epithelioid cell granulomas. In the colon, findings suggestive of ulcerative colitis (UC) included mucosal edema, loss of vascular pattern, erythema, mucosal granularity and friability, erosions, ulcers, and pseudopolyps. Findings suggestive of Crohn’s disease included aphthous ulcers, cobblestone pattern, and discontinuous (“skip”) lesions13.
Statistical analysis
Data were processed using SPSS version 25 (IBM Corp., Armonk, NY). Categorical variables were expressed as absolute and relative frequencies (%). Continuous variables were summarized using means and standard deviations (SD) or medians and ranges, according to data distribution. Comparisons among groups (PillCam SB3, PillCam Colon, and CapsoCam SV-1) were performed using the chi-square test or Fisher’s exact test for categorical variables, and ANOVA or Kruskal-Wallis tests for continuous variables. Ninety-five percent confidence intervals (95% CI) were calculated, and statistical significance was defined as p < 0.05.
Ethical considerations
The study was approved by the Ethics Committee of Gastroadvanced IPS, which provides gastroenterology services at two tertiary-level institutions and serves as a local referral center for gastroenterology and digestive endoscopy. The study design adhered to the principles of the Declaration of Helsinki (2013 revision, Fortaleza, Brazil) and Resolution 8430 of 1993 issued by the Colombian Ministry of Health. The study was classified as minimal risk research. Confidentiality and data protection were strictly ensured. All patients were informed and provided written informed consent. No records contained sensitive patient-identifying information.
Procedure
All patients received the same bowel preparation protocol. Two days before the procedure, patients were advised to consume a soft diet and clear liquids without artificial coloring. On the day prior to the study, patients followed a clear liquid diet and initiated fasting at 17:00 hours, followed by oral administration of 3 L of polyethylene glycol solution (NULYTELY®; formulation containing more than 105 g of polyethylene glycol 3350, 2.8 g NaCl, 0.37 g KCl, and 1.43 g NaHCO₃), according to institutional availability. No additional laxative boosters were used.
The technologies employed included PillCam SB3, PillCam Colon, and CapsoCam SV-1 (CapsoVision), available at the time of the study. The sole objective was evaluation of the small intestine. The PillCam SB3 and PillCam Colon systems are cylindrical devices with adaptive image capture rates. PillCam SB3 is designed for small bowel endoscopy and operates at an adjustable frame rate ranging from 2 to 6 frames per second, allowing acquisition of high-quality images during transit through the small intestine. PillCam Colon, primarily designed for colon evaluation, uses an adaptive frame rate typically ranging between 4 and 6 frames per second to ensure adequate coverage of the intestinal tract, although its principal function focuses on imaging the colonic mucosa. Both devices are equipped with a camera, light source, batteries, and transmitter, and can capture up to 60,000 images during gastrointestinal transit. Images are transmitted to an external recording device, after which they are downloaded and analyzed by two gastroenterologists experienced in VCE interpretation.
The CapsoCam SV-1 system provides a 360° panoramic view of the small intestine. This capsule uses wireless technology and is equipped with four high-speed cameras that enable detailed visualization of the intestinal mucosa. During the first two hours of examination, the capsule captures images at 20 frames per second (fps), after which the capture rate decreases to 12 fps while maintaining adequate coverage for complete evaluation of the gastrointestinal tract. The CapsoCam SV-1 has a battery life of up to 15 hours, sufficient for most small bowel examinations. Images are stored directly in the capsule’s internal memory; therefore, the patient does not need to carry an external receiver. After completion of the examination, the capsule is naturally excreted, and stored images are downloaded for analysis using specialized software. The software allows simultaneous visualization of up to four images and achieves a total viewing rate of approximately 32 frames per second (eight frames per second per image). The study was independently evaluated by two expert endoscopists, who recorded findings for each patient and issued a written report14-17.
For analysis, a retrospective database was created including the following variables: patient name, sex, age, study results, and technical and clinical complications identified.
Results
Clinical characteristics
A total of 68 hospitalized patients were included, of whom 61.8% were male (n = 42; 95% CI: 49.6-73.0). The median age was 60.5 years (range: 18-96; SD: 24.3), with no significant differences by sex (p = 0.27). Bowel preparation quality was optimal in 92.6% of cases (75.0% excellent; 17.6% adequate), whereas only 7.4% were classified as fair, supporting high diagnostic reliability. Regarding clinical indications, the most frequent was obscure gastrointestinal bleeding (77.9%; 95% CI: 65.8-86.9), followed by suspected inflammatory bowel disease (IBD) (22.1%; 95% CI: 13.1-34.2). In terms of technology used, CapsoCam SV-1 was employed in 54.4% of cases (n = 37), PillCam SB3 in 25.0% (n = 17), and PillCam Colon in 20.6% (n = 14), reflecting device availability and clinical preference at participating centers. Detailed clinical and technical characteristics of the cohort are presented in Table 1, including proportions, measures of central tendency, and corresponding 95% confidence intervals.
Table 1 Clinical and technical characteristics of patients undergoing inpatient capsule endoscopy (n = 68)
| Variable | n (%) | 95% CI |
|---|---|---|
| Male sex | 42 (61.8) | 49.6-73.0 |
| Age, years (mean ± SD; range) | 60.5 ± 24.3 (18-96) | - |
| Previous studies | ||
| Ileocolonoscopy | 68 (100) | - |
| Contrast-enhanced abdominal CT | 34 (50.0) | 37.6-62.4 |
| Upper gastrointestinal endoscopy | 56 (82.4) | 71.2-90.3 |
| Technology used | ||
| PillCam SB3 | 17 (25.0) | 15.2-37.1 |
| PillCam Colon 2* | 14 (20.6) | 11.9-32.8 |
| CapsoCam SV-1 | 37 (54.4) | 41.9-66.4 |
| Main indication | ||
| Suspected obscure gastrointestinal bleeding | 53 (77.9) | 65.8-86.9 |
| Suspected inflammatory bowel disease | 15 (22.1) | 13.1-34.2 |
| Bowel preparation quality (modified Boston scale) | ||
| Excellent | 51 (75.0) | 62.9-84.7 |
| Adequate | 12 (17.6) | 9.7-28.8 |
| Fair | 5 (7.4) | 2.8-16.9 |
*For PillCam Colon 2, activation was performed in the stomach to avoid hibernation periods. SD: standard deviation; IBD: inflammatory bowel disease; 95% CI: 95% confidence interval. Table prepared by the authors.
Capsule endoscopy procedure
Capsule ingestion was successful in all patients. No failures were documented in device activation or image transmission to the recording systems. The mean time from ingestion to esophageal passage was 5.9 seconds (range: 3.7-8.1). Mean gastric transit time was 43.8 minutes (range: 26-74) and mean small bowel transit time was 384 minutes (range: 228-468). Regarding colonic progression, complete colonic imaging was obtained in 19 patients (27.9%; 95% CI: 18.2-40.0), with a mean colonic residence time of 110 minutes. Gastrointestinal transit parameters, compared across the three capsule systems used (PillCam SB3, PillCam Colon, and CapsoCam SV-1), are presented in detail in Table 2, including dispersion measures and 95% confidence intervals.
Table 2 Gastrointestinal transit times according to capsule endoscopy system used in hospitalized patients (n = 68)*
| Parameter | PillCam SB3 (n = 17) | PillCam Colon 2 (n = 14) | CapsoCam SV-1 (n = 37) | p-value |
|---|---|---|---|---|
| Esophageal transit (seconds), mean ± SD | 5.1 ± 1.2 | 5.2 ± 1.4 | 4.9 ± 1.1 | 0.74 |
| Gastric transit (minutes), mean ± SD | 40.3 ± 9.5 | 42.6 ± 10.1 | 41.5 ± 8.9 | 0.62 |
| Small bowel transit (minutes), mean ± SD | 279 ± 65 | 290 ± 71 | 217 ± 54 | 0.03** |
| Colonic residence time (minutes), mean ± SD | 109.4 ± 28.3 | 117.0 ± 30.1 | 112.9 ± 26.7 | 0.58 |
*Small bowel transit time was significantly shorter with CapsoCam SV-1 compared with PillCam systems (p = 0.03), whereas no significant differences were observed in other parameters. **p < 0.05 indicates statistical significance (one-way ANOVA). SD: standard deviation. Table prepared by the authors.
Clinical findings
Endoscopic findings obtained through capsule endoscopy are summarized in Tables 3 and 4. In studies performed with PillCam SB3 and PillCam Colon, the most frequent lesions were ulcers and erosions (67.8%), followed by angiectasias (19.5%). In all cases, prior ileocolonoscopy was negative for clinically relevant findings, highlighting the added diagnostic value of capsule endoscopy in this patient population.
Table 3 Endoscopic findings in patients evaluated with PillCam SB3 or PillCam Colon capsule endoscopy (n = 31)
| Finding | n (%) | 95% CI |
|---|---|---|
| Erosions or ulcers | 21 (67.8) | 48.6-82.8 |
| Small bowel angiectasias | 6 (19.5) | 8.0-37.0 |
| Phlebectasias | 2 (6.4) | 1.1-21.1 |
| Lymphangiectasias | 3 (9.6) | 2.6-25.9 |
| Ulcerated jejunal gastrointestinal stromal tumor (GIST) | 1 (3.2) | 0.2-19.0 |
Ulcers/erosions and vascular lesions represented more than 85% of diagnoses in this subgroup. IBD: inflammatory bowel disease; GIST: gastrointestinal stromal tumor; 95% CI: 95% confidence interval; SB: small bowel. Table prepared by the authors.
Table 4 Endoscopic findings in patients evaluated with CapsoCam SV-1 capsule endoscopy (n = 37)
| Overall findings | n (%) | 95% CI |
|---|---|---|
| Erosions or ulcers | 28 (75.7) | 59.9-87.1 |
| Small bowel angiectasias | 9 (24.3) | 12.5-41.0 |
| Phlebectasias | 4 (10.8) | 3.4-25.0 |
| Lymphangiectasias | 5 (13.5) | 5.0-28.9 |
| Findings attributable to IBD (n = 15) | n (%) | 95% CI |
| Ileal ulcer | 9 (60.0) | 35.8-80.2 |
| Jejunal ulcer | 5 (33.3) | 14.6-58.9 |
| Stenotic lesions | 1 (6.6) | 0.3-28.7 |
IBD: inflammatory bowel disease; 95% CI: 95% confidence interval; SB: small bowel. Table prepared by the authors.
Safety profile and adverse events
A single adverse event (1.5%) was recorded with the CapsoCam SV-1 system in a patient with serpiginous ulcers and areas of ileal stenosis, who presented delayed capsule progression with an incomplete study. Fluoroscopic follow-up documented capsule retention in the right iliac fossa on day 5 and spontaneous progression to the transverse colon on day 7. Expulsion occurred on day 8 without the need for therapeutic intervention. This case did not meet criteria for capsule retention, and no clinical complications were observed.
No adverse events were reported with the PillCam SB3 or PillCam Colon systems. This confirms an overall favorable safety profile in hospitalized patients.
Diagnostic yield of PillCam SB3 and PillCam Colon
All cases in which PillCam SB3 and PillCam Colon were used corresponded to indications for obscure gastrointestinal bleeding. Capsule endoscopy established the diagnosis in 27 of 31 patients (87.1%; 95% CI: 71.2-95.1). The most frequent etiologies were ulcers, angiectasias, and vascular lesions (Table 3). Figures 1 and 2 illustrate representative examples of findings detected with PillCam SB3 and PillCam Colon, including stigmata of recent bleeding, subepithelial lesions, and ulcerated gastrointestinal stromal tumors that had not been identified in prior conventional endoscopic studies.
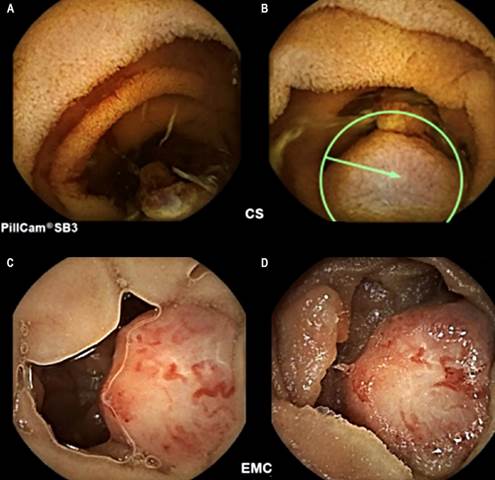
Figure 1 Images obtained using PillCam SB3 capsule endoscopy in patients with obscure gastrointestinal bleeding. A. Stigmata of recent bleeding. B. Non-ulcerated subepithelial lesion. C-D. Ulcerated gastrointestinal stromal tumor. Images property of the authors.
CapsoCam SV-1 capsule endoscopy findings
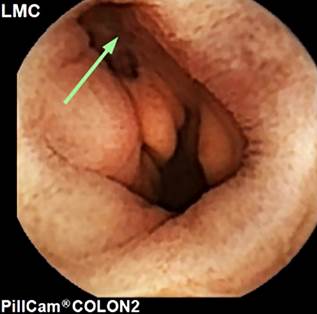
A total of 37 patients were evaluated using CapsoCam SV-1. Among them, 22 corresponded to indications for obscure gastrointestinal bleeding (59.5%), and 15 to suspected Crohn’s disease (40.5%). Capsule endoscopy established a diagnosis in 33 of 37 cases (89.2%; 95% CI: 74.6-96.9). This indicates a high diagnostic yield in the hospitalized patient population (Table 4, Figure 3). The most frequent lesions were deep ileal ulcers with irregular borders and fibrin deposition, predominantly located in the distal ileum. This pattern was observed primarily in younger patients, with a mean age <35 years, consistent with the age distribution described for more aggressive IBD phenotypes. In a single case (2.7%), stenosis with delayed capsule progression was documented, which resulted in an incomplete study. Imaging follow-up confirmed spontaneous device migration without the need for medical intervention, and the patient was subsequently diagnosed with stenosing Crohn’s disease. These findings support the clinical utility of CapsoCam SV-1 in the evaluation of the small bowel in the inpatient setting, both for the diagnosis of obscure gastrointestinal bleeding and for early detection of lesions consistent with inflammatory bowel disease.

Figure 3 Images obtained using CapsoCam SV-1 (CapsoVision) capsule endoscopy in patients with Crohn’s disease involving the small bowel. A-E. Ileal ulcer. F-G. Jejunal ulcers. H. Area of stenosis. Images property of the authors.
The most frequent findings were ulcers/erosions (75.7%), followed by vascular lesions (24.3%). In the subgroup with suspected IBD (n = 15), deep ileal ulcers were most commonly documented (60%), with one case of stenosis associated with delayed capsule excretion that did not require therapeutic intervention.
Discussion
This study demonstrates the clinical utility of capsule endoscopy using the PillCam SB3, PillCam Colon, and CapsoCam SV-1 systems in hospitalized patients in Colombia. The results show high diagnostic yield, adequate safety, and high-quality image acquisition in both obscure gastrointestinal bleeding and inflammatory bowel disease. A distinguishing feature of this study is that it represents the first national report describing the use of CapsoCam SV-1 in a hospitalized population, providing novel evidence in a clinical setting characterized by increased complexity and risk.
The findings indicate that capsule endoscopy is feasible and reliable in this patient population and achieves a diagnostic yield exceeding 75% for obscure gastrointestinal bleeding. This result is consistent with previous studies conducted in Latin America (60%-78%)18-21 and comparable to the Colombian registry reported by Galiano et al., which demonstrated an effectiveness of 91.7%8. These variations may be attributed to differences in technological availability, timing of the procedure, bowel preparation quality, and lesion interpretation, which remains operator-dependent. Internationally, variability in the diagnostic yield of capsule endoscopy for obscure gastrointestinal bleeding ranges from 38% to 93%22,23. This variability underscores the need to standardize interpretation criteria and establish the clinical relevance of detected lesions24,25.
Findings related to Crohn’s disease are of particular relevance. In this cohort, capsule endoscopy using CapsoCam SV-1 identified deep ileal ulcers and stenotic lesions, predominantly in younger patients, consistent with more aggressive disease phenotypes. Although Crohn’s disease is a heterogeneous condition requiring integration of clinical, endoscopic, radiologic, and histologic findings for diagnosis26, capsule endoscopy provides high-resolution imaging and facilitates early detection of inflammatory lesions. According to the STRIDE II strategy27,28, endoscopic remission is a key therapeutic target in Crohn’s disease management. The present findings support the role of capsule endoscopy as a complementary diagnostic tool to achieve treatment targets in the inpatient setting.
Regarding safety, a single case of delayed capsule excretion was documented with CapsoCam SV-1 in a patient with stenosing Crohn’s disease, without the need for medical intervention. This observation is consistent with international reports identifying capsule retention as the most clinically relevant complication, particularly in patients with inflammatory bowel disease29-31. Current literature supports the use of complementary diagnostic tools, such as patency capsules or CT enterography, to identify patients at risk of retention prior to capsule endoscopy31,32.
Bowel preparation remains a subject of ongoing debate. In this study, polyethylene glycol preparation achieved adequate or excellent quality in more than 90% of cases, consistent with national registry data9 and international studies such as that of Calabrese et al.26, which reported optimal preparation quality in more than 90% of patients with Crohn’s disease. These findings support the routine use of polyethylene glycol as a safe and cost-effective strategy in this clinical context.
Notably, the rate of complete visualization of the small bowel and colon exceeded 70%, which is an encouraging finding considering that the study population consisted of hospitalized patients with limited mobility and multiple comorbidities-factors that often impair capsule progression.
An additional finding of interest is the difference in Crohn’s disease clinical phenotype compared with Asian populations, where proximal involvement predominates and patients are typically younger (mean age 25 years)33-35. In the present series, involvement was primarily distal and observed in older patients (mean age >42 years). These differences suggest potential geographic and genetic variability in disease expression and highlight areas for future research in the region.
This study has limitations, including its retrospective design, relatively small sample size, and conduct in only two tertiary referral centers, which may limit generalizability. Unequal availability of capsule systems (PillCam and CapsoCam) may have introduced selection bias. Although interpretation of findings was performed by experienced endoscopists, a degree of subjectivity remains inherent. Nevertheless, independent data verification by two investigators minimized the risk of transcription errors.
Conclusions
This study demonstrates that capsule endoscopy is a safe and effective diagnostic tool in hospitalized patients in Colombia, with notable performance in the evaluation of obscure gastrointestinal bleeding and inflammatory small bowel disorders. The technique enables detection of clinically relevant lesions and supports timely therapeutic decision-making.
The PillCam SB3, PillCam Colon, and CapsoCam SV-1 systems demonstrated comparable performance in terms of image quality and diagnostic capability. This study represents the first national report describing the use of CapsoCam SV-1 in the inpatient setting. These findings suggest that capsule endoscopy, even in patients with greater clinical complexity, can be safely integrated into routine hospital practice.
Although the observed safety profile was overall favorable, prospective multicenter studies are needed to robustly compare available technologies, identify predictors of complications (such as capsule retention in patients with stenosis), and develop regional protocols adapted to the characteristics of the Latin American population.
Capsule endoscopy emerges as a high-value diagnostic strategy in the hospital setting. Its systematic implementation may optimize comprehensive management of patients with small bowel disorders in this context.

