











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
The gut-brain axis constitutes a bidirectional communication network between the central nervous system and the gastrointestinal system. This network regulates not only digestive physiological functions but also emotional responses to psychological stressors1,2. Disorders of gut-brain interaction (DGBI) are gastrointestinal disorders associated with a combination of altered motility, visceral hypersensitivity, mucosal and immune dysfunction, alterations in the intestinal microbiota, and changes in central nervous system processing3. These disorders include symptoms such as abdominal pain, bloating, and changes in bowel habits, and are highly prevalent in gastroenterology practice4,5; their classification is based on the assessment of chronic gastrointestinal symptoms occurring in the absence of structural or organic abnormalities that could explain them6. The most extensively studied and clinically relevant DGBI include irritable bowel syndrome (IBS), functional dyspepsia (FD), functional constipation (FC), functional diarrhea, and functional abdominal bloating/distension3. A study conducted in Argentina, Brazil, Colombia, and Mexico reported that DGBI are highly prevalent across these four Latin American countries. Intestinal disorders were the most common (35.5%), followed by gastroduodenal (11.9%), anorectal (10.0%), and esophageal disorders (5.8%)7.
The diagnosis of intestinal disorders is based on patient-reported clinical symptoms and the application of standardized criteria, such as the Rome IV criteria8. The severity of gastrointestinal symptoms is mainly assessed using the IBS Severity Scoring System (IBS-SSS), which has been validated in Spanish-speaking populations9.
Evidence indicates that between 20% and 90% of patients with DGBI, such as irritable bowel syndrome (IBS), present psychiatric symptoms or a formal psychiatric diagnosis, with depression being the most frequent comorbidity, followed by anxiety10-14. Personality, understood as the organization of structural and functional characteristics that shape a relatively stable pattern of affect, cognition, behavior, and motivation, determines how individuals respond to different situations and allows, to some extent, prediction of behavior15,16.
Several studies have explored the relationship between personality traits and IBS using different psychometric instruments. One of the most relevant studies is that by Farnam et al.17, which evaluated the association between personality traits and IBS in patients without psychiatric comorbidity using the NEO Personality Inventory. Findings indicated that among the five major personality factors assessed (neuroticism, extraversion, agreeableness, conscientiousness, and openness to experience), neuroticism and conscientiousness were the most prevalent traits in patients with IBS17, with women scoring higher than men in neuroticism, extraversion, and conscientiousness17.
Despite these advances, evidence regarding the relationship between personality traits and intestinal disorder symptoms of the gut-brain axis (ID-GBA) remains limited, particularly in Latin American populations, where studies are scarce and fragmented. In this context, further investigation into the relationship between personality traits and ID-GBA symptoms is warranted, as it may contribute to a better understanding of associated psychological factors.
Based on the above, the study hypothesis proposed that patients with a greater presence of ID-GBA symptoms exhibit a higher prevalence of personality traits associated with neuroticism and conscientiousness, and that these characteristics are associated with the severity of symptoms of gut-brain axis intestinal disorders.
Materials and methods
An observational, analytical, cross-sectional study was conducted in patients diagnosed with mental disorders treated at the Instituto Colombiano del Sistema Nervioso-Clínica Montserrat, both in the outpatient setting (Day Clinic) and inpatient unit, during the first half of 2025. The sample size was calculated using a 95% confidence interval (CI) and 12% variability, resulting in an initial sample of 136 participants. During data collection, five questionnaires were excluded (two due to failure to meet inclusion criteria and three due to incomplete administration), resulting in a final sample of 131 patients.
Participants aged 18 years or older with a diagnosis of a mental disorder who were receiving care in outpatient and inpatient services were included. Rome IV criteria were not applied to establish a formal diagnosis of irritable bowel syndrome. Accordingly, although participants did not have a confirmed IBS diagnosis, the IBS-SSS scale was administered to evaluate the severity of intestinal disorder symptoms. Patients with organic or oncological gastrointestinal pathology, active psychotic symptoms, psychomotor agitation, substance withdrawal syndrome, or cognitive impairment as determined by the treating clinician were excluded.
Instruments
The Irritable Bowel Syndrome Severity Scoring System (IBS-SSS), developed in 1997 by Francis et al. under the direction of Peter Whorwell, classifies IBS severity18. In 2011, the instrument was translated, culturally adapted, and validated in Spanish. Evidence demonstrated that the instrument is reproducible, sensitive to clinically relevant changes, and more applicable when the visual analog scale is replaced with a numerical scale8. It includes five items assessing abdominal pain (intensity and frequency), abdominal distension, satisfaction with bowel habits, and the impact of IBS on daily life over the previous 10 days. Each item is scored from 0 to 100 (total range: 0-500): <75 = remission, 75-175 = mild, 175-300 = moderate, and >300 = severe18.
The Personality Inventory for DSM-5 (PID-5) was developed by the American Psychiatric Association as part of the alternative model for personality disorders proposed in DSM-5. It consists of 220 items with four response options and assesses 25 personality trait facets and five broad personality domains in adults aged 18 years and older19. Its application is recommended for adult populations aged 18 years and older19.
Statistical analysis
Data were recorded using the REDCap platform and exported in CSV format for analysis using Jamovi v2.3 statistical software. A normality test was performed to assess sample distribution. Categorical variables were reported as absolute frequencies, and quantitative variables were summarized using measures of central tendency and dispersion. For bivariate analysis, nonparametric tests were used, including Spearman correlation and median comparison using the Kruskal-Wallis test.
Ethical considerations
The research protocol and informed consent form were approved by the Campo Abierto LTDA Research Ethics Committee (Record No. 221, May 2025). All participants provided written informed consent prior to inclusion. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and national regulations governing health research (Resolution 8430 of 1993 issued by the Colombian Ministry of Health). All collected data were handled with strict confidentiality and used exclusively for academic and scientific purposes.
Results
The sample consisted of 136 participants, with a mean age of 40.8 years (standard deviation [SD] = 15.5; range: 18-92). The majority were female (76.5%), and most participants received care in outpatient psychiatry and psychology services (56.6%). The predominant mental disorder diagnostic groups were depressive disorders (48.5%) and anxiety disorders (24.3%) (Table 1).
Table 1 Sociodemographic and clinical characteristics of the sample
| Variable | n (%) |
|---|---|
| Age, years (mean, SD) | 40.8 (+/-15.5) |
| Sex | |
| Female | 104 (76.5) |
| Male | 30 (22.1) |
| Other | 2 (1.5) |
| Marital status | |
| Single | 91 (66.9) |
| Married | 28 (20.6) |
| Cohabiting | 11 (8.1) |
| Separated | 5 (3.7) |
| Widowed | 1 (0.7) |
| Care setting | |
| Outpatient | 77 (56.6) |
| Inpatient | 59 (43.4) |
| Diagnostic group | |
| Anxiety disorders | 33 (24.3) |
| Depressive disorders | 66 (48.5) |
| Bipolar disorder | 15 (11.0) |
| Personality disorder | 1 (0.7) |
| Substance-related disorder | 4 (2.9) |
| Psychotic disorder | 1 (0.7) |
| Other | 16 (11.8) |
SD: standard deviation. Table prepared by the authors.
Regarding the assessment of gastrointestinal symptoms, the mean IBS-SSS score was 205 (SD = 100). Distribution by severity according to IBS-SSS scores showed that 42.6% of participants were classified within the moderate range, 16.9% within the severe range, 31.6% within the mild range, and 8.8% presented scores compatible with absence of symptoms or remission (Table 2, Figure 1).
Table 2 Distribution of participants according to severity ranges of ID-GBA symptoms based on IBS-SSS scores
| Total IBS-SSS score range | n | (%) |
|---|---|---|
| No disease or remission | 12 | 8.8 |
| Mild disease | 43 | 31.6 |
| Moderate | 58 | 42.6 |
| Severe | 23 | 16.9 |
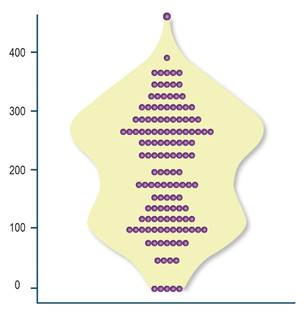
Figure 1 Distribution of severity ranges of ID-GBA symptoms according to IBS-SSS scores. Image property of the authors.
With respect to personality traits, mean scores according to PID-5 results were as follows: negative affect = 1.56 (SD = 0.64), detachment = 1.21 (SD = 0.59), antagonism = 0.79 (SD = 0.58), disinhibition = 1.16 (SD = 0.64), and psychoticism = 0.87 (SD = 0.65).
In the Kruskal-Wallis analysis comparing the severity of ID-GBA symptoms, as measured by the IBS-SSS, across personality domains, a statistically significant difference was observed for the detachment domain (chi-square [χ²] = 11.5; degrees of freedom [df] = 3; p = 0.009). This finding indicates that higher levels of detachment were associated with greater symptom severity (Table 3).
Table 3 Comparison of personality domains according to severity ranges of ID-GBA symptoms assessed using the IBS-SSS scale*
| Domain | χ² | df | p |
|---|---|---|---|
| Negative affect | 8.80 | 6 | 0.185 |
| Detachment | 9.48 | 6 | 0.148 |
| Antagonism | 2.90 | 6 | 0.821 |
| Disinhibition | 7.84 | 6 | 0.250 |
| Psychoticism | 4.31 | 6 | 0.635 |
*Results of the Kruskal-Wallis test. χ²: chi-square; df: degrees of freedom. Table prepared by the authors.
Pearson correlation analysis showed positive associations between total IBS-SSS score and the personality domains of negative affect (r = 0.176; p = 0.041), detachment (r = 0.250; p = 0.003), and psychoticism (r = 0.177; p = 0.039). These associations suggest that greater severity of ID-GBA symptoms is associated with higher scores in these personality traits (Table 4).
Discussion
This study aimed to determine whether an association exists between the five personality domains and the presence of intestinal disorder symptoms, with personality domains assessed using the PID-5 and symptom severity measured with the IBS-SSS. The study population consisted of patients with mental disorders receiving care at a mental health unit in Bogotá.
The literature reports a prevalence of DGBI in Latin America of 35.5%7, and disorders such as IBS show a strong association with psychiatric comorbidity, primarily depression and anxiety, with frequencies ranging between 40% and 90% according to different authors10-14. Consistent with these findings, the analyzed sample showed a high proportion of depressive disorders (48.5%) and anxiety disorders (24.3%). However, these percentages were lower than those reported by authors such as Mariños, who described prevalences exceeding 80%14.
Although the literature indicates a predominance of DGBI among women7, the present study did not allow evaluation of this relationship because the sample consisted predominantly of women (76.5%). This represents a limitation associated with convenience sampling. Regarding intestinal disorder symptoms, a mean IBS-SSS score of 205 was observed, corresponding to a moderate severity range. Most participants were classified within mild and moderate ranges, consistent with the clinical heterogeneity described for this disorder3.
Previous studies, such as that conducted by Farnam et al.17, have reported that neuroticism and conscientiousness are among the most frequent personality traits in patients with ID-GBA symptoms, including those diagnosed with IBS. Higher scores in neuroticism, extraversion, and conscientiousness have also been observed in women. In contrast, the findings of the present study showed that the domains of negative affect, detachment, and psychoticism were significantly correlated with the severity of ID-GBA symptoms, with no relevant differences observed across psychiatric diagnostic categories. This divergence may be explained by the use of different psychometric instruments and by the clinical characteristics of the sample, which included patients with psychiatric comorbidity. Nevertheless, both prior evidence and current findings highlight the relevance of personality traits as modulators of clinical expression and symptom severity in disorders of gut-brain axis.
The gut-brain axis, described as a bidirectional communication system between the central nervous system and the enteric nervous system, regulates both gastrointestinal functions and psychological responses associated with anxiety and depression1,2. In the sample analyzed in this study, a predominance of depressive disorders (48.5%) and anxiety disorders (24.3%) was observed, together with a high frequency of ID-GBA symptoms. According to the IBS-SSS, 42.6% of participants were classified within moderate ranges and 16.9% within severe ranges. However, given the sampling method and cross-sectional study design, causal relationships between these variables cannot be established. The positive correlation observed between severity of ID-GBA symptoms and the personality traits of negative affect, detachment, and psychoticism suggests that personality factors may amplify the clinical expression of this symptomatology. These findings reinforce the hypothesis that dysfunction of the gut-brain axis constitutes a shared mechanism linking affective disorders with gastrointestinal symptomatology.
In this regard, the finding of a significant correlation between the detachment domain and greater severity of ID-GBA symptoms provides a novel contribution relative to previous literature and suggests the relevance of integrating these dimensions into future therapeutic interventions, particularly among patients presenting with more severe gastrointestinal symptomatology.
Future studies could incorporate explicit comparisons between patients with ID-GBA symptoms and those without such symptoms. This approach would allow evaluation of potential differences in personality profiles within clinical populations.
Among the study limitations, its cross-sectional design precludes the establishment of causal relationships. Furthermore, the non-probabilistic convenience sampling resulted in a predominance of female participants (76.5%) and a high frequency of diagnoses of depression (48.5%) and anxiety (24.3%). These characteristics limit the generalizability of the findings to populations with different clinical profiles.
It is important to note that the findings of this study correspond to a population of patients with mental disorders in whom ID-GBA symptoms were identified, rather than to patients with a confirmed diagnosis of IBS according to Rome IV criteria. Therefore, caution is warranted when extrapolating these results to clinical gastroenterology populations. It is plausible that, in samples with a formal diagnosis of IBS, personality profiles and the magnitude of observed associations may differ. This underscores the need for future comparative studies in populations with and without a confirmed diagnosis.
The IBS-SSS scale, originally designed to assess symptom severity in patients with a confirmed diagnosis of IBS, was applied in this sample to quantify the intensity of ID-GBA symptoms rather than for diagnostic purposes. This application outside a confirmed diagnostic context represents a methodological limitation, and findings should be interpreted within this framework. Nevertheless, the findings highlight the potential for longitudinal research exploring the directionality between personality traits and the progression of gastrointestinal symptomatology, as well as studies integrating physiological biomarkers with psychological measures in order to further elucidate these associations.
Conclusions
The association between the personality traits of detachment, negative affect, and psychoticism and greater severity of intestinal disorder symptoms supports the hypothesis of an interaction between the gut-brain axis and psychological factors. These findings underscore the need for comprehensive therapeutic approaches that incorporate assessment of personality traits.

