











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
The management of eosinophilic esophagitis (EoE) should be multidisciplinary and coordinated by pediatric gastroenterologists, working collaboratively with allergists/immunologists (given their expertise in diverse therapeutic approaches and biologic therapies for atopic comorbidities, such as severe atopic dermatitis), nutritionists with training in allergy and EoE, pathologists, pediatricians, and speech-language pathologists1. Therapeutic decisions should be discussed with patients and their families and should aim to control symptoms and improve quality of life (Figure 1)2-6.
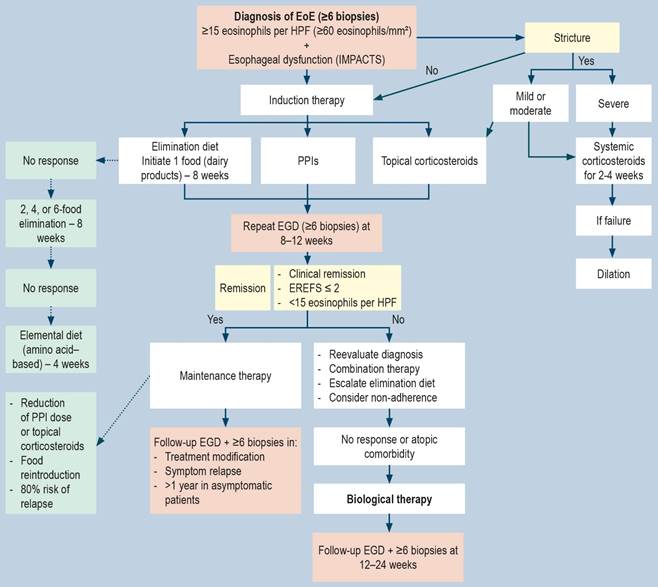
Figure 1 Comprehensive algorithm for the diagnosis and management of eosinophilic esophagitis: clinical evaluation, endoscopic confirmation, and therapeutic interventions. HPF: high-power field; EGD: esophagogastroduodenoscopy; EoE: eosinophilic esophagitis; Eos: eosinophils; EREFS: Endoscopic Reference Score; PPI: proton pump inhibitors; IMPACTS: Index of Symptoms and Impact of Eosinophilic Esophagitis. Adapted from: de Bortoli N, et al. Dig Liver Dis. 2024;56(6):951-633; Amil-Dias J, et al. J Pediatr Gastroenterol Nutr. 2024;79(2):394-4374.
Methodology
A literature search was conducted emphasizing the highest level of evidence, including clinical practice guidelines (CPGs) (AGREE-II), randomized controlled trials (RCTs), systematic literature reviews (SLRs), and meta-analyses. The databases PubMed, Medline, Embase, Cochrane, and LILACS were searched in both English and Spanish for the period 2014-2024. MeSH terms were used (eosinophilic esophagitis, guidelines, pediatric, evidence). Three CPGs were identified as the primary basis for the development of this consensus: two focused on pediatric populations-the guideline from the British Society of Gastroenterology (BSG) and the British Society of Pediatric Gastroenterology, Hepatology and Nutrition (BSPGHAN)7, and the guideline from the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN)4. For adult populations, the Italian consensus on the diagnosis and management of EoE was considered3. Two recent SLRs were also included: one addressing swallowed topical corticosteroids2 and another focused on dietary management5, as well as a meta-analysis on pharmacologic medical management6. These studies were selected based on their methodological rigor and the relevance of their updated evidence.
A multidisciplinary panel of 16 experts was convened, including members from the Colombian College of Pediatric Gastroenterology, Hepatology and Nutrition (COLGAHNP), allergists from the Colombian Association of Allergy, Asthma and Immunology (ACAAI), national pathologists, adult gastroenterologists from the Colombian Association of Gastroenterology (ACG), and four international experts. The panel formulated 18 clinical questions (8 related to diagnosis and 10 related to treatment). Panel members were selected based on their clinical and research expertise in gastroenterology, allergology, and pediatrics, with a minimum of five years of clinical experience and affiliations with academic institutions, referral hospitals, and national scientific societies. Additionally, four epidemiologists supported the process. All participants critically appraised the available literature to develop statements and recommendations.
Each statement was presented alongside the quality of evidence and strength of recommendation (strong or weak), according to the U.S. Preventive Services Task Force criteria (Table 1)8. A modified Delphi method was applied, including an initial round of electronic voting followed by a second in-person round conducted in a hybrid format. Each recommendation was evaluated using three response options: disagree, agree, or agree with modifications. Recommendations were considered approved when agreement reached ≥80% (strong agreement)9. The response rate was 100% in both rounds. In the first round, agreement exceeded 90% for all statements. Statements receiving the response “agree with modifications” were discussed collectively, reformulated, and resubmitted for voting during the hybrid meeting until consensus was achieved. An update of the consensus is recommended after 5 years. This study was sponsored by COLGAHNP, with no reported conflicts of interest.
Table 1 Classification of dietary strategies for eosinophilic esophagitis: characteristics, advantages, and limitations
| Type of diet | Recommendation | Efficacy (%) | References | |
|---|---|---|---|---|
| Empirical elimination diets* | 1 food | Milk and dairy products | 41-46 | 4,5,10,11) |
| 2 foods | Milk and dairy products, wheat/gluten | 43-44 | 4,5,10,11 | |
| 4 foods | Milk and dairy products, wheat/gluten, egg, soy | 41-55 | 4,5,10,11 | |
| 6 foods | Milk and dairy products, wheat/gluten, egg, soy, peanuts/tree nuts, fish and seafood | 40-65 | 4,5,10,11 | |
| Elemental diet (amino acid-based) | Formula only, no other foods | 95 | 4,5,10,11 | |
| Allergy test-directed diets | Skin prick testing | Not recommended | 39 | 4,5,10,11 |
| Patch testing | ||||
| Other: IgG4 | No robust evidence | 39 | 12 | |
*Other eliminated foods: legumes in Spain; sesame in Israel. IgG4: immunoglobulin G4. Adapted from: Amil-Dias J, et al. J Pediatr Gastroenterol Nutr. 2024;79(2):394-4374; Arias Á, et al. Nutrients. 2024;16(14):22315; Harris PR, et al. Rev Chil Pediatr. 2020;91(5):809-2710; Visaggi P, et al. Dig Liver Dis. 2023;55(2):208-2211; Chang JW, et al. Clin Gastroenterol Hepatol. 2023;21(7):1690-812.
What should be the therapeutic objectives in eosinophilic esophagitis?
Statement 1
Patients and their families should be educated regarding the chronic nature of the disease and the need for long-term treatment. Therapeutic objectives should include control of inflammation in all biopsies (<15 eosinophils per high-power field [HPF]) and prevention of tissue remodeling (fibrosis/stricture formation); achievement of endoscopic remission based on an EREFS score ≤2; reduction in symptom severity, assessed using the Pediatric Eosinophilic Esophagitis Symptom Score (PEESS), version 2.0; and improvement in quality of life, which should be measured using the Pediatric Quality of Life Inventory (PedsQL)3,13.
Level of evidence: II-2
Grade of recommendation: B
Agreement: 100%
What is the best strategy to initiate dietary therapy?
Statement 2
The preferred strategy is empiric elimination of one or more food antigens to induce remission, followed by endoscopic reassessment with esophageal biopsies 8-12 weeks later10, with the goal of achieving the least restrictive diet possible (ideally elimination of a single food antigen). The elemental diet is highly effective; however, it should be reserved for complex cases due to its high cost and lower adherence. Allergy test-directed diets lack robust supporting evidence. The selection of the food(s) to be eliminated should be individualized (Table 1)5,11,14-16.
Level of evidence: I-II
Grade of recommendation: A
Agreement: 100%
Good Practice Points
The elimination diet may follow either a step-up (ascending) approach, beginning with elimination of one or two foods and progressing to four- and six-food elimination (requiring fewer endoscopies), or a top-down (descending) approach, beginning with six-food elimination followed by gradual reintroduction. However, the latter approach requires more endoscopies, greater nutritional support, and is associated with lower adherence (Figure 2)14.
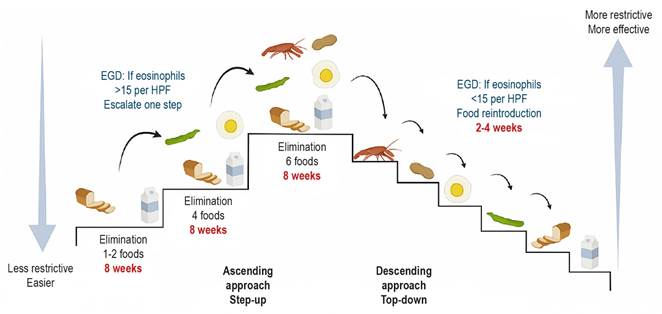
Figure 2 Comparison of step-up and top-down elimination diet approaches: number of foods restricted, duration, and clinical indications. *The elimination diet includes legumes in Spain and sesame in Israel. HPF: high-power field; EGD: esophagogastroduodenoscopy; eos: eosinophils. Adapted from: Visaggi P, et al. Best Pract Res Clin Gastroenterol. 2023;62-63:10182514; Votto M, et al. Front Pediatr. 2022;9:82019217.
Elimination diets may result in nutritional deficiencies, feeding difficulties, psychological distress, and impaired quality of life. Theoretically, they may also predispose to immunoglobulin E (IgE)-mediated allergies; therefore, careful individualization is required. The selection of dietary strategy depends on disease severity and nutritional status, the presence of feeding difficulties or food allergies, patient and family preferences, financial resources, and the need to evaluate response through esophagogastroduodenoscopy with biopsies at least 6-8 weeks after elimination of a food group5,11,15-17. Current research is evaluating transcriptomic profiling in the context of elimination diets16.
In the step-up elimination diet strategy: is initiation with single-food elimination (milk and dairy products) more effective than four- or six-food elimination for the treatment of eosinophilic esophagitis?
Statement 2.1
Single-food elimination (milk and dairy products) represents a reasonable initial therapeutic option within the step-up strategy and has demonstrated symptomatic and histologic improvement comparable to more restrictive diets (four- or six-food elimination). This approach requires fewer endoscopies, reduces costs, improves adherence, decreases the number of missed school and workdays, and enhances quality of life, achieving remission in 46.4%-51% of cases (Table 2, Figure 2)10,14,15,18,19.
Level of evidence: I
Grade of recommendation: A
Agreement: 100%
Table 2 Comparison of elimination diet strategies: advantages, disadvantages, and indications of step-up and top-down approaches
| Elimination strategy | ||
|---|---|---|
| Step-up | Top-down | |
| Advantages |
Early identification of food triggers. Shorter diagnostic process. Avoidance of unnecessary dietary restrictions. |
More restrictive diets are more effective. |
| Disadvantages | May be less effective. |
Greater number of endoscopies. Lower adherence. Risk of nutritional deficiencies. |
| Indication | Recommended in pediatric patients with mild to moderate symptoms. |
Adults or older pediatric patients. Significantly limiting symptoms. |
Adapted from: Votto M, et al. Front Pediatr. 2022;9:82019217.
Good Practice Points
In children, comparison of single-food elimination versus four-food elimination showed response rates of 44% versus 41% (p = 1.00), respectively. In adults, comparison of one-food versus six-food elimination demonstrated response rates of 34% and 40% (p = 0.58), respectively18. A recent randomized controlled trial evaluated single-food elimination (milk) (1FED) versus four-food elimination (milk, egg, wheat, and soy) (4FED) in patients aged 6-17 years over 12 weeks. The less restrictive diet was associated with better nutritional status. The discontinuation rate for the 4FED diet (32%) was significantly higher than for the 1FED diet (11%) (p = 0.0496)10. The step-up strategy beginning with dairy elimination has demonstrated effectiveness, reducing diagnostic time and the number of endoscopic procedures compared with the top-down strategy14. Endoscopic evaluation with biopsy should be performed 6-8 weeks after initiation of the elimination diet to assess treatment response (Figure 2)15.
In elimination diet strategies: which foods are eliminated, and how effective is two-food elimination compared with four- or six-food elimination in the treatment of eosinophilic esophagitis?
Statement 2.2
Standard two-food elimination (cow’s milk protein and wheat/gluten), four-food elimination (cow’s milk protein, wheat/gluten, egg, soy), or six-food elimination (cow’s milk protein, wheat/gluten, egg, soy, peanuts/tree nuts, fish and seafood) induces histologic remission in up to 63.9% of patients5. These approaches are slightly more effective than elimination of milk and dairy products alone in both children and adults; however, they are associated with lower adherence and increased nutritional risk4,5,10,11,14,15.
Level of evidence: I
Grade of recommendation: A
Agreement: 93.7%
Good Practice Points
Although more restrictive elimination diets may demonstrate greater effectiveness, they require evaluation by a nutrition specialist, involve a higher number of endoscopic procedures (increasing costs), and may be associated with nutritional deficiencies, feeding disorders, psychological disturbances, and reduced quality of life4,5,10,11. A recent meta-analysis demonstrated that empiric six-food elimination achieved histologic remission in 63.9% of patients and showed high homogeneity when exclusively pediatric patients with EoE were analyzed (67.5%) compared with adults (63.5%). Four-food elimination demonstrated effectiveness of 54.7% and was more effective in children (59.5%) than in adults (52.7%)5. During the food reintroduction phase, at least one daily serving of the reintroduced food should be consumed for 4-6 weeks before reassessment with endoscopy and biopsy15. Reintroduction should proceed from less allergenic to more allergenic foods: fish/seafood, peanuts/tree nuts, soy, egg, wheat/gluten, and finally milk (Tables 1 and 2; Figure 2)15.
Statement 2.3
Allergy test-guided elimination diets are not recommended as first-line dietary therapy because their effectiveness is lower than that of empiric and elemental diets5,12,20,21.
Level of evidence: I
Grade of recommendation: C
Agreement: 100%
Good Practice Points
A systematic review and meta-analysis21 reported overall effectiveness ranging from 39.5% to 45.7% for allergy test-guided elimination diets, with better outcomes observed in children than in adults (45.7% vs 26.4%). Variability was observed in allergy testing methods, types of allergens assessed, confirmation procedures, duration of food challenges, and criteria for treatment success, resulting in significant heterogeneity5.
A systematic review20 of 16 studies in children and adults demonstrated that elimination diets based on allergy testing achieved effectiveness of 66.7% when results from serum-specific IgE (sIgE), skin prick testing, and patch testing were combined; however, these approaches do not appear to be superior to empiric elimination diets20.
Statement 2.4
Amino acid-based formulas are highly effective (>90%) in achieving histologic remission; however, they are costly and associated with low adherence. Therefore, they are considered second-line therapy in complex cases4,5,11,22.
Level of evidence: I
Grade of recommendation: A
Agreement: 100%
Good Practice Point
Amino acid-based formulas are highly effective and act rapidly, inducing histologic remission in 95% of children with EoE. They should be administered for at least four weeks prior to endoscopic reassessment5. Their disadvantages include high cost and poor palatability, which negatively affects adherence; consequently, they are considered a second-line option. Their use is indicated in infants who have not yet initiated solid food intake, in patients with multiple food allergies, in those with growth failure, and in individuals with severe disease unresponsive to highly restrictive diets or pharmacologic therapy22. Swallowing therapy with puréed foods based on amino acid-based formulas should be continued to facilitate subsequent reintroduction of other foods4,5,11.
What is the role of proton pump inhibitors in inducing and maintaining remission of eosinophilic esophagitis?
Statement 3
Proton pump inhibitors (PPIs) are a treatment of choice in the management of EoE and have been described as the most cost-effective pharmacologic strategy, with an efficacy of approximately 50% in the pediatric population that is maintained over the long term (Table 3)23-32.
Level of evidence: I-II
Grade of recommendation: A
Agreement: 100%
Table 3 Induction and maintenance regimens with proton pump inhibitors: recommended doses, formulations, and administration
| Medication | Induction dose | Maintenance dose* | Formulations | Administration |
|---|---|---|---|---|
| Omeprazole / Esomeprazole | 1 mg/kg per dose, twice daily (max. 40 mg every 12 h) | 1 mg/kg/day (max. 40 mg/day) |
Tablets, capsules** 20-40 mg, 10 mg sachets |
15-20 minutes before breakfast or dinner |
| Lansoprazole | 0.75 mg/kg per dose, twice daily (max. 30 mg every 12 h) | 0.75 mg/kg/day (max. 30 mg/day) |
Tablets*** 15-30 mg |
*Maintenance dose should subsequently be reduced to the lowest effective dose. **A formulation of esomeprazole designed for dissolution in water is available. ***An orally disintegrating formulation is available. Adapted from: Gutiérrez Junquera C, et al. An Pediatr. 2020;92(6):376.e1-376.e1025.
Good Practice Points
PPIs improve EoE by blocking eotaxin-3, ICAM-1, and VCAM-1. Their role in eosinophil migration has been demonstrated through attenuation of IL-13-induced chemokine secretion and adhesion molecules, as well as improvement of esophageal barrier function26. They represent the most frequently used first-line option, with reported histologic response rates ranging from 23% to 83%27. In a retrospective Colombian study, histologic remission was achieved in 47% of patients28.
A meta-analysis including 619 patients treated with PPIs (188 children), across 33 studies (11 prospective), reported histologic remission in 50.5% of cases, with no difference between children and adults, and maintenance of remission in up to 73% with a low-dose regimen29. The European multicenter EoE CONNECT study, including 630 patients (76 children), reported clinicopathologic remission in 48.9%27. PPIs irreversibly inhibit the H+/K+ ATPase pump and may be particularly beneficial in patients with concomitant gastroesophageal reflux disease (GERD). EoE may coexist with GERD due to impaired esophageal clearance; therefore, PPI therapy may provide clinical benefit by reducing gastric acid production30.
Greater efficacy during the induction phase has been observed in the inflammatory phenotype and with higher doses (2 mg/kg/day; maximum 80 mg/day). Conversely, common CYP2C19*17 and STAT6 variants have been associated with reduced therapeutic response, suggesting a potential genotype-guided approach24,31,32. The long-term safety profile remains controversial. In a randomized controlled trial including 17,598 adult patients followed for a median of 3.01 years, pantoprazole was not associated with adverse effects, except for a slightly increased risk of gastrointestinal infections23.
What is the role of topical corticosteroids in inducing and maintaining remission of eosinophilic esophagitis?
Statement 4
Swallowed topical corticosteroids are safe and effective, with good adherence and a favorable safety profile for both induction and maintenance of remission, with rare complications. No evidence demonstrates superiority between viscous budesonide and swallowed fluticasone. Dose reduction or alternate-day dosing may result in relapse; therefore, endoscopic reassessment is recommended. Food intake should be avoided for one hour after administration of the topical corticosteroid (Table 4)2,6,33-36.
Level of evidence: I
Grade of recommendation: A
Agreement: 100%
Table 4 Topical corticosteroids for EoE: recommended induction and maintenance doses, clinical response, and adverse effects
| Topical corticosteroid | Age | Induction dose | Maintenance dose | Adverse effects | Response |
|---|---|---|---|---|---|
| Viscous budesonide* | <10 years | 0.5 mg per dose (twice daily) | 0.5 mg per dose (once daily) |
Adrenal insufficiency 1% Osteopenia 1% Esophageal candidiasis 4% |
64.9% in 8 RCTs (n = 437) vs 13.3% with placebo |
| >10 years | 1 mg per dose (twice daily) | 1 mg per dose (once daily) | |||
| Liquid fluticasone** | <10 years | 400 μg per dose (twice daily) | 400 μg per dose (once daily) | ||
| >10 years | 800 μg per dose (twice daily) | 800 μg per dose (once daily) |
*Avoid grapefruit intake: inhibits CYP3A. **Release contents onto the base of the tongue. RCTs: randomized controlled trials. Adapted from: Harris PR, et al. Rev Chil Pediatr. 2020;91(5):809-279; Gutiérrez Junquera C, et al. An Pediatr. 2020;92(6):376.e1-376.e1025; McCallen JD, et al. J Clin Gastroenterol. 2025;59(8):737-74335.
Good Practice Points
In March 2024, swallowed topical corticosteroids were approved by the U.S. Food and Drug Administration (FDA) for the management of EoE. A systematic review and meta-analysis demonstrated histologic improvement in more than 63% of patients compared with placebo (relative risk [RR]: 11.94; 95% confidence interval [CI]: 6.56-21.75; number needed to treat [NNT] = 3), although little to no endoscopic improvement was observed (RR: 2.60; 95% CI: 0.82-8.19). No significant differences were observed in total adverse events (RR: 1.14; 95% CI: 0.94-1.40) or serious adverse events (RR: 0.35; 95% CI: 0.17-0.73) compared with placebo6.
Comparison between viscous budesonide and swallowed fluticasone demonstrated no significant differences in clinical outcomes (mean difference [MD]: −0.60; CI: −3.78-2.58), histologic outcomes (RR: 1.13; CI: 0.84-1.51), endoscopic outcomes (MD: 0.70; CI: −0.03-1.43)6, or total adverse events (RR: 0.92; CI: 0.15-5.56). Induction therapy should be administered for a minimum of 3 months at age-appropriate doses. Maintenance therapy should be continued at half the induction dose for at least 1-2 years to prevent relapse (Table 4), with dose reduction by half every 6-12 months under endoscopic monitoring2. Long-term adverse effects are uncommon; however, concomitant corticosteroid exposure for other conditions (oral, topical, inhaled, or intranasal) should be considered. A recent study evaluating the effectiveness and safety of swallowed topical corticosteroids in children and adults demonstrated sustained long-term efficacy (mean follow-up: 6.5 years), with improved adherence and rare complications: adrenal insufficiency (1%), osteopenia (1%), and esophageal candidiasis (4%)35.
Dose reduction of topical corticosteroids may lead to recurrence of EoE. A pediatric study demonstrated a 100% relapse rate with alternate-day dosing. Given the favorable long-term safety profile of topical corticosteroids, continuation of the standard dose without reduction may be more effective and safer. If dose reduction is implemented, endoscopic reassessment should be performed36.
What is the role of biologic therapy in inducing and maintaining remission of eosinophilic esophagitis?
Statement 5
Dupilumab may be used as a second-line therapy in patients with EoE refractory to conventional treatment or in those experiencing adverse events that limit its use. Patients with EoE and concomitant atopic comorbidities (dermatitis, asthma, or chronic rhinosinusitis) who meet clinical criteria for biologic therapy based on the underlying comorbid condition may receive dupilumab regardless of EoE severity. Its use as first-line therapy may be limited by cost when compared with topical corticosteroids24,37-42.
Level of evidence: I
Grade of recommendation: A
Agreement: 100%
Good Practice Points
Dupilumab is a monoclonal antibody that inhibits the alpha subunit of the interleukin-4 and interleukin-13 receptor. It has been approved by the FDA for patients with EoE aged ≥12 years and weighing ≥40 kg since 2022, and for children aged ≥1 year and weighing ≥15 kg since 2024. Real-world studies have demonstrated effectiveness exceeding 90% in achieving histologic remission37-39.
Evaluation of treatment response to dupilumab should include esophagogastroduodenoscopy with biopsies 5-6 months after treatment initiation, following dose adjustment, or in the presence of symptom worsening. Recommended weight-based dosing is as follows: 200 mg every two weeks for children weighing 15-30 kg; 300 mg every two weeks for those weighing 30-40 kg; and 300 mg weekly for patients weighing more than 40 kg41. Adverse effects have been reported in approximately 2% of patients and include injection-site reactions, upper respiratory tract infections, arthralgia, and headache40,41.
Most patients receiving dupilumab achieve significant clinical and histologic improvement 12-24 weeks after initiation of standard weight-based dosing. Currently, no evidence supports dose reduction or treatment discontinuation after this period. Continuation of therapy is recommended to achieve and maintain disease remission42. Topical corticosteroids may be gradually discontinued once dupilumab induces histologic remission. PPIs may be continued in the presence of concomitant GERD. Elimination diets should be individualized. Although no significant pharmacologic interactions between dupilumab and these therapies have been established, decisions regarding continuation or discontinuation of concomitant treatments should be individualized42.
How should patients with eosinophilic esophagitis be followed?
Statement 6
Clinical follow-up should be conducted periodically using the PEESS v2 questionnaire. Treatment modifications should be evaluated endoscopically after 8-12 weeks for elimination diets, topical corticosteroids, or proton pump inhibitors (PPIs), and no less than 4 weeks for exclusive elemental diets. In cases of relapse or non-response, endoscopic and histologic reassessment is required during maintenance therapy, and the timing should be individualized. Clinical, endoscopic, and histologic remission should be clearly defined. In asymptomatic patients, endoscopic reassessment should be considered 1-3 years after sustained remission due to the risk of fibrotic progression4,7,43-45.
Level of evidence: III
Grade of recommendation: B
Agreement: 100%
Good Practice Points
The PEESS v2 is a validated instrument for assessing symptoms during maintenance therapy. Clinical remission should be evaluated regularly during follow-up43, given the correlation between reported symptoms and eosinophil counts in the distal esophagus (p < 0.05)44. Twenty-four-hour pH-impedance monitoring has been evaluated as a diagnostic tool for gastroesophageal reflux disease (GERD) or non-response to PPIs in relation to alterations in baseline nocturnal impedance and its association with eosinophil counts in biopsy samples. Additional studies are required7,45.
Treatment adherence is a key component of patient follow-up, as multiple barriers extend beyond clinical factors. First, the presence of adverse effects that may reduce adherence should be considered (Table 5). Second, additional factors such as barriers to accessing recommended therapies should be evaluated. A recent study identified limited food options, food insecurity, and difficulty maintaining dietary restrictions outside the home as significant challenges for families implementing elimination diets46. Similarly, an earlier study demonstrated that the cost of acquiring foods meeting dietary requirements constitutes a major source of caregiver stress, together with the need to prepare specialized meals47. These findings confirm that adherence depends not only on patient engagement but also on family support and on the availability and affordability of appropriate foods. These factors should be considered when designing sustainable therapeutic strategies.
Table 5 Most frequent adverse effects of pharmacologic treatments for eosinophilic esophagitis
| Treatment | Common adverse effects | Clinical considerations | References |
|---|---|---|---|
| Proton pump inhibitors | Increased risk of gastrointestinal and respiratory infections | Generally well tolerated; long-term use has been associated with hypomagnesemia and vitamin B12 deficiency | 4,6,7,23,27,31,32 |
| Topical corticosteroids (viscous budesonide, liquid fluticasone) | Adrenal insufficiency 1%, osteopenia 1%, esophageal candidiasis 4% | Low risk of systemic effects; isolated cases of adrenal insufficiency and bone alterations with prolonged use | 2,4,6,7,33-35 |
| Systemic corticosteroids (prednisone, prednisolone) | Weight gain, hypertension, hyperglycemia, osteoporosis, adrenal suppression | Not recommended for chronic therapy; reserved for severe and refractory cases | 4,6,7,48 |
| Biologics (dupilumab) | Injection-site reactions, headache, conjunctivitis, arthralgia | Favorable safety profile in clinical trials; additional data are needed for long-term pediatric use | 37,38,40 |
Adapted from: Chan J, Flynn DM, Gordon M, Parmar R, Moolenschot K, Jackman L, et al. Swallowed topical steroid therapy for eosinophilic oesophagitis in children: practical, evidence-based guidance by the BSPGHAN Eosinophilic Oesophagitis Working Group. BMJ Paediatr Open. 2024;8(1):e002467-e0024672; Amil-Dias J, et al. J Pediatr Gastroenterol Nutr. 2024;79(2):394-4374; Franciosi JP, et al. Cochrane Database Syst Rev. 2023;2023(7):CD0040656; Dhar A, et al. Gut. 2022;71(8):1459-877; Shah SC, et al. Clin Gastroenterol Hepatol. 2019;17(11):2185-2198.e323; Laserna-Mendieta EJ, et al. Aliment Pharmacol Ther. 2020;52(5):798-80727; Mougey EB, et al. J Pediatr Gastroenterol Nutr. 2019;69(5):581-731; Chevalier R, et al. Expert Opin Drug Metab Toxicol. 2023;19(2):53-632; Bose P, et al. J Pediatr Gastroenterol Nutr. 2020;70(3):324-933; Philpott H, et al. Aliment Pharmacol Ther. 2018;47(8):1071-834; McCallen JD, et al. J Clin Gastroenterol. 2025;59(8):737-74335; Russin M, et al. Am J Gastroenterol. 2025;120(3):663-66637; Chehade M, et al. N Engl J Med. 2024;390(24):2239-5138; Aceves SS, et al. Ann Allergy Asthma Immunol. 2023;130(3):371-840; Al-Hussaini A. J Pediatr Gastroenterol Nutr. 2016;63(5):474-8048.
What are the predictors of treatment response and risk factors for esophageal tissue remodeling or stricture formation in patients with eosinophilic esophagitis?
Statement 7
Delayed diagnosis of EoE is the most important risk factor for the development of esophageal strictures. Early initiation of treatment during the course of the disease may prevent esophageal tissue remodeling or stricture formation49-52.
Level of evidence: II-2
Grade of recommendation: B
Agreement: 100%
Good Practice Points
The prevalence of esophageal strictures and their occurrence over time has been demonstrated during longitudinal follow-up of patients with EoE and is proportional to the interval between symptom onset and diagnosis: 0-2 years: 17.2%; >2-5 years: 30.8%; >5-8 years: 38.9%; >8-11 years: 37.9%; >11-14 years: 41.7%; >14-17 years: 64.3%; >17-20 years: 66.7%; and >20 years: 70.8% (p < 0.001). Diagnostic delay was identified as a risk factor for stricture formation (odds ratio [OR]: 1.08 per year; 95% confidence interval [CI]: 1.04-1.12; p < 0.001)49. Patients with delayed diagnosis and late initiation of treatment more frequently presented with dysphagia and food impaction50. Poor response to topical corticosteroids has been observed more frequently in patients with strictures (28% vs 12%, p = 0.005) or in those requiring dilation (37% vs 19%, p = 0.006)51.
In which patients is esophageal dilation indicated secondary to eosinophilic esophagitis, and how should it be performed?
Statement 8
Endoscopic dilation should be considered in patients with moderate or severe strictures who continue to experience dysphagia despite adequate treatment with proton pump inhibitors (PPIs), topical corticosteroids, elimination diets, or dupilumab. A four-week course of systemic corticosteroids is recommended in cases of severe acute stricture with dysphagia or food impaction requiring rapid symptomatic improvement, particularly when adequate nutritional intake cannot be ensured. Both hydrostatic balloon dilation and Savary-Gilliard bougie dilation are effective and safe in pediatric patients, with low complication rates. These approaches should be considered in patients who do not respond to systemic corticosteroids or who present with severe strictures at diagnosis, combined with corticosteroid therapy. The dilation method should be selected according to the endoscopist’s expertise4,7,48-51,53-59.
Level of evidence: II
Grade of recommendation: B
Agreement: 100%
Good Practice Points
Strictures can be classified into three severity grades: mild, when a standard 9 mm endoscope can pass; moderate, when a 6 mm pediatric endoscope can pass; and severe, when a 6 mm pediatric endoscope cannot pass4. In a study including 20 patients (mean age: 10.6 ± 4.2 years), 16 had moderate strictures and four had severe strictures. Eighteen patients received oral systemic corticosteroids (prednisone 1-2 mg/kg/day in one or two daily doses) for four weeks, and two initially received intravenous corticosteroids (methylprednisolone). Seventeen patients (85%) received PPIs and nine (45%) initiated elimination diets. All patients demonstrated clinical improvement, and 15 of 20 became asymptomatic. Resolution of the stricture was observed endoscopically in 19 of 20 patients, and histologic remission was achieved in 13 of 20. Minor adverse effects were reported: hyperphagia (10/20), weight gain (5/20), hyperactivity (2/20), and acne (1/20). Ultimately, esophageal dilation was required in 3 of 20 patients during a follow-up period of 48.5 months54. Mild inflammatory strictures may resolve with standard treatment using PPIs, dietary restriction, or topical corticosteroids55. Dilation does not control underlying inflammation; therefore, it should be combined with standard induction and maintenance therapies4, particularly topical corticosteroids, which demonstrate greater effectiveness7,48-56.
A meta-analysis including 1,890 dilations in children and adults reported a very low perforation rate of 0.38%, confirming that dilation is safe and effective, with no differences between Savary bougies and balloon dilation57. Hydrostatic balloons allow direct visual inspection during and after dilation; however, their main limitation is the presence of multiple or long strictures, which may be more easily treated using Savary-Gilliard bougies. Both techniques should begin with a small dilation diameter and increase progressively in 1 mm increments (not exceeding 3 mm per session) until symptom resolution is achieved4,58. A satisfactory dilation target should consider the esophageal diameter according to patient age: <9 months: 8 mm; 9-23 months: 10 mm; 24 months to 5 years: 12 mm; and >6 years: 14 mm(7.53). Intralesional corticosteroid administration, such as triamcinolone, may be beneficial and has demonstrated potential to increase the final achieved diameter, although it does not appear to reduce the number of required dilations59. Another alternative is EsoFLIP, a method shown to be faster than balloon dilation and associated with reduced fluoroscopy requirements60. Expert consensus guidelines on dilation techniques have been published internationally53,61.
Quality of life in patients with eosinophilic esophagitis
Statement 9
The Pediatric Quality of Life Inventory (PedsQL) Eosinophilic Esophagitis Module is an appropriate instrument for assessing health-related quality of life across different pediatric age groups, together with parental input, and has undergone cross-cultural adaptation into Spanish. This assessment provides a comprehensive evaluation of physical, emotional, and social impact and allows assessment of outcomes from individualized therapeutic interventions62-65.
Level of evidence: II-2
Grade of recommendation: B
Agreement: 100%
Good Practice Points
In pediatric patients, the PedsQL scale has been translated, cross-culturally adapted, and validated in Spanish in Spain63. High reliability and validity have been demonstrated in multiple studies64. This instrument enables monitoring of treatment impact and shows that more restrictive elimination diets are associated with poorer quality-of-life scores (p < 0.001)65.
Recommendations for transition to adult care
Statement 10
Transition should be individualized for each patient and family, involving a multidisciplinary team including pediatric and adult gastroenterologists, nutritionists, nurses, and psychologists, to ensure adequate preparation of adolescent patients and their families for an appropriate transfer of care. The involvement of a transition coordinator is recommended4,66-68.
Level of evidence: II-2
Grade of recommendation: B
Agreement: 100%
Good Practice Points
This process should ideally be led by a transition coordinator4. Instruments such as the STARx (Self-Management and Transition to Adulthood with Rx) questionnaire may be used to assess disease-related knowledge and readiness for successful transition. The questionnaire includes 18 items on a 5-point scale and evaluates six domains, with scores ranging from 0 to 90. Higher scores indicate greater readiness for transition66. The instrument has been translated into Spanish but has not undergone cultural validation in the Colombian context67. Studies indicate that 78% of patients and 76% of family members lacked knowledge regarding the transition process and demonstrated low levels of readiness according to the STARx questionnaire66. Barriers to transition include adolescent resistance and reduced adherence to treatment, highlighting the need for stronger parental involvement; limited physician training and experience in transitional care; and healthcare system limitations, including a scarcity of multidisciplinary teams and lack of insurance coverage for transition programs. Multidisciplinary participation should be ensured during the transition process, and continued development of national and international guidelines is recommended68.

