











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Inflammatory bowel disease (IBD) is a chronic inflammatory condition characterized by a relapsing-remitting course and the absence of curative treatment. It encompasses Crohn’s disease (CD) and ulcerative colitis (UC). IBD affects millions of individuals worldwide and imposes a substantial burden on both patients and healthcare systems1,2. The introduction of monoclonal antibodies targeting tumor necrosis factor alpha (anti-TNF-α) in the late twentieth century represented a major therapeutic advance in the management of IBD. These agents led to significant improvements in clinical outcomes, including sustained clinical remission, prevention of complications, and improved quality of life3,4. The first anti-TNF agent developed was infliximab4. Subsequently, other anti-TNF agents emerged, including adalimumab, golimumab, and certolizumab, all of which received approval for the treatment of UC or CD5. Since 2013, biosimilars of infliximab and adalimumab have also been approved for the treatment of IBD2.
Anti-TNF agents appear to exert a protective effect against the development of colorectal cancer in patients with both UC and CD, likely as a result of effective control of inflammation rather than an intrinsic antitumor mechanism6. In contrast, uncertainty persists regarding the association between anti-TNF therapy and the risk of anorectal cancer (ARC). Nevertheless, the broader relationship between anti-TNF agents and malignancy, particularly in patients with IBD, has been extensively explored. Several systematic reviews and meta-analyses have evaluated the risk of malignancy associated with anti-TNF therapy in patients with IBD. A systematic review conducted by Müller et al. found no significant association between anti-TNF use and an increased overall risk of malignancy, although one study reported an increased risk of lymphoma7. Similarly, Williams et al. conducted a meta-analysis in which no increased risk of malignancy was observed with anti-TNF therapy compared with placebo, although the available data were limited to short-term follow-up8. In a cohort study by Andersen et al., no significant increase in overall cancer risk associated with anti-TNF therapy was reported among patients with IBD, with a median follow-up of 3.7 years9. Furthermore, Targownik and Bernstein emphasized that although anti-TNF agents may increase the risk of nonmelanoma skin cancer, limited evidence suggests a meaningful increase in the risk of other malignancies, including ARC, beyond risks attributable to the underlying disease and concomitant therapies10.
Overall, some concern persists regarding specific malignancies such as lymphoma; however, current evidence does not suggest a significant association between TNF inhibitors and an increased risk of ARC. Nevertheless, long-term data remain limited, and further research is required to fully characterize the long-term cancer risks associated with anti-TNF therapy. In the current context of colorectal cancer (CRC) and anal squamous cell carcinoma in patients with IBD receiving anti-TNF therapy, attention has focused on the potential impact of these agents on neoplasia risk. Available evidence suggests that patients with IBD treated with anti-TNF agents may have a reduced risk of CRC due to effective control of chronic inflammation. In contrast, the risk of anal squamous cell carcinoma remains less clearly defined. Evidence indicates that the benefits of TNF inhibitors in controlling inflammation outweigh potential cancer risks6,11. Consequently, an important knowledge gap persists regarding the relationship between anti-TNF use and the risk of CRC and anal squamous cell carcinoma in patients with IBD. The objective of this review is to evaluate the current state of knowledge regarding this association from multiple perspectives, based on the evidence available to date.
Methods
This study constitutes a narrative literature review examining the relationship between anti-TNF therapy and the risk of ARC in patients with inflammatory bowel disease. The stages of the literature review included literature search, article selection, and reference screening of selected studies. Additionally, some articles cited in the reference lists of selected publications were incorporated into the final selection when they met predefined criteria (described below). During the first phase of the review, an initial search was conducted between February 2024 and November 2024 using the following parameters: databases and metasearch engines included PubMed, ScienceDirect, Embase, SciELO, Cochrane, and MEDLINE. Search terms included: “Tumor Necrosis Factor Inhibitors,” “Rectal Diseases,” “Anorectal,” “Neoplasms,” “Neoplasms by Site,” “Inflammatory Bowel Diseases,” “Ulcerative Colitis,” and “Crohn’s Disease.” Timeframe: no restrictions. Languages: English and Spanish. Study types included clinical practice guidelines, observational studies, randomized controlled trials, systematic reviews and meta-analyses, case series, and case reports. Eligibility criteria included use of evidence grading systems and recommendation strength classifications, as well as publication by authors affiliated with internationally recognized institutions. Following the initial search, titles and abstracts were independently reviewed according to the eligibility criteria described above and assessed for consistency with the objective of the literature review.
Results
Defining criteria
In clinical practice, attributing ARC to anti-TNF therapy first requires a comprehensive evaluation of the patient’s clinical history8,12, including assessment of other cancer risk factors, as well as careful review of evidence supporting an association between these agents and cancer risk (Figure 1):
Temporal association: development of anorectal cancer after initiation of anti-TNF therapy.
Exclusion of alternative risk factors: consideration of other potential risk factors for ARC.
Biological plausibility: understanding potential mechanisms by which anti-TNF therapy could contribute to carcinogenesis.
Epidemiological evidence: data from studies suggesting increased incidence of ARC among patients receiving anti-TNF therapy.
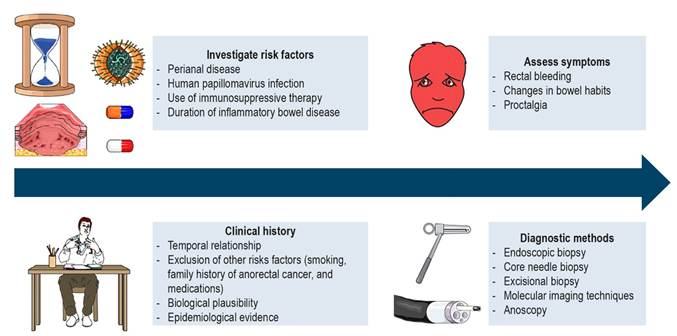
Figure 1 Considerations in the diagnostic approach to anorectal cancer in relation to the use of tumor necrosis factor inhibitors in patients with inflammatory bowel disease. Image created using Servier Medical Art figures under their terms of use, based on: Muller M, et al. J Crohn’s Colitis. 2021;15(5):840-597; Williams CJM, et al. Aliment Pharmacol Ther. 2014;39(5):447-588; Andersen NN, et al. JAMA. 2014;311(23):2406-139; Targownik LE, et al. Am J Gastroenterol. 2013;108(12):1835-4210; Townsend CM, et al. Dig Dis Sci. 2021;66(12):4436-4012; Axelrad JE, et al. Clin Gastroenterol Hepatol. 2024;22(7):1365-7213; Laredo V, et al. Cancers (Basel). 2023;15(3):87114; Matsuno H, et al. Digestion. 2016;94(1):24-915.
Epidemiology
Recent data indicate an increased risk of anal cancer among patients with IBD who present specific risk factors. However, according to current evidence, the use of TNF inhibitors does not appear to significantly modify the risk of anorectal tumors7,8,13. Individuals with CD have a higher risk of developing anal cancer, particularly anal squamous cell carcinoma, especially in the presence of anal or perianal lesions. The CESAME study demonstrated that patients with IBD and anal or perianal lesions had a higher incidence rate of anal squamous cell carcinoma (2.6 per 10,000 person-years) compared with those without such lesions (0.8 per 10,000 person-years)13. Risk factors for anal cancer in this population include human papillomavirus (HPV) infection13. Among patients with IBD, a higher risk of ARC has been observed in those with anal or perianal CD13,16.
Systematic reviews and meta-analyses suggest that anti-TNF agents do not significantly increase the risk of cancer in patients with IBD, including anorectal tumors. The principal malignancy-related concerns associated with anti-TNF therapy are lymphoma and nonmelanoma skin cancer rather than anorectal cancer7,8.
Risk factors
The main risk factors for ARC in patients with IBD receiving anti-TNF agents are not specifically detailed in the medical literature. However, several general risk factors for anorectal cancer in patients with IBD can be identified (Figure 1):
Perianal disease: patients with CD and long-standing perianal fistulas have an increased risk of anal cancer. The CESAME study demonstrated this elevated risk, particularly in individuals with anal or perianal lesions13.
HPV infection: a well-established risk factor for anal squamous cell carcinoma. Its presence may increase risk in patients with IBD13.
Chronic inflammation: persistent inflammation in the anorectal region, commonly observed in IBD, may contribute to carcinogenesis13,14.
TNF inhibitors do not appear to be associated with an increased risk of ARC. However, combination therapy with thiopurines may increase the risk of certain malignancies, including lymphoma and nonmelanoma skin cancer7,10,14.
Regarding disease duration, longer duration of IBD has been associated with an increased overall risk of malignancy, although data specifically addressing ARC remain limited17.
Pathophysiology
The pathophysiology of ARC in patients with IBD treated with anti-TNF agents is not well characterized. Its relationship with CRC in patients with IBD continues to be investigated. TNF-α is a key proinflammatory cytokine involved in the pathogenesis of IBD, and its inhibition constitutes a cornerstone of biological therapy. The principal mechanism of action involves reduction of inflammation, a well-established risk factor for CRC in patients with IBD6,18. By controlling inflammation, anti-TNF agents may reduce the risk of CRC6. The role of TNF-α in immune surveillance and tumor suppression is complex. TNF-α contributes to immune recognition and elimination of malignant cells; therefore, its inhibition could theoretically interfere with this process and increase malignancy risk10,19. Nevertheless, current evidence does not support an increased risk of neoplasia, including CRC, despite this theoretical concern8,10. In animal models, TNF-α appears to be redundant in colitis-associated carcinogenesis, as other proinflammatory cytokines compensate for its absence19. This finding may explain why TNF inhibition does not significantly increase cancer risk in clinical settings.
Anti-TNF agents have been shown to induce apoptosis of T cells in patients with IBD through tumor necrosis factor receptor 2 (TNFR2) and membrane-bound TNF (mTNF) expressed on CD14+ macrophages, which may explain their anti-inflammatory effects20. This mechanism may also play a role in modulation of the intestinal immune environment, potentially influencing cancer risk.
In summary, TNF inhibitors are effective in controlling inflammation associated with IBD. Further studies are required to fully elucidate the underlying mechanisms and their clinical implications.
Clinical presentation
ARC in patients with IBD, irrespective of TNF inhibitor use, typically presents with symptoms such as rectal bleeding, changes in bowel habits, and proctalgia. These symptoms may overlap with those of IBD, which can delay early diagnosis. Regular surveillance and a high index of suspicion are essential for early detection7.
Ogawa et al. investigated the relationship between infliximab therapy and anorectal cancer in patients with perianal CD. A small subgroup of patients undergoing surgery for perianal CD developed ARC associated with perianal fistulas. These patients presented with advanced-stage cancer and had received infliximab prior to cancer diagnosis, often due to progression of anal lesions21. These findings suggest that patients with long-standing anal fistulas, particularly those receiving anti-TNF agents such as infliximab, may be at increased risk of developing ARC. The results also highlight the importance of careful inspection and biopsy of anal lesions before initiating infliximab therapy in such cases.
Diagnosis
Diagnosis of ARC in patients with IBD receiving TNF antagonists requires integration of comprehensive clinical history assessment with complementary diagnostic tests (Figure 1), including endoscopic biopsy, core needle biopsy, and excisional biopsy, frequently complemented by advanced imaging techniques15,22-24. Particularly in patients with long-standing perianal disease, regular surveillance and a high index of suspicion are essential for early detection15,22. Endoscopic biopsy constitutes the cornerstone of ARC diagnosis. It allows direct visualization and tissue sampling of suspicious lesions. In the study conducted by Matsuno et al.15, various biopsy methods were evaluated for cancer detection in patients with CD, and endoscopic biopsy demonstrated a detection rate of 5.56%. This method is essential for obtaining tissue samples for histopathological examination15.
Core needle biopsy is most commonly used in the perianal region when endoscopy is impracticable due to stenosis or severe inflammation. One study reported a detection rate of 1.85% for CRC using core needle biopsy. This technique may be useful when endoscopic evaluation cannot be performed15. Excisional biopsy involves surgical removal of part of the lesion. In the study by Matsuno et al., this method demonstrated a detection rate of 5.88%. It is useful for larger or more accessible lesions and provides sufficient tissue for histopathological evaluation15. Endoscopic surveillance under anesthesia may be considered in patients with perianal pain or stenosis. This approach allows more thorough and less painful examination and biopsy15.
Molecular imaging techniques represent valuable tools in the evaluation of IBD and associated neoplasia. Intracolonic ultrasound targeting membrane-bound TNF--α (mTNF-α) enables quantitative detection of TNF-α expression in the intestinal mucosa. Furthermore, the use of fluorescent anti-TNF antibodies during confocal laser endomicroscopy has shown promise for predicting therapeutic response and could potentially be adapted for surveillance purposes22,23. These approaches are not yet standardized, and their clinical applicability remains uncertain. Random biopsies may identify “invisible” neoplastic lesions; however, their utility in detecting colorectal neoplasia in IBD is controversial. Detection rates are generally low, and the approach increases procedural time and cost24.
High-resolution anoscopy and inflammatory bowel disease
High-resolution anoscopy (HRA) is used to identify precancerous squamous cell lesions25. Squamous cell carcinoma of the anal canal and anal margin occurs approximately three times more frequently in immunocompromised individuals than in the general population. Incidence rates may reach 5.5 per 100,000 persons in the general population25,26.
Use of the therapies described in patients with IBD has been associated with persistence of high-risk HPV infection through alteration of viral oncoproteins E6 and E7, which promote viral overexpression27. The most commonly implicated and best-documented HPV genotypes are HPV 16 and HPV 1827. In most cases, HPV infection in sexually active adults tends to resolve spontaneously (viral clearance)25,27. When infection persists, cytopathological changes may occur, ranging from viral warts to anal intraepithelial neoplasia, classified as low-grade squamous intraepithelial lesions (LSIL) or high-grade squamous intraepithelial lesions (HSIL)28. Low-grade dysplastic changes may regress or progress to high-grade dysplasia25-27. This process may ultimately lead to superficially invasive squamous cell carcinoma of the anal canal (SISCCA), which is initially superficial and asymptomatic but subsequently progresses to deeper tissue infiltration accompanied by symptoms29,30. Specific risk groups have been identified as having a higher incidence of anal squamous cell carcinoma. These groups have been classified as follows29-31:
Individuals living with HIV older than 35 years, with incidence rates up to 90 per 100,000.
Women older than 45 years with documented HPV 16 infection.
Individuals older than 45 years with receptive anal intercourse (unknown serological status).
Immunocompromised patients, including transplant recipients and those receiving corticosteroids or anti-TNF therapy, representing approximately 5.5% of the population31.
Hypotheses and underlying mechanisms
Persistence of high-risk HPV infection is a key factor in the development of anal cancer31. Immunocompromised patients are more susceptible to infections, and the use of anti-TNF agents has been associated with an increased risk of HPV infection30. Alterations in the viral oncoproteins E6 and E7 may also affect human defensins, which function as a protective system against HPV in perianal skin through surface proteins30,31. Development of dysplasia as a precursor lesion may be promoted by chronic inflammation attributable to IBD itself30.
Surveillance and prevention
The meta-analysis published by Clifford et al., together with the guidelines of the International Anal Neoplasia Society, suggests that patients with IBD, particularly those with CD26, should be included in screening programs in order to reduce the incidence of anal cancer. Primary prevention through HPV vaccination could mitigate this risk over several decades. However, ongoing screening and surveillance strategies remain necessary because most of the population was not vaccinated at an early age26,31.
Complementary surveillance strategies include the following26-31:
Liquid-based anal cytology: enables early detection of abnormal cells, analogous to cervical cytology.
Advanced genotyping: identifies high-risk HPV types, particularly types 16 and 18.
High-resolution anoscopy (HRA): enables rapid and safe identification and treatment of dysplastic lesions. This approach has reduced the incidence of anal cancer by approximately half in other high-risk populations, comparable to the reductions in cervical cancer incidence achieved through colposcopy.
High-resolution anoscopy technique
HRA is performed using a colposcope rather than a colonoscope in order to allow a detailed 360-degree examination of the anal transformation zone30. This area is located between the visible squamocolumnar junction and the dentate line. Topical agents such as 5% acetic acid and 5% Lugol’s solution are used to identify lesions. The specialist identifies low- and high-risk lesions, superficially invasive squamous cell carcinoma of the anal canal (SISCCA), or deeply infiltrative carcinoma32.
Lesion identification is based on several characteristic patterns:
Acetic acid uptake (flat or raised).
Surface pattern (granular or micropapillary).
Vascular patterns (mosaic and punctation).
Areas of abnormal metaplasia (lace-like or honeycomb pattern).
Lugol uptake (partial or negative in high-grade dysplasia).
These findings guide diagnosis and therapeutic decision-making32. Figure 2 illustrates representative findings observed in dysplastic changes associated with HPV infection, as well as elements commonly used in an HRA examination setting.
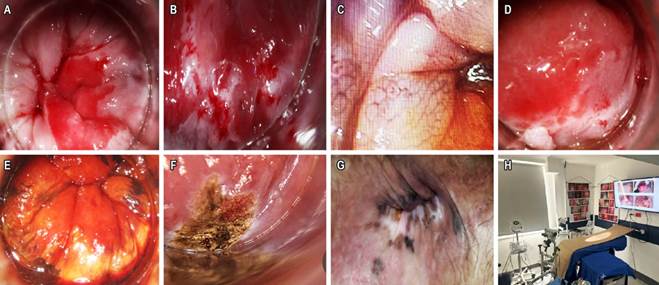
Figure 2 A. Dense acetowhite area: transformation zone with a clearly visible 360-degree squamocolumnar junction. B. High-grade dysplasia with lace-like metaplasia and coarse punctation observed at 15× magnification using microscopy. C. Coarse mosaic pattern at 15× magnification, consistent with high-grade dysplasia. D. LSIL-condyloma lesion and lace-like metaplastic area of anal intraepithelial neoplasia. E. Lugol-negative area corresponding to high-grade dysplasia requiring treatment. F. Electrocautery treatment of a high-grade dysplastic area in the HRA setting. G. Anoscopy includes assessment and magnification of the perianal region. In this case, pigmented lesions correspond to perianal HSIL (bowenoid papulosis). H. HRA examination setting. Images property of the authors.
Surveillance strategies such as liquid-based cytology, genotyping, and HRA are essential for prevention and early detection of precursor lesions and early-stage anal cancer, particularly in high-risk populations. These strategies may significantly reduce disease incidence, as demonstrated in other high-risk groups33.
Differential diagnoses
Diagnosis of ARC in patients with IBD receiving anti-TNF therapy requires careful assessment of the impact of chronic inflammation associated with IBD and the potential effects of anti-TNF therapy on both malignant and nonmalignant cells. Management of these patients typically requires a multidisciplinary team involving gastroenterologists, oncologists, and coloproctologists. Regular surveillance and a high index of suspicion are essential to detect and manage malignancies in this high-risk population in the following clinical scenarios:
Perianal abscess and fistula: common in IBD and may mimic CRC. Chronic perianal fistulas, particularly in patients with long-standing disease, should raise suspicion for malignancy34.
Infectious processes: opportunistic infections, including reactivation of latent infections such as tuberculosis and hepatitis B, may mimic malignancy, particularly in immunocompromised patients35.
CRC: chronic inflammation in IBD increases CRC risk, which may be further influenced by immunosuppressive therapies, although data regarding TNF antagonists remain inconclusive7,14,16.
Lymphoma: anti-TNF therapy has been associated with an increased risk of lymphoproliferative disorders, including lymphoma, particularly in patients receiving concomitant thiopurines14,16,35.
Nonmelanoma skin cancer: anti-TNF therapy is associated with an increased risk of nonmelanoma skin cancer. This possibility should be considered when evaluating unusual cutaneous lesions in the anorectal region7,8.
Anal squamous cell carcinoma: this malignancy may present as anorectal abscesses or fistulas and occurs more frequently in individuals with Crohn’s disease or chronic perianal disease34.
Management
Management of ARC in patients with IBD receiving anti-TNF therapy is complex, primarily due to the interaction between cancer risk and the immunosuppressive effects of these biological agents36,37. Anti-TNF therapy plays a fundamental role in the management of IBD because of its anti-inflammatory properties and its capacity to promote mucosal healing. However, its use in patients with a history of malignancy, including colorectal cancer, requires careful consideration. A study comparing the safety of anti-TNF agents with that of non-anti-TNF biologic therapies found no significant differences in cancer progression or recurrence. These findings suggest that anti-TNF therapy may be safely used in this context36-38. Recent data suggest that anti-TNF therapy may reduce the risk of CRC in patients with IBD, possibly due to its anti-inflammatory effects. In the study conducted by Alkhayyat et al.6, patients with IBD treated with anti-TNF agents were less likely to develop CRC compared with those not receiving these therapies (odds ratio [OR]: 0.69; 95% confidence interval [CI]: 0.66-0.73; p < 0.0001 for CD, and OR: 0.78; 95% CI: 0.73-0.83; p < 0.0001 for UC) Although this finding is specific to CRC, it underscores the importance of inflammation control in cancer risk management, which may also be relevant to ARC6.
The decision to use anti-TNF therapy should be made by a multidisciplinary team, taking into account disease severity and oncological status (Figure 3). Potential benefits and risks must be carefully weighed. Therapeutic drug monitoring and combined strategies (e.g., antibiotics or surgery) have also been shown to improve outcomes in fistulizing CD39,40.
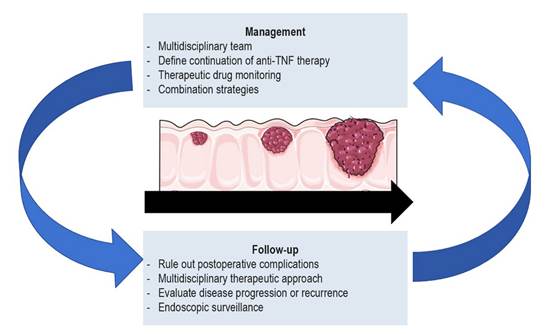
Figure 3 Considerations in the therapeutic approach and follow-up of anorectal cancer in relation to the use of tumor necrosis factor inhibitors in patients with inflammatory bowel disease. Image created using Servier Medical Art figures under their terms of use, based on: Boaz E, et al. Am Surg. 2023;89(6):2572-634; Billiet T, et al. Expert Opin Biol Ther. 2014;14(1):75-10136; Holmer AK, et al. Clin Gastroenterol Hepatol. 2023;21(6):1598-1606.e537; Waljee AK, et al. Lancet Gastroenterol Hepatol. 2020;5(3):276-8441; Lee KE, et al. Dis Colon Rectum. 2024;67(S1):S11-2542; Hammoudi N, et al. Dig Liver Dis. 2023;55(9):1280-743.
Evidence regarding anti-TNF therapy in patients with IBD remains limited. Achieving an appropriate balance between optimal IBD control, cancer risk, and the safety of anti-TNF therapy in patients with prior malignancy remains essential. Further research is required.
Recurrence
Research on recurrence of neoplastic disease in patients with IBD treated with anti-TNF therapy is clinically relevant, as it may inform therapeutic decision-making according to the current literature. A multicenter study conducted by Holmer et al. compared the safety of anti-TNF biologic agents with non-TNF inhibitor biologics in patients with IBD and active or recent malignancy. No differences in cancer recurrence were observed between the two groups, suggesting that anti-TNF therapy does not increase recurrence risk in this population37. Another study supports this finding. It evaluated the risk of new or recurrent cancer in patients with IBD and a prior history of malignancy treated with anti-TNF agents. The study concluded that anti-TNF therapy was not associated with an increased risk of cancer compared with other immunosuppressive treatments or absence of therapy44.
A review of available studies found no significant differences in cancer risk among patients with a prior history of malignancy who received anti-TNF therapy compared with those treated with nonbiologic disease-modifying therapies45. This meta-analysis further supports the conclusion that anti-TNF therapy is not associated with an increased risk of cancer recurrence.
A Danish cohort study similarly reported that anti-TNF therapy did not increase the risk of cancer recurrence or development of a new malignancy. No significant increase in risk was observed, with an adjusted hazard ratio (HR) of 0.82 (95% confidence interval [CI]: 0.61-1.11) for cancer recurrence or development of a new malignancy among patients receiving anti-TNF therapy41.
Overall, the medical literature suggests that use of anti-TNF therapy in patients with IBD and a history of malignancy does not substantially increase recurrence risk. These findings are consistent across multiple studies and meta-analyses, supporting the relative safety of TNF inhibitors in this context. Nevertheless, individualized clinical assessment remains essential, and therapeutic decisions should involve close collaboration with oncology specialists.
Complications
Concern persists regarding lymphoma risk, particularly when anti-TNF therapy is used in combination with thiopurines, which are a recognized risk factor for hepatosplenic T-cell lymphoma13. A systematic review found that anti-TNF therapy does not significantly increase the risk of postoperative complications in patients with IBD undergoing surgery42. This finding is particularly relevant for patients with ARC who may require surgical intervention. A multicenter study reported that anti-TNF therapy in patients with active or recently diagnosed cancer does not appear to increase the risk of cancer progression or recurrence37. This observation is clinically important for management of IBD in patients with a history of CRC, as it suggests that anti-TNF therapy may be used without significantly increasing the risk of cancer-related complications.
Overall, TNF inhibitors do not appear to significantly increase the risk of malignancy or postoperative complications, although variability may exist. Close monitoring and multidisciplinary management are recommended (Figure 3).
Prognosis
Prognosis represents a nuanced issue with several important considerations based on current clinical evidence. A study conducted at a French tertiary care center provides relevant data regarding the prognosis of IBD-associated CRC43. The study reported a median overall survival of 45 months for the entire cohort. Patients with metastatic disease had a poorer prognosis, with a median overall survival of 20.4 months, compared with patients presenting with localized tumors, who demonstrated a median overall survival of 74 months among those previously exposed to immunosuppressive therapy43. These findings suggest that prior exposure to immunosuppressive agents, including anti-TNF therapy, may be associated with improved prognosis in localized IBD-associated CRC.
A multicenter study found no significant differences in cancer progression or recurrence rates between anti-TNF and non-TNF biologic therapies in patients with IBD and active or recent malignancy37, indicating that anti-TNF therapy does not adversely affect cancer prognosis in this population37. A review evaluating patients with IBD treated with anti-TNF agents found no increased risk of malignancy, including CRC7. These findings support the conclusion that anti-TNF therapy does not negatively influence CRC prognosis in patients with IBD7. A study evaluating the risk of new or recurrent cancer in patients with IBD and prior malignancy found no significant differences in cancer risk between patients treated with anti-TNF agents and those not receiving anti-TNF therapy44. This observation suggests that anti-TNF therapy does not increase cancer recurrence risk, which represents a key determinant of prognosis in ARC44.
Conclusions
Evidence regarding TNF inhibitors and malignancy risk in patients with IBD may be extrapolated. Available evidence largely supports a protective effect for colorectal cancer. Diagnosis of ARC in patients with IBD potentially associated with anti-TNF therapy should rely on careful clinical judgment. Suspicion should be heightened in patients with long-standing anal or perianal lesions, HPV infection, concomitant immunomodulator therapy, chronic inflammation, and long disease duration. Pathophysiological mechanisms may involve alterations in T-cell function. Diagnosis relies primarily on HRA and histopathological evaluation due to the broad differential diagnosis and nonspecific clinical presentation. Management requires a multidisciplinary approach. Risk of complications and prognosis vary, with poorer outcomes observed in patients with disseminated disease. Although specific data regarding ARC remain limited, evidence from CRC and other malignancies suggests that anti-TNF therapy does not substantially modify cancer risk in patients with IBD. More robust studies are required to establish definitive conclusions. Evidence regarding the impact of anti-TNF therapy on anorectal cancer remains scarce, and no study has demonstrated either an increased or decreased risk of anorectal cancer attributable to anti-TNF therapy. Although anti-TNF therapy may influence CRC risk, data regarding its specific effect on anorectal cancer are lacking.

