











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Short bowel syndrome (SBS) is the leading cause of intestinal failure in childhood1. Among the surgical strategies used in its management, serial transverse enteroplasty (STEP), first described by Kim et al. in 20032, consists of lengthening the dilated intestine while preserving the mesentery through transverse divisions using an intestinal stapler and reducing the intestinal lumen diameter in a zigzag configuration (Figure 1). This technique has been shown to effectively reduce areas of stasis, optimize nutrient contact with the absorptive surface of the intestine, and improve intestinal motility; nevertheless, the medical literature has documented several complications associated with this procedure, including gastrointestinal bleeding, perianastomotic ulceration, and eosinophilic enterocolitis. These complications may affect clinical outcomes and require additional interventions for appropriate and timely management3.
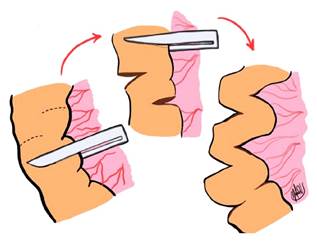
Figure 1 STEP technique. Prepared by: Natalia Velasquez. Adapted from: Almau H, et al. Rev Venez Cir. 2015;68(1):21-44.
Case report
An 11-year-old female patient with a history of gastroschisis repaired at birth and persistent intestinal obstruction is presented. At 31 days of life, distal ileal atresia with absence of the ileocecal valve was identified. A resection of 16 cm of terminal ileum and a jejunocolic anastomosis were performed. Obstructive symptoms persisted, with progressive intestinal dilation documented on contrast intestinal transit studies. At 140 days of life, the patient underwent a second surgical procedure. The small intestine measured 66 cm in length, with the distal 30 cm markedly dilated. A patent jejunocolic anastomosis and a colon measuring 18 cm were identified. Intestinal lengthening using the STEP technique was performed, together with gastrostomy and tube jejunostomy placement. The patient showed favorable clinical progression, with adequate intestinal adaptation and no complications. She was discharged at 7 months and 19 days of age with a body weight of 6.2 kg, receiving hydrolyzed formula and without the need for parenteral nutrition.
Ten years later, the patient was readmitted with a one-year history of disabling abdominal pain, melena, abdominal distension, and weight loss, without increased stool output and with a tendency toward constipation. Severe microcytic hypochromic anemia was identified, with normal red cell mass, requiring transfusion without complications. Colonoscopy revealed a 1.5 cm jejunocolic anastomotic ulcer associated with jejunal stenosis. Exploratory laparotomy was performed, including resection of 10 cm of the affected segment and creation of a new anastomosis. Initial postoperative progression was favorable. The patient tolerated the nutritional regimen prescribed by the clinical nutrition team. Parenteral nutrition (PN) was successfully discontinued. Adequate weight gain and stable stool output were observed, with no clinical or hemodynamic deterioration. However, symptom recurrence developed within a few months.
A repeat colonoscopy revealed extensive perianastomotic ulceration and friable mucosa at the STEP suture lines. Histopathological analysis demonstrated chronic active enteritis with neutrophilic and eosinophilic infiltration. Pharmacological management included a two-week course of prednisone, mesalamine, cholestyramine, azathioprine, a proton pump inhibitor (PPI), a prokinetic agent, and cycles of intestinal decontamination. An adequate clinical response was not achieved. Due to persistent symptoms and previously described findings, a new surgical intervention was indicated, including intraoperative endoscopic evaluation.
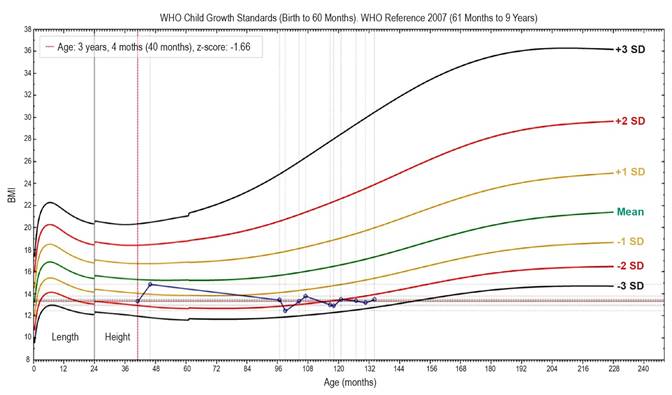
Intraoperative colonoscopy demonstrated an extensive ulcer and erosive colitis at the mechanical suture line, associated with jejunal stenosis and mesenteric thinning between the STEP segment and the jejunocolic anastomosis (Figure 2). Resection of the ulcerated segment was performed, including the portion previously treated with STEP, followed by a new jejunocolic anastomosis. Final intestinal length was 76 cm of small bowel and 95 cm of colon. Postoperative evolution was favorable, with complete resolution of symptoms. At the most recent follow-up, two months after the procedure, the patient was in good clinical condition, without the need for parenteral nutrition and without significant weight loss. Adequate tolerance to fractionated oral feeding was observed. The diet included restriction of simple carbohydrates and saturated fats, a high content of soluble fiber, and supplementation with an oligomeric formula to meet energy and macronutrient requirements. Current treatment includes ferrous sulfate, loperamide, calcium carbonate, vitamin D, and cycles of intestinal decontamination with rifaximin. During recent hospitalizations, progressive increases in weight and height were observed. Nevertheless, the patient continues to present growth delay, with body mass index (BMI) consistent with underweight status and depletion of energy reserves for age according to World Health Organization (WHO) indicators (Figure 3). Ongoing follow-up is being conducted by pediatric endocrinology.
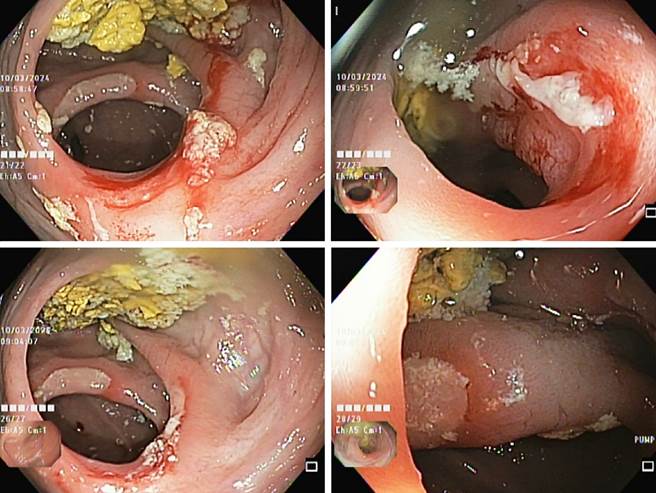
Figure 2 Colonoscopy showing multiple linear perianastomotic ulcerations covered by fibrin, without active bleeding. Images property of the authors.
Discussion
Intestinal failure (IF) is defined as a reduction in functional intestinal mass below the threshold required to sustain life, resulting in dependence on parenteral support for at least 60 days5. According to the RESTORE registry, in Latin America the mortality rate associated with IF is 7.7%, and the rehabilitation rate reaches 53% at five years6. Short bowel syndrome (SBS) is the leading cause of IF and represents a condition that requires timely multidisciplinary management. Initial management includes maintenance of acid-base balance and fluid and electrolyte homeostasis, initiation of nutritional support, and pharmacological therapy with antisecretory agents (H2 receptor antagonists, PPIs, loperamide), as well as other medications such as cholestyramine or teduglutide. These interventions aim to promote intestinal adaptation, improve intestinal motility and transit, and reduce dependence on parenteral nutrition7. However, when medical management is unsuccessful, surgical alternatives should be considered, including stoma closure and gastrointestinal tract reconstruction, enteroplasty procedures, intestinal transit-slowing techniques, or intestinal lengthening procedures8.
The group of surgical procedures developed to facilitate transition to enteral autonomy is known as autologous intestinal reconstructive surgery (AIR). The AIR procedures most commonly used in clinical practice include serial transverse enteroplasty (STEP), longitudinal intestinal lengthening procedure (LILT), and tapering enteroplasty (TPE)9,10. The STEP technique (Figure 1) has demonstrated reduction of areas of stasis, increased contact between nutrients and the absorptive intestinal surface, and improvement in intestinal motility2,11. According to a Markov decision analysis, this procedure improves long-term survival in pediatric patients with SBS, increasing rates of enteral autonomy and reducing the need for intestinal transplantation12.
In the experimental study conducted by Kim et al. in 2003 using a porcine model, a 64% increase in final intestinal length was observed. Six weeks after the procedure, the animals demonstrated adequate intestinal adaptation, with weight gain and no associated complications2. Similarly, a study conducted by Patrick et al. in 2005 evaluated the surgical and nutritional outcomes of STEP in infants and concluded that it is a technically straightforward intestinal lengthening procedure with favorable results in terms of growth and nutritional status13. Additional advantages of this surgical technique include the absence of a requirement for additional anastomoses and preservation of mesenteric integrity. Moreover, the procedure effectively achieves intestinal lengthening, which depends on both the degree of preexisting dilation and the caliber of the newly created intestinal channel.
However, the procedure may be associated with complications such as gastrointestinal (GI) bleeding, perianastomotic ulceration, and eosinophilic enterocolitis3. A demographic statistical analysis conducted at the Center for Advanced Intestinal Rehabilitation (CAIR) in Boston included follow-up of 296 patients, of whom 23 underwent STEP surgery, with a median age of 4.5 months. Among these patients, 3 (13%) developed GI bleeding between 5 and 30 weeks after surgery, requiring red blood cell transfusion. In addition, multiple endoscopic evaluations identified staple-line ulceration in 2 patients, which stabilized with bowel rest, and eosinophilic enterocolitis in 1 patient, which responded to treatment with luminal steroids. No technical factors related to the surgical procedure were identified as contributing to these complications3.
Similarly, a retrospective study conducted in Finland compared pediatric patients with SBS who underwent AIR procedures with those who received conservative management. The results demonstrated that the incidence of perianastomotic ulcerations and the presence of pathological endoscopic findings were similar in both groups. These findings suggest that such alterations are more likely a consequence of SBS itself rather than of the AIR surgical procedure14. Thus, available evidence indicates that complications are primarily associated with the underlying intestinal condition rather than the surgical intervention.
The available literature on long-term complications following the STEP procedure remains limited both globally and in Colombia. Historically, insufficient knowledge regarding IF and its therapeutic alternatives has hindered long-term follow-up. However, advances in the field have significantly improved survival through timely management strategies. Patients with IF who undergo AIR techniques require long-term follow-up by a multidisciplinary team, as complications may develop weeks or even years after the procedure. Endoscopic surveillance represents a key tool for early detection.
In the clinical case presented, the STEP procedure promoted intestinal adaptation during the neonatal period. Nevertheless, after ten years of follow-up, the patient developed severe ulceration and stenosis. Intraoperative surgical and endoscopic findings were essential for accurate identification of the affected segments, allowing preservation of the greatest possible length of viable intestine.
From a multidisciplinary perspective, the previously described anemia was considered in the context of the patient’s clinical history and the absence of the ileocecal valve. A potential impairment in vitamin B12 absorption was considered, as this process depends on intrinsic factor and occurs primarily in the terminal ileum15. However, the morphological characteristics of the anemia (microcytic, hypochromic anemia with normal red cell mass), together with normal serum vitamin B12 levels, allowed exclusion of megaloblastic anemia. Evaluation of iron kinetic parameters confirmed the diagnosis of iron deficiency anemia.
Patients with chronic intestinal failure present impaired nutrient absorption, which negatively affects the GH-IGF-1 axis. This alteration impacts growth and development secondary to growth hormone deficiency or resistance16. For this reason, the patient remains under follow-up by pediatric endocrinology to evaluate the potential benefit of adjunctive growth hormone therapy.
Finally, in patients with SBS, it is essential to ensure “volume-for-volume” replacement of gastrointestinal losses in order to prevent complications such as hypovolemia, hydroelectrolytic disturbances, acute kidney injury, and splanchnic hypoperfusion17. Enteric losses may rapidly exceed the adaptive capacity of the kidneys, leading to extracellular volume depletion. Omission or inadequate replacement of these components may precipitate metabolic disturbances, hinder intestinal adaptation, prolong dependence on parenteral nutrition, and increase morbidity and mortality17,18.
As evidence regarding long-term outcomes following STEP surgery continues to expand, further studies are needed to better understand risk factors associated with complications and to optimize postoperative management strategies.
Conclusion
Short bowel syndrome, as the most frequent cause of intestinal failure in the pediatric population, represents a complex condition that requires interdisciplinary management and therapeutic strategies aimed at promoting intestinal adaptation. Although the STEP technique provides multiple advantages in terms of intestinal function and long-term quality of life, late complications may occur. Continuous clinical and endoscopic follow-up is therefore strongly recommended. In addition, the incorporation of intraoperative surgical and endoscopic tools allows precise identification of these complications and supports decision-making aimed at achieving the best possible prognosis for the patient.

