











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Portal hypertensive enteropathy (PHE) is an uncommon condition defined by the presence of pathological changes and mucosal abnormalities in the small intestine of patients with portal hypertension (PH)1 Case series report a prevalence of approximately 40%-96.8% among patients with liver cirrhosis and PH2. Based on these studies, several risk factors have been identified, including the presence of large esophageal varices, portal hypertensive gastropathy and colopathy, Child-Pugh class (B or C), prior history of variceal ligation or sclerotherapy, elastography values, and tomographic findings suggestive of portal hypertension, particularly portosystemic shunts 3. The available literature focuses almost exclusively on cases of PHE in cirrhotic patients; the present report describes a 35-year-old male with non-cirrhotic PH secondary to chronic portal vein thrombosis who presented with gastrointestinal bleeding and findings suggestive of PHE on video capsule endoscopy.
Case description
A 35-year-old male with a history of portal vein thrombosis with signs of cavernous transformation diagnosed by computed tomography angiography since childhood due to omphalitis was evaluated. The patient underwent splenectomy at 21 years of age for hypersplenism. Thrombophilia testing was negative, and liver elastography (FibroScan) showed a value of 5.2 kPa. He had experienced multiple previous episodes of variceal upper gastrointestinal bleeding since the age of 12, treated with endoscopic band ligation and sclerotherapy. He had also received anticoagulation therapy with warfarin for thrombosis, with the last dose administered two days prior to admission. The patient was admitted to the emergency department with hematochezia and generalized weakness. He was hemodynamically stable on admission, and digital rectal examination was positive for hematochezia. Laboratory tests revealed mild normocytic, normochromic anemia with hemoglobin of 12.6 g/dL, platelet count of 217 × 10³/μL, leukocyte count of 14.1 × 10³/μL, and an international normalized ratio (INR) of 1.78. The remaining biochemical and liver profile parameters were within normal limits. Abdominal ultrasound demonstrated dilation of the portal vein with multiple collateral vessels, no signs of cirrhosis, and no free fluid.
Treatment with octreotide was initiated. Upper gastrointestinal endoscopy revealed moderate portal hypertensive gastropathy and small esophageal varices without signs of recent bleeding. Given the presence of gastrointestinal bleeding, colonoscopy was performed, which showed no evidence of recent bleeding or residual blood. Mild erythema was observed in several segments of the colon, findings compatible with portal hypertensive colopathy but insufficient to explain the previously documented hematochezia. Video capsule endoscopy (VCE) was subsequently performed, identifying multiple red spots (Yano-Yamamoto type 1a) in the duodenum, jejunum, and ileum (Figure 1), as well as an angiodysplasia-like lesion (Yano-Yamamoto type 1b) measuring 2-4 mm in length without signs of active bleeding in the proximal ileum (Figure 2). Areas of hyperemia measuring 2-3 mm were also detected between the distal jejunum and proximal ileum (Figure 3).

Figure 1 Vascular lesions: red spots in the distal jejunum (Yano-Yamamoto type 1a). Images property of the authors.
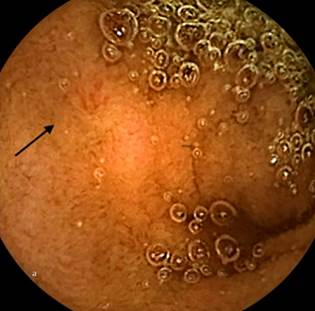
Figure 2 Vascular lesion: angiodysplasia-like lesion in the proximal ileum (Yano-Yamamoto type 1b). Image property of the authors.
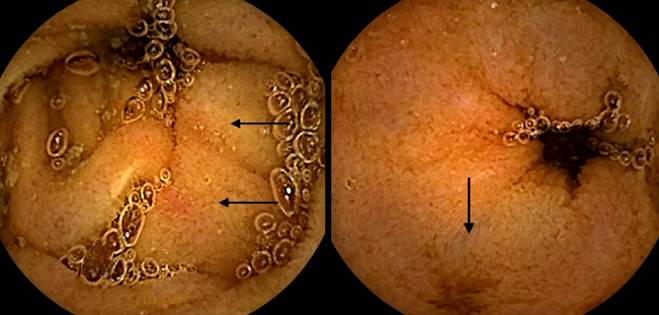
Figure 3 Nonvascular lesions: areas of mucosal hyperemia between the distal jejunum and proximal ileum. Images property of the authors.
The patient completed five days of octreotide therapy at an initial dose of 50 μg as an intravenous bolus followed by continuous infusion at 50 μg/hour. After diagnosis, the patient was discharged on carvedilol 12.5 mg/day. No additional episodes of gastrointestinal bleeding were observed during one year of follow-up.
Discussion
Findings associated with PHE are usually classified as vascular or nonvascular. Vascular findings include red spots, telangiectasias, angiodysplasia-like lesions, and varices. Nonvascular findings, also described as inflammatory abnormalities, include edema, hyperemia, granularity, and friability4,5. Vascular lesions are more prevalent than nonvascular lesions6. Available case series report angiectasias in 24.3%-67% of patients, red spots in 16.6%-62.2%, inflammatory lesions in 5.6%-41.9%, varices less frequently in 6.2%-16.1%, and active bleeding in 5.5%-17.8% of patients with PHE7. Other rare findings include pedunculated or sessile protrusions, either solitary or multiple, that may mimic polyps2,6. Vascular lesions, including angiectasias, red spots, and varices, are usually responsible for overt gastrointestinal bleeding2. In contrast, nonvascular or inflammatory lesions are more nonspecific and appear to carry a lower risk of bleeding. Both types of endoscopic findings may also be observed in other conditions, including inflammatory bowel disease, celiac disease, arteriovenous malformations, radiation enteritis, hereditary hemorrhagic telangiectasia, and familial adenomatous polyposis.
Although histopathology may assist in the evaluation of nonvascular lesions, imaging techniques such as computed tomography3 and transient elastography may help determine the likelihood of portal hypertension and its severity8. Diagnosis should always be established with a high index of suspicion in conjunction with clinical and endoscopic findings. In the present case, mucosal hyperemia, multiple red spots, and angiodysplasia-like lesions were identified in a patient with portal hypertension and additional risk factors. These findings supported the diagnosis of PHE.
Currently, no clinical guidelines are available for the management of symptomatic PHE. The usefulness of balloon-assisted enteroscopy has been described, including therapeutic interventions such as argon plasma coagulation, hemoclip placement, and sclerotherapy. Interventional radiology procedures, including transjugular intrahepatic portosystemic shunt (TIPS) placement or percutaneous embolization, as well as surgical management, have also been reported. Small studies have suggested potential benefits of nonselective β-blockers, somatostatin, and thalidomide in this condition6,9. In the most recent Baveno VII consensus, regarding the use of β-blockers in patients with portal hypertension-related bleeding due to portal vein thrombosis with cavernous transformation, insufficient evidence was identified to support their use for primary or secondary prophylaxis. Therefore, recommendations for patients with cirrhosis should be followed10. The patient described in this report was initially treated with octreotide, followed by nonselective β-blockers. No evidence of gastrointestinal bleeding was observed during one year of follow-up. This case is noteworthy because most published reports involve cirrhotic patients1,3,7, whereas the present case involves non-cirrhotic portal hypertension secondary to portal vein thrombosis in a patient with risk factors for developing PHE.
Conclusion
Portal hypertensive enteropathy is an uncommon and likely underdiagnosed condition. It should be suspected in patients with portal hypertension, whether cirrhotic or non-cirrhotic, who present with gastrointestinal bleeding or anemia, in order to avoid delays in the use of video capsule endoscopy. Management is not standardized; however, octreotide and nonselective β-blockers may represent a therapeutic option.

