











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Choledochal cysts constitute a rare congenital or acquired anomaly of the hepatobiliary system, characterized by cystic or diverticular dilatation of the biliary tract1. Their etiology is primarily associated with an anomalous pancreaticobiliary junction, which facilitates reflux of pancreatic juice into the biliary tree1. Although traditionally considered a pediatric condition, choledochal cysts may also present in adulthood, often with less specific symptoms than those observed in children1.
The Todani classification divides choledochal cysts into five main types, with type I being the most common2. Within this group, subtype Ib is defined by focal or segmental dilatation of the common hepatic duct or the distal common bile duct3. The complete classification and its subtypes are summarized in Figure 1.

Figure 1 Todani classification of choledochal cysts. Adapted from: Brown ZJ, et al. HPB. 2023;25(1):14-254.
The most frequent choledochal cyst subtypes are type I (64%) and type IV (22%), although some series have reported substantial variability, with prevalence rates as high as 88% for type I in one study and 48% for type V in another5. Regarding age distribution, type I cysts occur more commonly in children, whereas type IV cysts are more prevalent in adults. Together, types I and IV account for approximately 90% of all cases in both adult and pediatric populations4.
Among the available noninvasive imaging modalities, magnetic resonance cholangiopancreatography (MRCP) is the reference standard because it allows precise characterization of biliary anatomy and accurate preoperative classification of cysts6, with reported sensitivities ranging from 81% to 100% and specificities up to 100%7. Abdominal ultrasonography remains the initial screening modality, with variable sensitivity ranging from 33% to 90%8, whereas computed tomography is primarily used to evaluate complications and intrahepatic extension, providing intermediate diagnostic accuracy8. Other modalities, such as endoscopic ultrasonography, are useful for detecting small tumors and differentiating choledochoceles from other lesions9. Direct cholangiography through endoscopic retrograde cholangiopancreatography (ERCP) or percutaneous transhepatic cholangiography (PTC), previously considered the reference standard, is now reserved for selected cases due to its invasive nature and higher risk of complications4.
The clinical relevance of choledochal cysts lies in their potential for malignant transformation, particularly in Todani types I, IV, and V. In Western adult populations, the most recent systematic review reports an overall malignancy rate of 10.9%, with cholangiocarcinoma being the predominant histologic type10. The mean age at diagnosis of malignancy ranges from 36.8 to 57.2 years, and adults exhibit higher rates of complications and cancer compared with pediatric populations11.
Regarding subtype-specific risk, the estimated malignancy risk ranges from 6% to 14% for type I, 6% to 30% for type IV, and 7% to 15% for type V, whereas types II and III show considerably lower incidences (<5% and <1%, respectively)7. These findings support the indication for complete cyst resection, which reduces-although does not eliminate-the risk of neoplastic transformation, in contrast to internal drainage procedures, which have been associated with malignant recurrence in up to 11% of cases7. In this context, complete cyst excision serves not only a symptomatic purpose but also represents a fundamental strategy to interrupt progression toward malignant disease10.
Reconstruction of biliary continuity after resection is typically performed using Roux-en-Y hepaticojejunostomy, which is considered the technique of choice due to its technical reliability and favorable clinical outcomes. By separating the bilioenteric anastomosis from the duodenal pathway, this approach reduces reflux risk and ensures stable long-term drainage. Although hepaticoduodenostomy may shorten operative time, Roux-en-Y hepaticojejunostomy is associated with lower rates of reflux and fewer reinterventions, achieving patency rates exceeding 85%-90% in experienced hands5,7. The laparoscopic approach has gained acceptance because of its perioperative advantages. However, open surgery remains indispensable in complex scenarios in which maneuvers such as Kocher and Cattell-Braasch facilitate optimal anatomical exposure2,3.
The objective of this report is to describe the surgical management of a type Ib choledochal cyst in an adult patient, with particular emphasis on the reconstruction technique using a subcutaneous jejunal loop5. This strategy provides simple, safe, and permanent access to the anastomosis, thereby facilitating future diagnostic or therapeutic interventions (such as dilation of anastomotic strictures) and offering particular advantages in younger patients by reducing the need for major reinterventions.
Case presentation
A 36-year-old female patient with a history of two full-term pregnancies and no known comorbidities presented with recurrent right upper quadrant pain of approximately six months’ duration. Endoscopic ultrasonography identified fusiform cystic dilatation of the distal common bile duct, consistent with a type Ib choledochal cyst according to the Todani classification4, as well as gallstones within the gallbladder, establishing a diagnosis of concomitant cholelithiasis. Imaging evaluation confirmed the anatomy and intrapancreatic extension of the cyst.
Given the diagnosis of symptomatic cholelithiasis and type Ib choledochal cyst, a two-stage surgical approach was planned. Initially, laparoscopic cholecystectomy was performed without complications, followed by an uneventful postoperative recovery. Because biliary surgery in a recently inflamed setting increases the risk of technical and anastomotic complications7, cyst resection was deferred to an interval (“cold”) phase, as reduced tissue inflammation facilitates safer dissection and decreases postoperative morbidity4. Accordingly, 45 days after cholecystectomy, complete cyst excision and biliary reconstruction were performed via laparotomy with Roux-en-Y hepaticojejunostomy. The operative field was exposed, and the dilated choledochal cyst was identified (Figure 2).

Figure 2 Intraoperative view of the choledochal cyst in situ (Todani IB). The white arrow indicates the dilated cyst, and the blue arrow indicates the common bile duct. Image property of the authors.
To achieve adequate exposure and mobilization of the duodenum and pancreatic head, thereby facilitating complete resection of the distal portion of the cyst, the Kocher and Cattell-Braasch maneuvers were performed. The Kocher maneuver involves incising the peritoneum lateral to the duodenum at the level of its second portion and carefully dissecting the posterior avascular plane. This allows medial mobilization of the duodenum and pancreatic head, exposing the retroperitoneum, inferior vena cava, and right renal pedicle, thereby safely expanding the surgical view of the distal biliary tract2. The Cattell-Braasch maneuver, or right medial visceral rotation, complements the Kocher maneuver by mobilizing the hepatic flexure of the colon and the small intestine toward the midline. This provides wide exposure of the third and fourth portions of the duodenum, as well as retroperitoneal structures such as the right iliac vessels and ureter, thereby optimizing surgical access to the biliary tract and reducing the risk of inadvertent injury3. Intraoperative cholangiography was performed to visualize the proximal biliary tree anatomy and confirm the extent of the cyst (Figure 3).
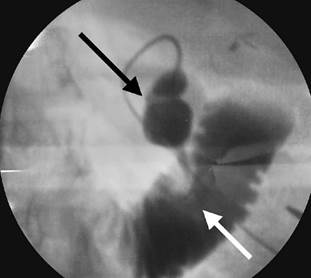
Figure 3 Intraoperative cholangiography. The black arrow indicates the choledochal cyst (fusiform dilatation), and the white arrow indicates the second portion of the duodenum. Image property of the authors.
Complete cyst excision was performed, including its intrapancreatic portion, as shown in the surgical specimen in Figures 4 and 5.

Figure 4 Gross resection specimen of the choledochal cyst. Fusiform dilatation of the extrahepatic biliary tract measuring 3.5 × 2.0 cm is observed. Image property of the authors.

Figure 5 Gross resection specimen of the choledochal cyst opened longitudinally. The cystic cavity and the characteristics of its thickened internal surface, with papillary folds, are visualized. Image property of the authors.
Reconstruction of biliary-enteric continuity was performed using Roux-en-Y hepaticojejunostomy (Figure 6). A defunctionalized jejunal limb was created. A termino-lateral anastomosis was constructed between the distal end of the jejunal limb and the proximal biliary tract (common hepatic duct and left hepatic duct), ensuring the absence of tension along the suture line. An enteroenterostomy (jejunojejunostomy, Y-limb) was created approximately 50-60 cm distal to the hepaticojejunostomy. As a technical particularity, a subcutaneous jejunal loop was fashioned by fixing the blind end of the Roux jejunal limb to the abdominal wall within the subcutaneous tissue.
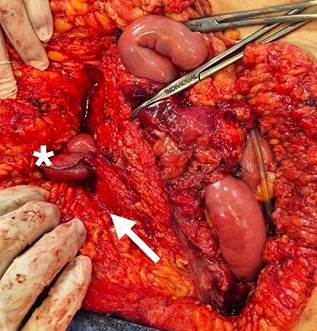
Figure 6 Preparation of the subcutaneous jejunal access loop: intraoperative view of the open abdominal cavity showing the jejunal limb that will be prepared as a permanent subcutaneous access route. The asterisk (*) indicates the defunctionalized jejunal limb, and the white arrow indicates the skin flap where the subcutaneous pocket will be created to accommodate the end of the loop. Image property of the authors.
The postoperative course was uneventful, with adequate oral tolerance and restoration of bowel function. The patient was discharged in good clinical condition. The pathology report confirmed the diagnosis of a type Ib choledochal cyst with areas of fibrosis associated with chronic inflammatory changes, as well as glandular hyperplasia of the lining with associated cholesterosis, without evidence of malignancy.
Discussion
Choledochal cysts are an uncommon entity in the adult population1. Clinical presentation is often nonspecific, which may delay early diagnosis. However, the risk of malignant transformation to cholangiocarcinoma represents one of the principal concerns, particularly in type I and type V cysts7, thereby supporting the indication for complete cyst excision once the diagnosis has been established7.
The standard treatment for type I choledochal cysts consists of complete cyst excision followed by biliary-enteric reconstruction using Roux-en-Y hepaticojejunostomy4,7. This technique is the most widely used worldwide due to its safety and durability in the management of benign biliary tract obstruction4, although it is not free of complications. The most clinically relevant long-term complication is anastomotic stricture, with an incidence of approximately 6.9% in follow-up periods ranging from 2 to 13 years and a cumulative prevalence that may reach up to 25% in some series11.
Resection should be as complete as possible, particularly in the distal intrapancreatic portion, in order to reduce the risk of persistent or recurrent malignant transformation10. In the present case, an open surgical approach was selected. Although the laparoscopic approach has gained increasing acceptance in recent years12, the technical complexity associated with resection of the intrapancreatic segment and the need to construct a subcutaneous jejunal loop justified the use of a conventional open approach. The Kocher and Cattell-Braasch maneuvers were essential to achieve safe exposure of the duodenum and right retroperitoneum, thereby enabling complete resection of the distal portion of the cyst2,3.
A technically relevant aspect of this case is the creation of a subcutaneous jejunal loop (or modified Praderi loop)13, which consists of fixing the end of the Roux limb to the abdominal wall within the subcutaneous tissue13. Its principal advantage is the provision of simple and permanent access to the hepaticojejunostomy, thereby facilitating subsequent endoscopic evaluation or intervention, such as dilation of anastomotic strictures5.
The literature addressing this technique and its variants remains limited and is based primarily on small series or isolated reports, without prospective studies or large cohort analyses. This limitation makes it difficult to establish its precise clinical impact and long-term applicability. Nevertheless, the available data support its potential usefulness. One prospective study reported successful endoscopic access to the anastomosis in 26 of 28 attempts (93%), although without subcutaneous positioning of the loop14. Another series evaluating intrahepatic lithiasis reported successful outcomes in all 55 procedures performed11. Clinically, resolution of anastomotic strictures was documented in three patients through endoscopic dilation and clearance, with normalization of liver function tests and no need for revision surgery14. Similarly, in another cohort, complete stone extraction was achieved in 21 of 28 patients (75%) using the access loop11. These findings suggest that this strategy enables repeated, minimally invasive interventions with low morbidity and without the need for general anesthesia, thereby representing a valuable option for patients at increased risk of anastomotic stricture or recurrent lithiasis.
Although no consensus exists regarding the routine use of stents or access loops in all hepaticojejunostomies, their use is considered appropriate in selected cases, particularly in younger patients with a higher probability of requiring long-term access to the anastomosis.
Postoperative complications of Roux-en-Y hepaticojejunostomy include biliary fistula, bilioma, cholangitis, and, in the long term, anastomotic stricture11. In this context, the subcutaneous jejunal loop provides a less invasive alternative than relaparotomy for the management of certain complications5.
The decision to perform surgery in two stages, with initial cholecystectomy followed by delayed cyst excision, was intended to resolve gallstone disease first and allow resolution of acute inflammation prior to definitive resection. Although simultaneous resection of the cyst and gallbladder represents a valid strategy, the selected approach aimed to optimize surgical safety and reduce morbidity.
Ultimately, management of choledochal cysts in adults requires a high index of diagnostic suspicion and timely surgical treatment because of the risk of malignancy10. Complete excision with Roux-en-Y reconstruction remains the standard of care. Incorporation of a subcutaneous jejunal loop, as described in this case, represents a useful technical modification for long-term follow-up and minimally invasive management of anastomotic complications5.
This case underscores the importance of combining a comprehensive surgical approach with reconstructive techniques adapted to the complexity of this uncommon but clinically significant condition.
Conclusion
Management of type Ib choledochal cysts in adults requires complete excision combined with safe biliary-enteric reconstruction. In the present case, the combination of Roux-en-Y hepaticojejunostomy with incorporation of a subcutaneous jejunal loop proved to be an effective strategy that not only mitigates oncologic risk but also provides permanent access for potential future interventions. This experience highlights the value of adapting innovative reconstructive techniques to complex clinical scenarios, offering durable and less invasive solutions for late complications, and reinforces the importance of a comprehensive surgical approach in this uncommon yet clinically relevant entity.

