











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
The gastrointestinal (GI) tract comprises the esophagus, stomach, small intestine, colon, and rectum. Benign and malignant tumors may develop along this anatomical continuum. In the United States, an estimated 26,500 new cases of gastric cancer (GC) were diagnosed in 2023, with 11,130 deaths attributable to the disease1. The five-year survival rate is 32%, reflecting that fewer than 25% of cases are detected at early stages2. In Colombia, according to Globocan 2022 data, approximately 8,938 new cases of GC are reported annually. This positions GC as the fourth most frequent malignancy (7.6%) and the leading cause of cancer-related mortality, with 6,901 deaths per year (12.2%)3.
Several risk factors have been identified as contributors to GC development. These include Helicobacter pylori infection, tobacco use, high dietary salt intake, a family history of gastric cancer, and geographic or ethnic factors4. Of particular concern is the increasing incidence of early-onset GC, defined as occurring in individuals younger than 50 years, especially among those born between 1980 and 1994. In this population, the incidence rate is twice that observed in individuals born in the 1950s5. Early-onset GC is associated with more aggressive biological features, including poorly differentiated tumors, diffuse histological subtype, and the presence of signet ring cells. Distinct genomic alterations have also been identified, contributing to an unfavorable prognosis6-8.
Clinically, GC may present with nonspecific symptoms such as dyspepsia, loss of appetite, unintentional weight loss, and abdominal pain6. Upper gastrointestinal endoscopy is the most effective diagnostic tool for both screening and surveillance in patients at high risk of GC. It allows direct visualization of the gastric mucosa, identification of suspicious lesions, and biopsy sampling for histopathological analysis. Endoscopic and histological evaluation are essential for accurate staging, risk stratification, and decision-making regarding the need for and frequency of follow-up2.
Gastric cancer is a clinically and biologically heterogeneous entity. Traditionally, it has been classified according to the Lauren classification into two main subtypes: intestinal and diffuse. The intestinal subtype is characterized by well-formed glandular structures. In contrast, the diffuse subtype is defined by poorly cohesive and infiltrative tumor cells, often exhibiting signet ring cell morphology. Mixed forms combining both patterns also exist. These are associated with a poorer prognosis because of their aggressive biological behavior and dual dissemination pattern. Although additional histological classifications have been proposed, their practical utility for guiding treatment remains limited (Table 1)9.
Table 1 Lauren Classification (1965)
| Subtype | Histological characteristics | Dissemination | Prognosis |
|---|---|---|---|
| Intestinal | Well-differentiated glandular or papillary structures | Hematogenous | Intermediate |
| Diffuse | Poorly cohesive, infiltrative cells; signet ring cells may be present | Peritoneal | Unfavorable |
| Mixed | Combined intestinal and diffuse components | Hematogenous + peritoneal + lymphatic | Worse than the above |
| Indeterminate | Does not clearly fit other subtypes | Variable | Variable |
Table prepared by the authors.
Mixed adenocarcinoma is an uncommon but clinically relevant subtype. Reported relative frequency ranges from 6% to 22%. These tumors exhibit greater aggressiveness than those composed of a single histological component10.
The present report describes a clinical case that challenges traditional paradigms of tumor classification and biological behavior. The lesion consists of a gastric polyp that could easily be overlooked during routine endoscopic evaluation. However, histopathological analysis revealed a poorly differentiated mixed gastric adenocarcinoma, histological grade 3, classified as Borrmann type 1 (polypoid), with invasion of the lamina propria but a tumor-free base. This finding is paradoxical given the high biological aggressiveness of the tumor. Due to its rarity and complexity, this case highlights the importance of maintaining a high index of clinical suspicion when evaluating apparently benign lesions. It also raises questions regarding the progression and behavior of mixed adenocarcinomas at early stages.
Case presentation
A 55-year-old male patient with a medical history notable for exposure to biomass smoke and cigarette consumption presented with a long-standing clinical course characterized by persistent dyspepsia, abdominal distension, and unintentional weight loss. Symptoms did not improve with antispasmodics, H2 receptor blockers, or proton pump inhibitors. For this reason, the patient was referred from the outpatient clinic for upper gastrointestinal endoscopy as part of the complementary diagnostic workup.
During the endoscopic procedure, a multipolypoid lesion was identified in the antrum, with no macroscopic features suggestive of malignancy (Figure 1). Polypectomy was successfully performed, and the specimen was submitted for histopathological examination to establish a definitive diagnosis (Figure 2).


Figure 2 Polypectomy specimen of a light-brown multipolypoid lesion measuring 3 × 5 cm and 3 × 2 cm. Image property of the authors.
Histopathological analysis demonstrated a poorly differentiated mixed intestinal and diffuse-type adenocarcinoma, histological grade 3, Borrmann type 1 (polypoid), with invasion of the lamina propria, absence of lymphovascular invasion, and a tumor-free base of the lesion.
Based on the endoscopic and histopathological findings, the polypectomy was considered to have been performed with curative intent, as the lesion met criteria for gastric tumors smaller than 2 cm that do not penetrate beyond the submucosa and show no evidence of lymphovascular invasion.
Discussion
A review of the literature indicates that risk factors for GC can be grouped into six major categories, reflecting the complexity of its etiology (Figure 3). First, infectious factors are particularly relevant, especially H. pylori infection, classified as a Group 1 carcinogen by the World Health Organization (WHO) and responsible for up to 75% of cases. Epstein-Barr virus infection has also been associated with 5%-10% of cases6. Second, environmental and lifestyle factors play a significant role, including high-salt diets, obesity, gastroesophageal reflux, tobacco use, alcohol consumption, and low socioeconomic status. Third, acquired genetic and epigenetic alterations have been identified, such as chromosomal instability, copy number variations, and aberrant DNA methylation. The fourth category includes hereditary factors, with germline mutations in genes such as CDH1, BRCA1/2, ATM, and PALB2, as well as syndromes including Lynch syndrome and familial adenomatous polyposis. The fifth category encompasses personal factors such as advanced age, pernicious anemia, and personal or family history of gastric cancer. Finally, preventive factors highlight the importance of strategies such as targeted H. pylori eradication and the implementation of active surveillance programs in high-risk populations6,12.
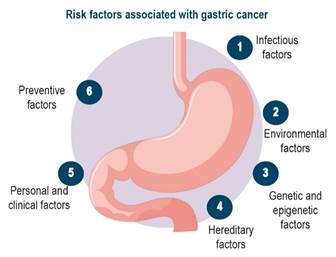
Figure 3 Risk factors associated with gastric cancer. Adapted from: Sundar R, et al. Lancet. 2025;405(10494):2087-21026.
Gastric adenocarcinoma has been classified from multiple perspectives, including clinical stage, macroscopic morphology, histology, growth pattern, and histogenesis. From a staging standpoint, it is categorized as early cancer (confined to the mucosa and submucosa, with or without lymph node metastasis) and advanced cancer (invasion of deeper layers)11,13. The latter is further classified according to Borrmann into five types (1-5), based on macroscopic morphology.
Regarding histological classification, the World Health Organization (WHO) recognizes subtypes such as papillary, tubular (TUB1 to TUB3), mucinous, signet ring cell, and undifferentiated, among others. The Broders classification, based on cellular differentiation, categorizes tumors into grades 1 through 4. The Lauren classification distinguishes three forms: intestinal type (glandular, well differentiated), diffuse type (poorly cohesive, infiltrative cells), and indeterminate9,11,13.
With respect to growth pattern, Ming proposed the expansive and infiltrative types14. In contrast, Nakamura and Sugano employed histogenesis to classify gastric cancer as differentiated (associated with intestinal metaplasia) or undifferentiated (originating from the native gastric mucosa), with distinct clinical, prognostic, and epidemiological characteristics14. Additional classifications, such as the Mulligan classification (pyloric, intestinal, and mucous cancer) and the Vienna classification (focused on early-stage lesions and dysplasia), further contribute to this multidimensional framework13. These classification systems are not mutually exclusive but complementary. Together, they allow a more comprehensive diagnostic, therapeutic, and prognostic approach to gastric adenocarcinoma.
The most recent classification of GC is no longer based solely on the traditional Lauren histological subtypes (intestinal and diffuse). Instead, it incorporates molecular profiles that enable more precise stratification with therapeutic implications15,16. Integrative analyses from The Cancer Genome Atlas (TCGA, 2014) and the Asian Cancer Research Group (ACRG, 2015) identified four principal molecular subtypes: chromosomal instability GC, microsatellite instability GC, genomically stable GC, and Epstein-Barr virus-positive GC. This updated classification provides substantial advances by identifying specific genetic and epigenetic alterations, including mutations in TP53, ARID1A, and PIK3CA, tyrosine kinase receptor amplifications, and CLDN18-ARHGAP fusions. These findings enable the development of targeted therapies and more personalized management strategies. Moreover, this approach facilitates identification of subgroups with distinct prognostic profiles. For instance, microsatellite instability GC is associated with improved survival and potential differential response to immunotherapy or targeted therapies, thereby overcoming limitations of previous histological classification systems (Table 2)15.
Table 2 Gastric cancer classification systems
| Classification system | Subtypes | Main characteristics |
|---|---|---|
| Lauren (1965) |
Intestinal Diffuse Mixed |
Intestinal: gland-forming, associated with intestinal metaplasia Diffuse: signet ring cells, poor cellular cohesion |
| WHO (2019) |
Tubular Papillary Mucinous Poorly cohesive (including signet ring cell) Rare variants |
Internationally standardized histological classification |
| TCGA (2014) |
EBV+ MSI CIN GS |
EBV+: hypermethylation, PIK3CA mutations, favorable response to immunotherapy MSI: high mutational burden, improved prognosis CIN: TP53 alterations, tyrosine kinase receptor amplification, HER2 amplification GS: CLDN18-ARHGAP fusions, diffuse phenotype |
| ACRG (2015) |
MSI MSS/TP53+ MSS/TP53- MSS/EMT |
MSI: improved prognosis MSS/TP53+: Intermediate prognosis MSS/TP53-: Intermediate-poor prognosis MSS/EMT: Diffuse phenotype, increased recurrence and peritoneal metastasis |
| Current integrated classification (2020-2023) | Molecular subtypes applied in clinical practice: HER2+, PD-L1+, CLDN18.2+, FGFR2b+, MSI-H, EBV+ | Directly guides targeted therapy and immunotherapy (trastuzumab, zolbetuximab, nivolumab, pembrolizumab, anti-FGFR2b) |
CIN: chromosomal instability; EBV: Epstein-Barr virus; GS: genomically stable; MSI: microsatellite instability. Adapted from: Januszewicz W, et al. Cancers (Basel). 2023;15(3):66416.
In the present case, the tumor corresponds to a poorly differentiated mixed gastric adenocarcinoma, histological grade 3, classified as Borrmann type 1 (polypoid), with invasion of the lamina propria, a tumor-free base, and no lymphovascular invasion. These features allow classification as early-stage GC despite its high histological aggressiveness.
Conclusion
This case represents an unusual and clinically challenging manifestation of mixed gastric adenocarcinoma. Detection at an early stage underscores the importance of endoscopy as a key diagnostic tool, even when lesions appear benign. Given its rarity and unpredictable biological behavior, this case highlights the need to strengthen screening programs, endoscopic surveillance, and rigorous histopathological evaluation, particularly in regions with moderate incidence such as Colombia, where GC remains a leading cause of cancer-related mortality.

