











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Dieulafoy lesion (DL) is a rare but potentially life-threatening condition characterized by a persistent, abnormally large-caliber artery associated with a significant risk of non-variceal upper gastrointestinal bleeding. Despite its low incidence, accounting for approximately 1%-2% of gastrointestinal hemorrhages, the profuse and painless bleeding it produces may compromise the patient’s hemodynamic stability, requiring prompt and effective intervention1,2. DL most commonly affects the stomach; however, it may also occur in other regions of the gastrointestinal tract, including the duodenum, colon, and gastric anastomoses. Early diagnosis by endoscopy is essential to identify the lesion and apply appropriate management techniques, primarily endoscopic interventions such as electrocoagulation, hemoclip placement, and laser photocoagulation3,4.
This report presents the case of a 70-year-old female patient with a medical history of type II diabetes mellitus and arterial hypertension who was admitted with massive hematemesis and severe epigastric pain. Severe anemia (hemoglobin [Hb]: 4.5 g/dL) was documented, and upper gastrointestinal endoscopy revealed a DL located on the lesser curvature of the stomach, with active bleeding successfully controlled by epinephrine sclerotherapy and hemoclip placement. The patient demonstrated favorable clinical progression and was discharged without complications. The objective of this article is to highlight key risk factors, pathogenesis, and treatment options in order to improve clinical outcomes and prevent serious complications associated with this condition.
Clinical case
A 70-year-old female patient with a history of type II diabetes mellitus and treated arterial hypertension presented to the emergency department with a one-hour history of abundant hematemesis in two episodes and severe burning epigastric abdominal pain associated with loss of postural tone. On admission, the patient was diaphoretic and hemodynamically unstable, with marked hypotension (blood pressure [BP]: 90/55 mmHg) and tachycardia (heart rate [HR]: 110 beats per minute [bpm]) in the context of upper gastrointestinal bleeding. Initial medical management included administration of 2000 mL of normal saline solution (NSS), omeprazole 80 mg intravenously (IV) as a bolus followed by continuous infusion at 8 mg/hour, one ampoule of IV tranexamic acid, and one ampoule of IV metoclopramide.
Laboratory tests performed at admission demonstrated severe anemia (Hb: 4.5 g/dL) and thrombocytosis (platelet count: 638,000), and four units of compatible packed red blood cells were transfused. Three hours after admission, the patient was evaluated by the Gastroenterology service, where the Glasgow-Blatchford score was calculated, yielding a result of 11 points (indicating a greater than 50% risk of requiring endoscopic, surgical, or transfusional intervention). Upper gastrointestinal endoscopy (esophagogastroduodenoscopy) was therefore performed, revealing:
Upper gastrointestinal bleeding secondary to a DL located in the distal third of the lesser curvature (Figures 1 and 2).
Successful control of active bleeding following epinephrine sclerotherapy and placement of two endoscopic hemoclips (Figures 3 and 4).
Hyperemic antral gastropathy with an erosive component.
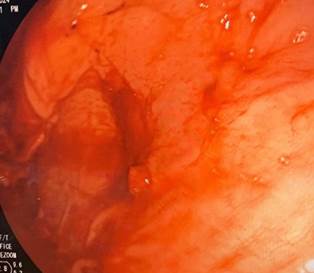
Figure 1 Dieulafoy lesion in the distal third of the lesser curvature (active bleeding). Image property of the authors.
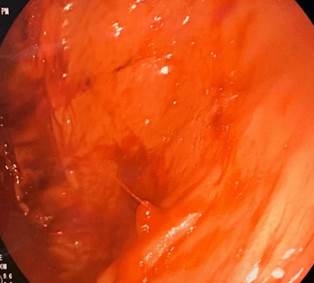
Figure 2 Dieulafoy lesion in the distal third of the lesser curvature (active bleeding). Image property of the authors.
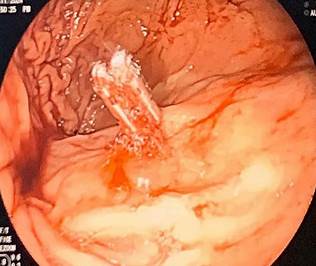
Figure 3 Dieulafoy lesion in the distal third of the lesser curvature after placement of endoscopic hemoclips. Image property of the authors.
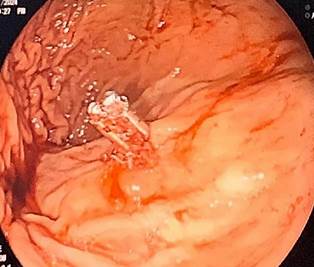
Figure 4 Dieulafoy lesion in the distal third of the lesser curvature after placement of endoscopic hemoclips, with successful control of bleeding. Image property of the authors.
Following successful endoscopic control of active bleeding, the patient was transferred to an intermediate care unit for continued medical management and hemodynamic monitoring. Due to favorable clinical progression, absence of signs of active gastrointestinal bleeding, and stabilization of hemoglobin levels, the patient was transferred to the general ward after 24 hours and discharged 24 hours later.
Discussion
Upper gastrointestinal bleeding refers to the signs and symptoms caused by hemorrhage originating from the gastrointestinal tract proximal to the ligament of Treitz. It is classified as variceal or non-variceal according to its etiology5. DL, also referred to as a persistent-caliber artery or cirsoid aneurysm, is characterized by a visible artery of constant caliber with an abnormal course that does not follow normal vascular branching patterns1. DL accounts for approximately 1%-2% of non-variceal upper gastrointestinal bleeding episodes that may threaten the patient’s life. It occurs in approximately 74% of cases in the stomach, 14% in the duodenum, 5% in the colon and gastric anastomoses, and 1% in the esophagus and jejunum/ileum1,2. Clinically, it is characterized by recurrent or intermittent episodes of abdominal pain, hematemesis, melena, hematochezia, and profuse painless bleeding requiring transfusion of blood products due to signs of hemodynamic instability6. Reported risk factors associated with this condition include advanced age, male sex (with a 2:1 ratio), and cardiovascular comorbidities.
The pathogenesis of DL remains uncertain. No genetic mutations have been described; however, vascular ectasia in the antrum has been associated with the following developmental abnormalities: disorders of antral motility (muscle hyperplasia), reduced blood flow in the antrum compared with the gastric fundus, the presence of neuroendocrine cells, and spontaneous arterial thrombosis and rupture1. Under normal conditions, arteries of the gastrointestinal tract progressively narrow as they approach their destination. In Dieulafoy syndrome, however, bleeding originates from an artery that, although histologically normal, is abnormally large (1-3 mm in diameter) and tends to penetrate the submucosa. This artery follows a tortuous course and protrudes toward the mucosa through a small mucosal defect (2-5 mm) accompanied by a fibrinonecrotic base. This lesion is commonly located in the upper third of the stomach, particularly along the greater curvature, where mucosal defects more frequently allow vascular protrusion5.
Diagnosis is established by endoscopic evaluation of the gastrointestinal tract, and diagnostic and therapeutic esophagogastroduodenoscopy is effective in identifying up to 70% of cases, as observed in the patient described6. The Glasgow-Blatchford score is a risk stratification tool used to predict the need for medical intervention (such as transfusion, endoscopy, or surgery) in patients with suspected upper gastrointestinal bleeding (Table 1). Scores of 0-1 indicate minimal need for intervention and allow outpatient management; scores between 2 and 6 require hospital-based intervention, with early endoscopic evaluation within 24 hours or sooner; scores of 7 or higher require continuous monitoring, hemodynamic resuscitation, and early endoscopy within the first 12 hours7.
Management of these patients is based on endoscopic hemostatic techniques such as electrocoagulation, laser photocoagulation, sclerotherapy, hemoclip placement, and band ligation3. DL responds well to mechanical therapies due to its focal nature and protruding morphology. However, electrocoagulation and thermocoagulation have been reported to increase the risk of transmural injury in organs with thin walls, such as the duodenum; therefore, hemoclips are preferred as an effective and safe hemostatic method4.
The present case involves a 70-year-old female patient with a history of type II diabetes mellitus and arterial hypertension who was admitted with massive hematemesis and epigastric pain, accompanied by severe anemia (Hb: 4.5 g/dL). Endoscopy identified a DL on the lesser curvature of the stomach, with active bleeding that was successfully controlled by epinephrine sclerotherapy and hemoclip placement. The patient showed stable clinical progression without complications and was discharged in good general condition. A comparison can be made with a previously reported case of a 17-year-old male patient at the Hospital de Veracruz, Mexico, previously healthy, who presented with sudden-onset upper gastrointestinal bleeding, hemodynamic instability, and severe anemia (Hb: 7 g/dL, decreasing to 3 g/dL after a second bleeding episode). Endoscopy revealed a lesion in the first portion of the duodenum with active bleeding and no evidence of ulceration, suggesting a DL. Initial treatment consisted of epinephrine injection at a 1:10,000 dilution administered in four quadrants, which achieved temporary hemostasis. However, the patient experienced severe recurrent bleeding requiring intensive resuscitation, intubation, and repeat endoscopy with repeated therapy, after which favorable clinical evolution was observed8.
Table 1 Glasgow-Blatchford Score
| Risk factor | Threshold | Score |
|---|---|---|
| Blood urea nitrogen (mmol/L) |
6.5-7.9 8.0-9.9 10.0-24.9 ≥25.0 |
2 3 4 6 |
| Hemoglobin in men (g/L) |
120-130 100-119 <100 |
1 3 6 |
| Hemoglobin in women (g/L) |
100-120 <100 |
1 6 |
| Systolic blood pressure (mmHg) |
100-109 90-99 <90 |
1 2 3 |
| Heart rate (bpm) | >100 | 1 |
| Melena | Present | 1 |
| Syncope | Present | 2 |
| Liver disease | Present | 2 |
| Heart failure | Present | 2 |
bpm: beats per minute. Table prepared by the authors.
Despite differences in lesion location, both cases highlight the importance of timely endoscopic diagnosis and the appropriate use of hemostatic therapies. Combined therapy (sclerotherapy plus hemoclip placement) is highly effective. In the present patient, bleeding control was successfully achieved in a single session without recurrence.
Conclusion
DL is an uncommon but serious cause of non-variceal upper gastrointestinal bleeding that may threaten the patient’s life due to its profuse and painless hemorrhage. Although its pathophysiology remains uncertain, it is associated with factors such as advanced age, male sex, and cardiovascular comorbidities. Early and accurate diagnosis by endoscopy is essential for appropriate management, which is based on effective endoscopic hemostatic techniques. A prompt and appropriate approach is critical to prevent major complications.
Key points
Dieulafoy lesion is primarily diagnosed by endoscopy, particularly esophagogastroduodenoscopy, which is effective in up to 70% of cases. It most commonly occurs in the stomach (74%), although it may also be located in the duodenum, colon, and other less frequent sites.
It is characterized by recurrent or intermittent gastrointestinal bleeding episodes, including hematemesis, melena, and hematochezia. Bleeding is typically profuse and painless, often accompanied by signs of hemodynamic instability requiring transfusion of blood products.
Management is based on endoscopic hemostatic techniques such as electrocoagulation, laser photocoagulation, sclerotherapy, hemoclip placement, and band ligation, which effectively control bleeding.

