











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Executive functions beyond clinical boundaries
Executive Functions (EFs) are higher-order cognitive processes essential for planning, organising, and adapting behaviour to changing goals and contexts (Lezak et al., 2012). The dysexecutive syndrome is characterised by an impairment of these EFs (Stuss & Levine, 2002). Subtle manifestations of dysexecutive syndrome, with lower frequency and intensity of symptoms, can be found in non-clinical populations (Chan, 2001). Evidence of executive dysfunction has been found in everyday decision-making related to health, finances, social behaviours (Moffit et al., 2011), academic performance, and quality of life (Bausela Herreras, 2017; Musso, 2009; Toplak et al., 2013). EFs show continuous development from childhood through adolescence, suggesting that EFs continue developing into late adolescence and early adulthood, likely reflecting ongoing brain maturation and changes in functional connectivity (Taylor et al., 2015). Insights into EFs have informed educational interventions (Diamond et al., 2007), emphasising that even minor EF variations can impact daily functioning, regardless of clinical diagnosis.
Subtle EF impairments in non-clinical populations are increasingly recognised as functionally significant. For instance, attentional control deficits, even at subclinical levels, moderate affective states and behavioural regulation (Drabble et al., 2014), echoing findings linking EF variability to anxiety and depression (Shaw et al., 2015). These have also been proposed as an explanation for the onset and maintenance of emotional disorders (e.g., Impaired Disengagement Hypothesis; Koster et al., 2011). Such evidence aligns with critiques that EF models must account for cross-domain interactions beyond traditional diagnostic boundaries (Barker & Morton, 2018; Manchester et al., 2004), which are particularly evident in the psychological and social consequences of executive dysfunction. For instance, difficulties with attentional control in the general population have been linked to shifts in affective state (Gerstorf et al., 2008) and may interfere with planning and cognitive flexibility (Chan, 2001). Collectively, this evidence broadensour understanding of dysexecutive phenomena beyond clinical thresholds, underscoring their relevance to everyday functioning.
The Dysexecutive Questionnaire: Structure, validity, and the need for cultural adaptation
The factorial structure of EF measurements has been widely analysed. While some models suggest a multidimensional structure (Amieva et al., 2003; Burgess et al., 1998; Chan et al., 2002; Chaytor & Schmitter-Edgecombe, 2007; Mooney et al., 2006), there is theoretical reasoning and evidence sustaining that EFs are a unidimensional phenomenon (Pedrero-Pérez et al., 2015; Takeuchi et al., 2013). The unidimensional approach argues that, despite the diversity of skills encompassed by EFs, there is an underlying unity reflecting general cognitive and behavioural self-regulation (Miyake et al., 2000). The DEX-Q (Dysexecutive Questionnaire; Wilson et al., 1996) assesses planning, organisation, inhibition, and emotional control. Participants provide responses reflecting the frequency of experiencing difficulties in everyday situations related to EFs. It has been used in clinical and research evaluations in both non-clinical (Takeuchi et al., 2013) and clinical contexts (Emmanouel et al., 2014). It has also been translated and validated into Spanish as the DEX-Sp (Pedrero-Pérez et al., 2009). However, this questionnaire raises concerns regarding its link with objective measures of EFs. While some studies have reported an inverse correlation between DEX scores and certain BADS subtests (Knight et al., 2002; Wilson et al., 1996) others have found no significant association between subjective and objective assessments (Burgess et al., 1998; Wood & Liossi, 2006) or have shown that such associations may only emerge with specific forms of DEX administration (Emmanouel et al., 2014). Moreover, concerns have been raised about the content validity of the DEX due to its strong correlation with personality measures (Gerstorf et al., 2008). However, this may reflect the close link between frontal lobe dysfunction and personality traits, particularly behavioural and emotional symptoms in daily life. In a study carried by de León et al. (2010), significant correlations were observed between disexecutive symptoms, novelty seeking, harm avoidance, and self-directedness. These traits are partly predicted by everyday behavioural symptoms associated with frontal impairments.
Although multifactorial solutions have been found, other studies show evidence for the unidimensionality of the DEX. For instance, Gerstorf et al. (2008) found high inter-factor correlations in models with three or more factors, suggesting a more parsimonious unifactorial solution. Similarly, Takeuchi et al. (2013) reported that the proportion of variance explained by the first factor in a five-factor solution was disproportionately high compared to the remaining four, suggesting a unidimensional structure for the DEX-Sp. Likewise, Pedrero-Pérez et al. (2011) explained that the results of an initial exploratory factor analysis (EFA) using the maximum likelihood method pointed to a potential unifactorial solution, given the large difference in variance explained between the first and second factors. Subsequently, recognising that previously used factor analysis techniques were unsuitable for ordinal measurements such as the Likert-type items of the DEX-Sp, Pedrero-Pérez et al. (2015) reanalysed its structure. Using more appropriate techniques, such as EFA based on polychoric correlations and parallel analysis, Pedrero-Pérez et al. (2015) concluded that the DEX-Sp’s structure is unidimensional.
Evidence of the validity and reliability of the DEX-Sp has been demonstrated in Spanish samples (e.g., Pedrero-Pérez et al., 2009, 2015) and the DEX-Q has been validated in three Latin American countries (Mondragón Bohórquez & Riveros Miranda, 2011; Oliveira et al., 2021; Querejeta et al., 2015). However, a review of the literature did not identify studies concerning the psychometric properties of these instruments in the Mexican population. This study aims to test the validity, reliability, and equivalence of the DEX-Sp in non-clinical samples from Mexico (León, Ciudad Juárez, Mexico City) and Spain (Madrid). In order to obtain evidence of validity through external criteria, a measurement of alcohol use disorder is also included (Babor et al., 2001), expecting that the Dex-Sp scores will be positively associated with this measurement (Gil-Hernandez & Garcia-Moreno, 2016; Houston et al., 2014). Given recent calls for unifying EF theories across disciplines and populations (Barker & Morton, 2018), this work contributes to refining EF assessment tools for diverse contexts. By examining EFs in general populations through the DEX-Sp, this study directly addresses calls for unifying frameworks that bridge typical and atypical functioning, while contributing to the development of culturally sensitive assessment tools.
Method
Participants
An Exploratory Factor Analysis (EFA) was conducted with a sample of 190 men and 145 women, with a mean age of 26.82 years (SD = 10.85), primarily residents of León, Guanajuato (85.7%) and other states in central Mexico. The most common education levels were incomplete or ongoing undergraduate studies (53.3%), completed undergraduate studies (17.9%), and completed upper secondary education (15.8%). Most participants were engaged in full-time work (37.5%), 31.3% were exclusively studying, 25.3% were both studying and working, and 6% were neither studying nor working.
The confirmatory and invariance factor analyses were conducted on four additional samples. From León, Guanajuato, in the Central-North region of Mexico, 182 women and 135 men responded, with a mean age of 26.31 (SD = 10.50). Their main education levels were incomplete or ongoing undergraduate studies (54.7%), upper secondary education (18.4%), and completed undergraduate studies (16.3%). The majority were engaged in full-time work (36.3%), full-time study (35.3%), or both studying and working (25.3%). From Mexico City, in the Central-South region of Mexico, 156 women and 59 men participated, with a mean age of 25.29 (SD = 11.72). Their education levels included incomplete or ongoing undergraduate studies (68.8%), completed undergraduate studies (13%), and completed upper secondary education (7.9%). Most participants were exclusively studying (57.2%), engaged in full-time work (19.5%), or both studying and working (18.6%). From Ciudad Juárez, Chihuahua, in the Northwest region of Mexico, 138 women and 56 men participated, with a mean age of 22.51 (SD = 5.91). Their education levels were primarily incomplete or ongoing undergraduate studies (82%), upper secondary education (8.8%), and completed undergraduate studies (6.2%). Participants were mainly exclusively studying (51%), both studying and working (39.8%), or exclusively working (9%). From Madrid, Spain, 157 women and 57 men participated, with a mean age of 28 years (SD = 13.28). Their main education levels were incomplete or ongoing undergraduate studies (49.1%), upper secondary education (17.5%), completed undergraduate studies (11.8%), and completed postgraduate studies (14.6%). Participants were engaged exclusively in studying (52.2%), both studying and working (33.3%), exclusively working (12.6%), or neither studying nor working (1.9%).
Instruments
Spanish Version of the Dysexecutive Questionnaire - Self Report (DEX-S-Sp; Pedrero-Pérez et al., 2009): The DEX-Q is a 20-item questionnaire originally developed as part of the Behavioural Assessment of the Dysexecutive Syndrome (BADS; Wilson et al., 1996) to measure executive dysfunction in daily life. It includes both a Self-Report version (DEX-S) and an Informant-Report version (DEX-I), which are typically used together to compare self-perceived executive difficulties with an external observer’s evaluation. The version used in this study, DEX-S-Sp, is the Spanish translation and validation of the DEX-S (Pedrero-Pérez et al., 2009). Previous studies have reported high internal consistency, with Cronbach’s alpha values ranging from .91 (Pedrero-Pérez et al., 2009) to .87 (Pedrero-Pérez et al., 2011).
Alcohol Use Disorders Identification Test (AUDIT; Babor et al., 2001): A 10-item instrument developed by the World Health Organisation that assesses risky alcohol consumption, symptoms of dependence, and harmful alcohol use (e.g., “How often do you have a drink containing alcohol?”).
Procedure
The Ethics and Research Committee of the Universidad Autónoma de Ciudad Juárez granted ethical approval to conduct this study, which was carried out in accordance with the ethical guidelines of the American Psychological Association (APA, 2017) and the principles outlined in the Declaration of Helsinki (WMA, 2013) as well as the national regulations of Spain and Mexico regarding research involving human participants. The questionnaire was administered through the Microsoft Teams platform, and the link was shared on social media. The first page of the survey provided participants with a consent form that outlined the study’s objectives, the information to be requested, the approximate duration, and the assurances regarding the anonymity and the confidentiality of their responses, which were safeguarded by the research team leader. Participants were also informed of their right to withdraw from the study at any time without any consequences and were provided with an email address for additional information.
Since the original translation of the DEX-Sp was conducted in and for Spain, the wording of its items was reviewed and administered to a small group of 40 participants as a pilot test to identify potential variations in meaning between samples from Mexico and Spain. This process revealed translation issues in the original Spanish version, which stemmed from inaccuracies in the translation from the original English version. As a result, linguistic and cultural modifications were made to improve the accuracy and appropriateness of the DEX-Sp for both Spanish and Mexican populations. For instance, in one item, the phrase “me pongo demasiado excitado” (“I get too excited”) was changed to “me emociono demasiado” (“I get overly emotional”), as “excitar” in Spanish typically refers to sexual arousal (Real Academia Española, 2023) rather than heightened emotion. Another item replaced “episodios” (“episodes”) with “eventos” (“events”) to better reflect everyday language. In a third item, “estoy como aletargado” (“I feel kind of sluggish”) was revised to “me siento apático/a” (“I feel apathetic”) for greater accuracy. A further change involved replacing “cortarme” (“to stop myself”) with “dejar” (“to stop”), clarifying the intended meaning. Finally, “enfado” (“annoyance”) was substituted with “enojo” (“anger”) in an item describing disproportionate emotional reactions.
Data analysis
For the EFA, the polychoric correlation matrix was analyzed using the Factor programme (Ferrando & Seva, 2017). It was verified that factor extraction was possible with KMO values ≥ .7 and statistically significant Chi2 in the Bartlett test. Factors were extracted using the robust diagonal weighted least squares method, following the estimates from the parallel analysis of optimal implementation (Timmerman & Lorenzo-Seva, 2011), comparing with the theoretically expected dimensions. Items with values below .5 in the sample adequacy measure were discarded (Ferrando et al., 2023). Acceptable goodness-of-fit values were considered RMSEA ≤ .08, CFI ≥ .95, GFI ≥ .90, and AGFI ≥ .90, and non-significant values in the Chi2 contrast test (Ferrando et al., 2022). The exploratory factor analysis solution was tested through four confirmatory factor analyses in each of the samples (León, Ciudad Juárez, Mexico City, and Madrid, Spain), estimating discrepancies using the diagonal weighted least squares method, with optimal goodness-of-fit values of RMSEA ≤ .08, CFI ≥ .95, GFI ≥ .90, and SRMR ≤ .08, and non-significant values in the Chi2 contrast test (Kline, 2023). The equivalence of the instrument across the four samples was tested using a multigroup analysis, considering acceptable Chi2 increases that were not statistically significant, decreases less than .01 in the CFI index, and maximum increases of .015 in the RMSEA index (Chen, 2007) when comparing the configural, metric, and scalar equivalence of the model. Internal consistency was calculated using McDonald’s omega formula (Zinbarg et al., 2005). Possible relationships between the mean scores of the DEX-Sp and the sum of points obtained from the AUDIT instrument to provide evidence of validity through external criteria were analysed using Spearman’s correlations. These analyses were conducted using the JASP programme (2024).
Results
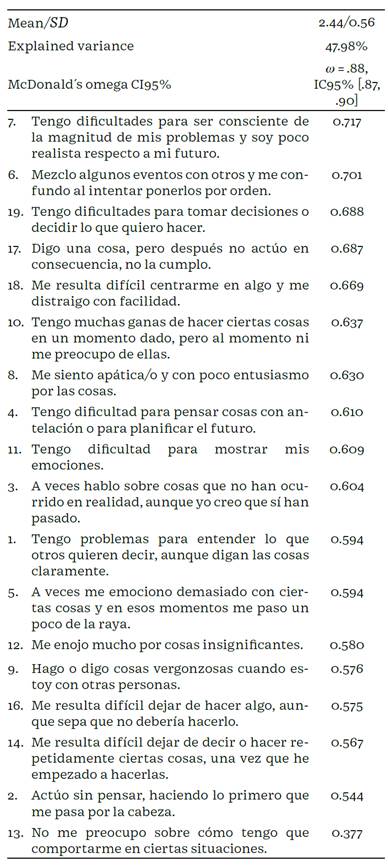
Two items (“Tiendo a ser bastante activa/o, y no puedo quedarme quieto/a por mucho tiempo” (“I tend to be quite active, and I can’t stay still for long,”); “No me entero, o no me interesa, lo que opinen otros sobre mi comportamiento” (“I am unaware of, or unconcerned about, how others feel about my behaviour”) were discarded for obtaining MSA values < .5. The correlations between these two items were statistically significant but low (rho = .14, p < .001), indicating that they share variance but not enough to form an additional dimension, as this was not identified as such by the parallel analysis. Analysing the remaining items, the KMO indices (KMO = .91) and Bartlett’s test (cZ = 2423.6, p < .001) confirm that factor extraction from the polychoric correlation matrix is feasible. The parallel analysis identifies a single factor structure, as shown in Table 1, obtaining adequate goodness-of-fit indicators (RMSEA = .04, 90% CI (.10, .05), CFI = .98, GFI = 1, AGFI = 1), except for the cZ index (cZ = 165.84, p = .03). The differences in means between men (M = 2.41) and women (M = 2.41) were not statistically significant (t1252 = -0.134, p = .89).
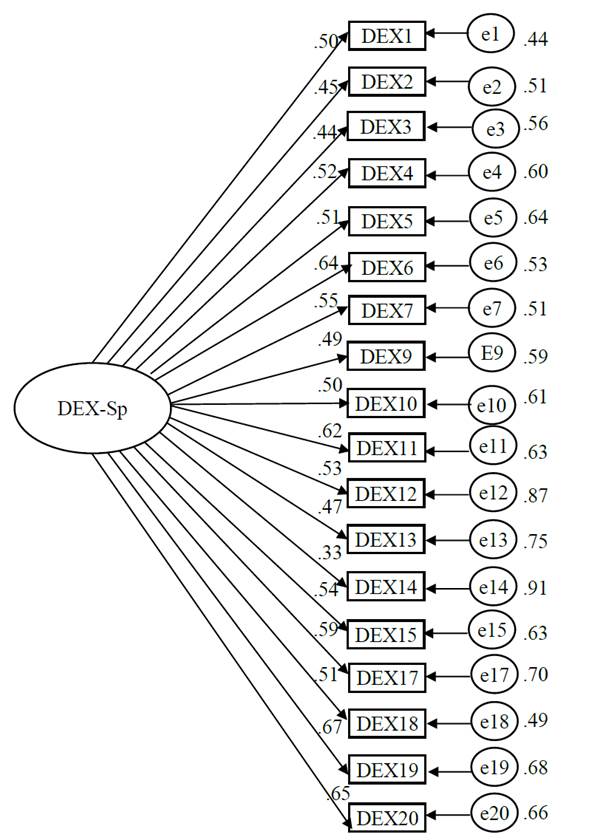
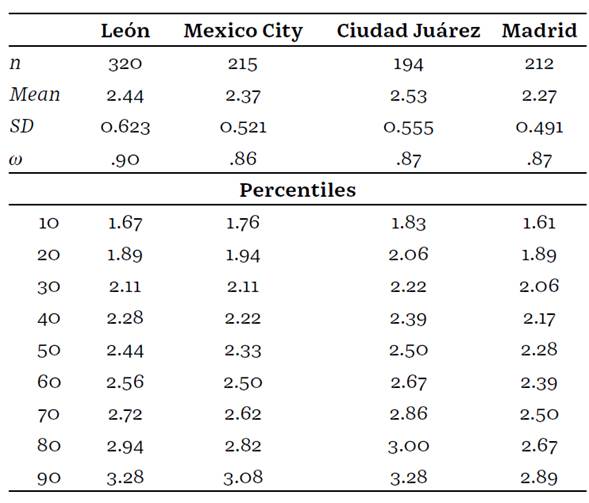
The confirmatory factor analysis of this structure (see Figure 1), conducted on a sample of 941 participants from León, Ciudad Juárez, Mexico City, and Madrid, showed adequate fit indices(RMSEA = .03, 90% CI (.02, .04), CFI = .98, GFI = .99, SRMR = .04) except for the Chi2 index (c2 = 282.09, p < .001). Z-values for factor loadings range between 21.74 to 40.76 and p-values < .001 for all items. To test the equivalence of this factorial structure across the four samples, confirmatory factor analyses and reliability tests were first conducted separately, yielding adequate fit and reliability indicators for León (c2 = 102.33, p = .98, RMSEA < .001, CFI = 1.0, GFI = .99, SRMR = .04, w = .90), Ciudad Juárez (c2 = 134.28, p = .50, RMSEA < 001, CFI = 1.0, GFI = .99, SRMR = .06, w = .86), Mexico City (c2 = 282.09, p = .29, RMSEA = .01, 90% CI (< .001, .03), CFI = .99, GFI = .99, SRMR = .06, w = .86), and Madrid (c2 = 132.72, p = .53, RMSEA < .001, 90% CI (< .001, .03), CFI = 1.0, GFI = .99, SRMR = .06, w = .87). Subsequently, the multi-group comparison analysis (see Table 2) showed that the unrestricted model produced adequate fit indices for all indicators, with statistically significant factor loadings for all items with Z-values ranging from 6.40 to 18.32 and p < .001 across all samples. This result confirms that the instrument’s structure is consistent across the four samples, meaning the measurement is effectively composed of the same items forming a single factor across the four samples. Comparing these values with those obtained from the metric equivalence-restricted analysis revealed statistically significant increases in Chi2, decreases in CFI = .014, and increases in RMSEA = .033. These differences indicate that while the same items are important for measurement across the four samples, their factor loadings-and thus their importance-are not identical among the samples. The instrument’s percentiles for the four samples are presented in Table 3. Thus, it is concluded that the instrument achieves configural equivalence but not metric equivalence across the four samples. Since metric equivalence was not achieved, equivalence in intercepts or residuals was not tested further.

To obtain evidence of validity using an external criterion, the scores of the DEX-Sp questionnaire were correlated with the scores of the AUDIT instrument. Using the classification criteria of Babor et al. (2001) for interpreting the AUDIT, it was observed that 62% of the sample (with maximum scores of 7) fell within low-risk consumption or abstinence, 32.8% (with scores between 8 and 15) exceeded the low-risk recommendations, 3.2% (with scores between 16 and 19) were in the risky and harmful consumption category, while only 2% (with scores of 20 or more) indicated possible alcohol dependence. Consistent with the hypothesis, positive correlations were observed, which can be considered of typical size in studies concerning individual differences (Gignac & Szodorai, 2016), between the mean scores of the DEX-Sp questionnaire and the total scores of the AUDIT instrument. This positive and statistically significant relationship persists in both groups classified as lowrisk or abstinent on the AUDIT (rho = .218, p < .001) and in those who slightly exceeded the low-risk threshold (rho = .191, p < .001). Due to insufficient sample size, these analyses could not be conducted for participants with hazardous/harmful drinking (n = 40) or probable alcohol dependence (n = 24).
In their study, Gerstorf et al. (2008) found a small but statistically significant negative association between DEX scores and age. This was also observed in the present study (rho = -.238, p < .001), indicating that older individuals reported lower DEX scores. Gerstorf et al. (2008) suggest that this unexpected result may stem from younger participants in their study also reporting higher levels of negative effects, which could exacerbate executive dysfunction.
Discussion
The structure of DEX-Sp, as expected, shows a unifactorial structure in line with the results of Pedrero-Pérez et al. (2015). In this study, as in previous studies that also identified a unidimensional structure (Gerstorf et al., 2008; Pedrero-Pérez et al., 2015; Takeuchi et al., 2013), adequate reliability levels were observed, indicating a good internal consistency of the instrument, providing evidence that this is an optimal structure.
This same structure can be considered valid for the samples from the three regions of Mexico and the one from Madrid, Spain. However, the equivalence of the instrument for these samples is maintained only at the configural level, without achieving metric equivalence, intercepts, or residuals. That is, the same items are organised in a unidimensional structure and can be applied to all four samples, although the loadings, means, and residuals are not comparable between them. It is worth noting that the DEX-Sp also achieved acceptable reliability levels across all four samples.
The correlation analyses with the AUDIT instrument provided evidence of validity through external criteria showing that high levels of consumption are associated with executive dysfunction. For example, Gil-Hernandez and Garcia-Moreno (2016) indicated that adolescents with high alcohol consumption reported greater executive symptomatology and disinhibition, and Houston et al. (2014) showed a positive relationship between alcohol consumption and total scores on the DEX-Q in a community sample. Similarly, the negative correlations between DEX-Sp scores and age align with previous findings reported by Gerstorf et al. (2008). Comparing the DEX-Sp with both standard tests (e.g., working memory tasks) and real-world analogs could clarify whether self-reported difficulties reflect cognitive deficits or functional limitations in non-clinical populations, strengthening its utility for identifying subclinical impairment.
There should also be discussion regarding two items that were discarded because they share little variance with the rest of the instrument and can be interpreted as not measuring the same construct. They also share minimal variance with each other, indicating they would not form part of an additional dimension a finding confirmed by the parallel analysis which identified only a single dimension. In the case of the item “I tend to be quite active, and I can’t stay still for long,” the analyses by Pedrero-Pérez et al. (2009; 2015) had already identified it as a problematic item in both clinical and non-clinical samples, concluding that the motor hyperactivity this item attempts to measure may be a consequence of a lack of executive control under certain circumstances, but it would not be a direct and unequivocal manifestation of executive dysfunction syndrome. Similarly, we consider that the item “I don’t notice or care what others think about my behaviour”, could reflect an individualistic or autonomous stance towards society, and not necessarily a syntom of executive dysfunction syndrome. It is important to acknowledge the recent development of other instruments for measuring executive dysfunction. For example, Pedrero-Pérez and de León (2022) have developed and provided evidence for the prefrontal symptom inventory, whose psychometric behaviour can be analysed later in samples from Mexico and Latin America. Additionally, it should be considered that early detection of executive dysfunctions in the non-clinical population has important implications for the prevention and management of mental and cognitive health issues in later stages of life (Toplak et al., 2013), allowing for preventive interventions or early treatment that could improve long-term outcomes (Diamond, 2013).
Conclusions
The DEX-Sp demonstrates a unidimensional structure that is consistent in its configuration and achieves adequate reliability indices across the four samples analysed in Mexico and Spain. Evidence of validity is further supported through external criteria, as positive correlations with measures of alcohol consumption were confirmed. Overall, the results affirm that the DEX-Sp is a valid and reliable instrument with robust psychometric properties for the samples analysed in Mexico and Spain, making it a valuable tool for future research in non-clinical populations.1 2 3

