











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Historically, individuals with severe mental disorders have been perceived as dangerous (1, 2). Nursing was directly confronted with the challenging environment of early psychiatric hospitals due to their close proximity to patient care. Given the precarious conditions of these facilities and the severity of psychiatric disorders, professionals were compelled to explore alternatives for managing patient behavior (1, 2).
It is likely that the culture of smoking in mental health services emerged as a strategy to manage the behavior of hospitalized individuals. Tobacco was thought to play a role in controlling symptoms and behaviors, helping to pass the time, and facilitating communication between professionals and patients. As a result, this may have contributed to the development of the triad of 'mental disorder-aggressiveness-smoking' (3, 4).
Currently, scientific evidence highlights the harmful effects of tobacco on individuals with mental disorders, including increased physical comorbidities, reduced life expectancy, exacerbation of psychotic symptoms, heightened anxiety with chronic use, interference with medication efficacy, and an elevated risk of suicide, among others (5-8). This concerning situation is emphasized by the significantly higher prevalence of smoking within the psychiatric population, which is two to three times greater than that among the general population (7, 9, 10).
Despite the harms of smoking for the psychiatric population, there is resistance among nurses and other professionals regarding the smoking ban in mental health services due to concerns about increased patient aggression (11-14). However, scientific evidence does not support the notion that implementing anti-smoking laws heightens the risk of dangerous behavior. For instance, an Australian study involving 200 interactions with individuals smoking in a hospital with a smoking ban reported only four instances of verbal aggression (11). Similarly, a Dutch psychiatric hospital found no increase in aggression when comparing incidents before and after the smoking ban was enforced (15). Thus, studies from different countries indicate that the fear of increased aggressiveness is a primary reason cited by professionals opposing the smoking ban in mental health services (4, 16, 17).
Considering that nursing is a profession dedicated to promoting and restoring health, professionals who continue to support smoking in mental health services likely do so due to a lack of knowledge. If nurses were fully aware of the harms of smoking for individuals with mental disorders and had the opportunity to dispel the myth that the anti-smoking law leads to increased aggressiveness, they would be less inclined to advocate for the continuation of smoking in these settings (16, 18). Therefore, this study can contribute to generating knowledge and reflections for nurses and other professionals working in mental health. Furthermore, the scientific literature contains a few studies addressing the relationship between aggression and the implementation of anti-smoking laws, highlighting the need to expand research in this area. Notably, no studies have been identified on this topic in Latin America.
The hypothesis of this study is that the implementation of the anti-smoking law in a psychiatric hospital is not associated with aggressive behavior among hospitalized individuals. The objective was to investigate the aggressive behaviors of patients in a psychiatric hospital adhering to the anti-smoking law and to identify the associated factors.
Materials and method
This was a cross-sectional epidemiological study conducted in a psychiatric hospital located in the countryside of São Paulo, Brazil. The hospital is philanthropic and, at the time of data collection, had 120 beds designated for short- or medium-term hospitalization of individuals with mental and behavioral disorders, as well as patients with substance use disorders. The bed distribution was as follows: 60 beds for hospitalizations funded by the Unified Health System (20 female and 40 male) and 60 beds for those funded by patients' own resources or health insurance (with no pre-established division for men or women).
The study population consisted of individuals discharged from public beds following short- or medium-term stays, as well as those hospitalized either before or after the implementation of the smoking ban in March 2018. Patients discharged from private beds were excluded due to the lack of authorization to access data from that unit. The convenience sample included 573 discharged patients. Inclusion criteria were: i) patients must have been discharged from public beds for short- or medium-term stays; ii) hospitalization must have occurred between September 2017 and August 2018, covering six months before and six months after the smoking ban was implemented. Exclusion criteria corresponded to discharged patients from private beds.
The project was registered on the Brazil Platform (CAAE number 79316817.7.0000.5393) and approved by the Research Ethics Committee of Ribeirão Preto Nursing School, Universidade de São Paulo. Because data collection involved secondary sources (medical records), the requirement for a free and informed consent form was waived.
A list provided by the computer team at the study site, which included the names of individuals hospitalized during the study period, was used to consult electronic records to obtain the following variables: sex (female, male), age (up to 35 years, 36 to 49 years, 50 years or more), current smoking status (yes, no), psychiatric diagnosis (psychotic disorders, mood disorders, personality disorders, substance use disorders, others), psychotropic drugs in use (up to four, five or more), hospitalization duration (up to 13 days, 14 to 24 days, 25 or more days), hospitalization period (before smoking ban, transition period, after smoking ban), hospital admission (voluntary, involuntary, or judicial), physical or mechanical restraints (yes, no), verbal or physical aggressive behaviors (yes, no).
To ensure data reliability, definitions were established for the variables physical restraint, mechanical restraint, and hospitalization duration prior to the start of data collection. Physical restraint refers to placing the individual in a room near the nursing station, without the presence of other patients, for continuous supervision by the nursing team. Mechanical restraint involves restricting the individual to the bed using fabric bands to limit their movements. The hospitalization period refers to the phase of psychiatric hospitalization relative to the implementation of the smoking ban at the study site. Three categories were defined for this variable: i) before the smoking ban (individuals hospitalized and discharged before March 2018); ii) after the smoking ban (individuals hospitalized from March 2018, when the anti-smoking law was enforced at the hospital); iii) transition period (individuals admitted when smoking was permitted—that is, before March 2018—, who experienced the implementation of the smoking ban as their discharge occurred after March of that year).
In addition to the criteria mentioned above, three additional measures were implemented to ensure reliability: i) data collection was conducted by a single researcher; ii) each medical record was reviewed twice to prevent inaccuracies; iii) absolute and relative frequencies, as well as the mean, minimum, and maximum values, were calculated before commencing bivariate and multivariate analyses to identify any outliers resulting from typing errors.
Statistical analysis was performed using Stata/IC (2017) and included descriptive statistics (absolute and relative frequencies, mean, standard deviation), bivariate analysis (Fisher's exact test at the 5% significance level), and two multiple Poisson regression models to calculate adjusted prevalence ratios and 95% confidence intervals.
The first multiple Poisson regression model was developed for the outcome variable "aggressive behaviors" (yes, no). Independent variables were selected based on a criterion of p < 0.20 from Fisher's exact test. The model included the following variables: age, number of drugs in use, length of stay, current smoking status, hospitalization period, and type of hospital admission. The second multiple Poisson regression model used "physical and mechanical restraints" (yes, no) as the outcome variable. Following the same selection criteria as in the previous model, the independent variables were age, number of drugs in use, length of stay, current smoking status, hospitalization period, and type of hospital admission.
To assess collinearity/multicollinearity among the independent variables, the mean "Variance Inflation Factor" (VIF) was evaluated for each model and for each independent variable. A VIF greater than 10 is generally considered problematic, as it may compromise the accuracy of the estimates (19-20). The mean VIF for the first model was 1.56, while for the second model it was 1.42, with no independent variable exceeding a VIF of 10.
For the independent variables included in both multiple models, crude prevalence ratios and 95% confidence intervals were calculated for comparison with the adjusted prevalence ratios.
Results
Out of the 573 participants, 65.4% were female, with a mean age of 42.7 years (SD 13.6). Approximately half (47.1%) had a diagnosis of a psychotic disorder, and 48% were smokers. The mean number of prescribed psychotropic drugs per participant was 3.8 (SD 1.2), as described in Table 1.
In 18.3% of the consulted medical records, there were instances of aggressive behaviors (verbal or physical), while 24.4% of the records documented the use of physical and/or mechanical restraint by the nursing team. Among individuals who underwent restraint procedures, the mean number of mechanical restraints was 2.2 (SD 2.4), and the mean number of physical restraints was 1.5 (SD 1.0) (Table 1).
Regarding the duration of hospitalization, the median length of stay was 24 days (interquartile range: 23 days). Approximately a quarter of the hospitalizations were involuntary or court-ordered (27.1%). The highest prevalence of aggressive behaviors was noted in the medical records of females, individuals aged up to 35 years, smokers, those diagnosed with a personality or psychotic disorder, those prescribed five or more psychotropic drugs, those hospitalized for 25 days or more, individuals admitted during the transition period of the smoking ban, and those who were hospitalized involuntarily (Table 1).
Fisher's exact test indicated a significant difference in aggressive behavior based on the variables of age, smoking status, number of psychotropic drugs in use, length of hospitalization, phase of hospitalization in relation to the smoking ban, and type of hospital admission (Table 1).
Table 1. Absolute (n) and relative (%) frequency of aggressive behaviors, as recorded in the medical records, according to personal and clinical profile, Brazil (n = 573)
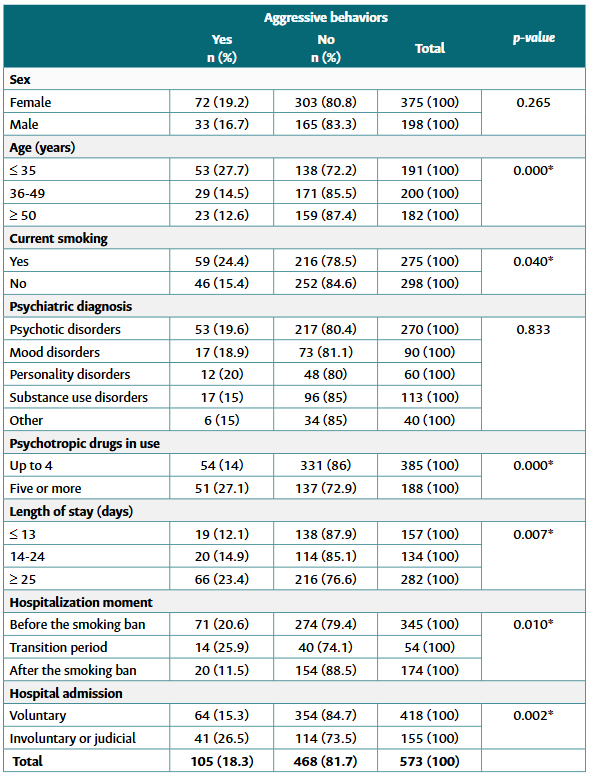
*Evidence of statistical difference (p < 0.05).
Source: authors.
As shown in Table 2, the Poisson multiple regression model indicated that, independent of the effects of other variables, the occurrence of aggressive behaviors was 121% higher among individuals aged 19 to 35 years, 73% higher among those hospitalized for 25 days or more, 55% higher among those admitted involuntarily or by court order, and 89% higher among those using five or more psychotropic drugs. Conversely, individuals hospitalized after the smoking ban was implemented exhibited aggressive behaviors 55% less frequently than those hospitalized before the ban.
Table 2. Crude and adjusted prevalence ratios (PR) for aggressive behavior, Brazil (n = 573)
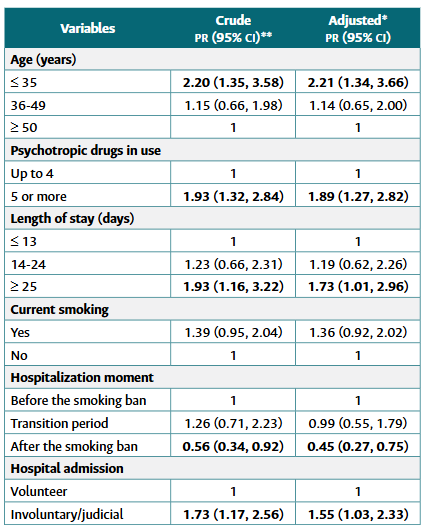
*Poisson regression model; **Prevalence Ratio and 95% Confidence Interval; PR (95% CI) in bold indicates evidence of statistical association.
Source: authors.
As shown in Table 3, physical and mechanical restraints were recorded more frequently in the medical records of men, individuals up to 35 years old, smokers, diagnosed with psychotic disorders, those using five or more psychotropic drugs, those hospitalized for 25 days or more, individuals admitted during the transition period of the smoking ban, and patients admitted involuntarily or by court order. Fisher's exact test showed a significant difference in aggressive behavior based on the variables of age, smoking status, number of psychotropic drugs in use, length of hospitalization, phase of hospitalization relative to the implementation of the smoking ban, and type of hospital admission.
Table 3. Absolute (n) and relative (%) frequency of physical and mechanical restraints, recorded in the medical records, according to personal and clinical profile, Brazil (n = 573)
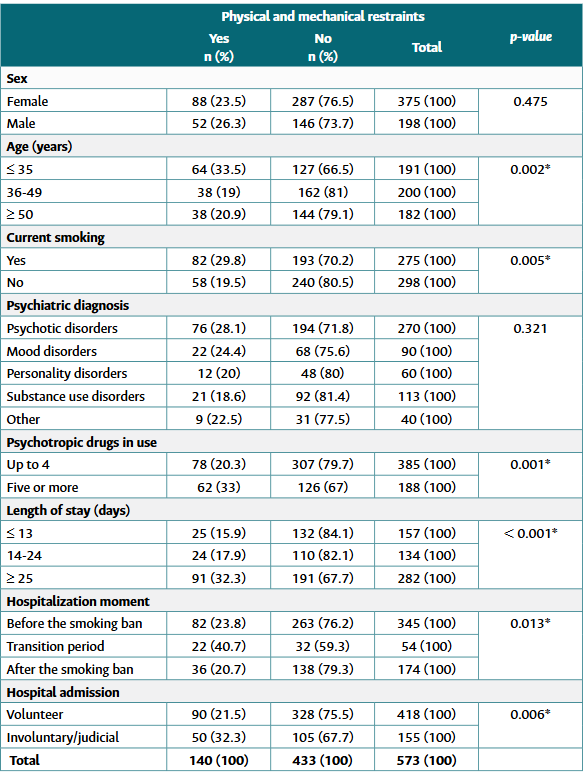
*Evidence of statistical difference (p < 0.05).
Source: authors.
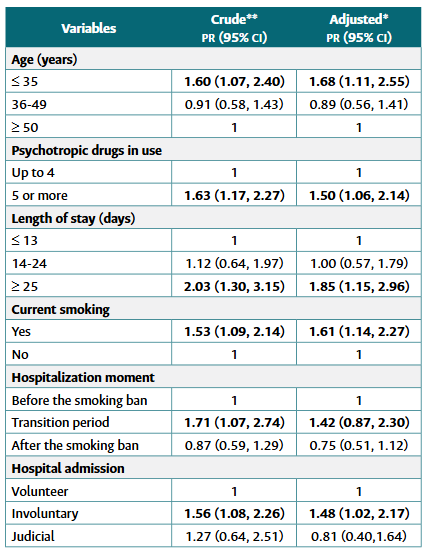
The prevalence of restraints was 61% higher among smokers, regardless of whether the psychiatric hospitalization occurred before or after the implementation of the smoking ban, and independent of other variables. Additionally, the prevalence of restraints was 68% higher among individuals up to 35 years old, 85% higher among those hospitalized for 25 days or more, 48% higher among those with involuntary hospitalizations, and 50% higher among those using five or more psychotropic drugs. When controlling for the effects of the other variables, the association between restraints and the transition period of the smoking ban was no longer significant (Table 4).
Discussion
In approximately one-fifth of the sample's medical records, instances of physical or verbal aggression directed at psychiatric hospital staff or other patients were documented. The prevalence of physical and/or mechanical restraints exceeded that of aggression, with such interventions recorded in one-quarter of the medical records.
The prevalence of aggression identified in this study aligns with findings from a representative sample of the U.S. population. That study reported a 12-month prevalence of aggression of 15% among individuals with severe mental disorders and 30% among those with other mental disorders, yielding an average prevalence of 22% (21). Similarly, a study conducted in a psychiatric emergency department in Berlin reported a prevalence of physical and mechanical restraints at 15% (22).
The findings on aggression and restraint prevalence in this study provide a nuanced perspective on individuals with mental disorders, who are frequently stigmatized by society as violent or dangerous. For instance, an American study found the highest prevalence of aggression (55%) among individuals without psychiatric diagnoses. Additionally, it noted that self-harm (including suicide attempts or self-mutilation) among individuals with severe mental disorders was three times more common than aggression directed at others (21).
Contrasting these findings, a systematic review reported a mean prevalence of verbal and physical aggression among individuals with mental disorders at 54%, with rates ranging from 8 to 76%. Such variability underscores the complexity of aggression, which is influenced by individual characteristics, the competence of professionals involved, and the care environment (14).
The demographic profile of individuals displaying aggressive behaviors is consistent with the literature, showing a higher incidence of aggression and management procedures (e.g., physical or mechanical restraints) among younger individuals, those hospitalized involuntarily, and those with extended hospital stays (14, 22, 23).
Although statistical analysis did not confirm gender differences in aggression prevalence, this study observed a higher frequency of aggression among women and a higher prevalence of physical and/or mechanical restraints among men. A systematic review of 146 studies reported no consensus on whether men or women were more likely to perpetrate verbal and physical aggression (14). However, regarding physical and mechanical restraints, a Swiss study involving 494 psychiatric inpatients found a higher prevalence of restraint use among men (23). Conversely, a German study reported a lower prevalence of restraints among women, although this difference diminished when controlling for other variables (22).
Similarly, while this study did not confirm a statistically significant relationship between psychiatric diagnoses and aggression or restraint prevalence, higher rates of aggression and restraint were observed among individuals with psychotic, mood, or personality disorders, consistent with other findings (14, 23).
The higher prevalence of restraints compared to aggression was expected, as these interventions aim to ensure the safety of patients and healthcare professionals, a principle well-established in the literature (22, 24). The data suggests that restraints fulfill their intended purpose of preventing aggression.
Notably, this study identified a higher frequency of physical restraints compared to mechanical ones, a finding echoed in a Swiss study (23). Furthermore, a Chinese study involving 98 nurses reported that 95% attempted alternative calming measures before resorting to mechanical restraint, reinforcing the principle of using such measures as a last resort (24).
The occurrence of aggression in psychiatric settings is a critical issue for nursing, as nurses spend the most time with patients with mental disorders, particularly during hospitalization. A Swiss study involving 1,128 nursing professionals from 13 psychiatric hospitals revealed that 24% had experienced physical aggression during their careers (25). Nursing professionals must be equipped to care for all parties involved in such incidents while maintaining their caregiving roles without personal involvement.
Nurses' susceptibility to aggression partly explains their resistance to supporting anti-smoking laws in mental health services. This resistance was highlighted in a Brazilian study involving 73 psychiatric hospital staff and a meta-synthesis of 15 studies conducted across the United States, Canada, Australia, the United Kingdom, and Brazil (26, 27).
Thus, a first reading of the data from the present study (bivariate analysis) might suggest that the implementation of the smoking ban is linked to an increase in aggressive behaviors, as aggression prevalence was higher during the transition period compared to pre-ban levels. Furthermore, the bivariate analysis may lead readers to infer that the higher prevalence of aggressive behaviors during the transition period stems from smokers' resistance, as their medical records show more instances of aggression compared to non-smokers.
An in-depth analysis of the data does not support the notion that smokers exhibit more aggressive behavior than non-smokers. By controlling personal and clinical variables, the association between smoking and aggression becomes insignificant. This finding highlights that aggression is linked to the personal and clinical profiles of individuals with mental disorders—such as younger age, high usage of psychotropic drugs, prolonged hospital stays, and involuntary hospitalization—rather than to smoking status.
In addition, the multivariate analysis provides a fresh perspective on aggressive behaviors in the context of the anti-smoking law. After controlling personal and clinical variables, the findings reveal a lower prevalence of aggression following the implementation of the smoking ban, challenging the assumption that such measures increase aggressiveness.
Consistent with the results of the present study, researchers in the United Kingdom reported a 39% reduction in recorded instances of physical aggression after implementing a smoking ban in psychiatric hospital wards, even after accounting for confounding variables such as sex, age, psychotic disorders, and involuntary hospitalization (28). A systematic review of 11 studies conducted in Australia, Canada, the United States, and the United Kingdom found that 75% of the analyzed studies reported either a reduction or no change in aggressive behaviors following smoking bans (17). Similarly, an American study across 14 psychiatric inpatient wards observed no changes in physical or mechanical restraint practices post-ban (29).
In contrast to the present study, researchers in London found that aggression incidents were higher under a partial smoking ban (designated smoking times) compared to a total ban (13). This suggests that smoking permission in mental health facilities is a problem, not a solution.
Since nursing is a profession characterized by continuous interaction with hospitalized individuals, nurses' perceptions of aggression risk play a critical role in determining whether restraints are implemented. By recognizing in nursing professionals an accurate capacity for observation (conferred to them due to the proximity of care), the interprofessional team usually validates the evaluation performed by them. Consequently, understanding nurses' perspectives on the use of physical and mechanical restraints, as well as the factors they identify as triggers for aggression, is essential for modifying restraint practices in mental health settings (30).
The critical role of nursing in the application of physical and mechanical restraints brings attention to an unexpected finding of the present study: A higher prevalence of these restraints among smokers, irrespective of whether hospitalization occurred before or after the implementation of the anti-smoking law. Although the multivariate analysis found no association between aggression and tobacco smoking, smokers were subjected to physical and/or mechanical restraints more frequently than non-smokers. This observation raises the question of whether this disparity reflects a perception among nursing staff that smokers are more prone to aggression, potentially leading to a premature decision to implement restraints before clear and assertive signs of imminent aggression are evident. A second interpretation may be explained by the fact that smokers often represent the most severe cases—characterized by a predominance of psychotic disorders, longer durations of diagnosis, greater use of psychotropic medications, and more pronounced symptomatology—, which could trigger the need for restraint, in certain situations, precisely to avoid the imminence of aggressions.
Future studies should prioritize investigating these newly formulated hypotheses, as nursing professionals play a pivotal role in delivering effective and humanized care. Research from the United Kingdom highlights that addressing misconceptions about aggressiveness in the context of smoking bans within mental health services can alleviate the anxiety of nurses and other professionals. This reassurance, supported by scientific evidence demonstrating the safety and effectiveness of smoking bans, can also provide confidence to service managers when implementing such policies (12).
Similar to how individuals with mental disorders may culturally perpetuate the perceived benefits of smoking across generations, older nursing professionals might influence their younger colleagues to permit tobacco use in mental health services to mitigate aggression. This cycle of misinformed beliefs can only be disrupted through the generation of new knowledge and critical reflection, which represents a key contribution of the present study.
This study, however, has certain limitations. The frequency of aggressive behaviors and the use of restraints was extracted from medical records, where incomplete documentation may have led to an underestimation of these occurrences. Furthermore, the lack of data on individuals receiving nicotine replacement therapy or Bupropion restricted the inclusion of these variables in the multiple regression model, which may have affected the comprehensiveness and depth of the findings.
Conclusions
This study provides insights for reflecting on the aggressiveness of individuals hospitalized in a psychiatric hospital during the period of the Anti-Smoking Law. Although the bivariate analysis suggested a higher occurrence of aggressive behaviors during the transition phase of the implementation of the anti-smoking law, this finding did not remain significant after controlling for the influence of other variables. Additionally, the multivariate analysis revealed a lower prevalence of aggression (verbal or physical) after the tobacco smoking ban was enforced.
Regarding the procedures for managing aggression, the multivariate analysis identified a higher prevalence of physical or mechanical restraints among smokers, regardless of the anti-smoking law and the influence of other independent variables. The association between restraints and the timing of psychiatric hospitalization, relative to the enactment of the law, was no longer significant in the multivariate analysis.

