











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Osteoarthrosis is an osteoarthropathy that can cause pain, deformities, weakness, and other abnormalities that affect the hands. About 10% of people over the age of 60 and more than 90% of people over the age of 80 have been observed to be affected by joint osteoarthritis. 1)(2
Between the ages of 71 and 100, the prevalence of symptomatic OA reaches 26% in women and 13% in men. As a result of the disease, these patients lose strength in their hands and have difficulty with daily manual activities. The main joints involved are the proximal and distal interphalangeal joints and the first carpal-metacarpal 3.
The etiology of OA is far from being fully understood, despite being the most frequent rheumatological pathology and probably also the medical pathology whose presence has been known for the most years 4. The structural changes seen are associated with confirmed or probable risk factors including demographic characteristics, obesity and dietary factors, joint load and injury, and joint shape and alignment 5)(6.
Diagnosing OA requires a multifaceted approach, as there is no single test or finding that has the appropriate sensitivity and specificity to make the diagnosis alone. EULAR published a series of recommendations for the diagnosis of OA that were developed using a combined methodology based on evidence and expert consensus 7. Prior to the EULAR task force, the best resource for diagnostic criteria for OA was the American College of Rheumatology (ACR) Criteria for the Classification and Reporting of Osteoarthritis of the Hand (1990) 8.
The first step in diagnosis is to compare a patient's complaints with typical presenting symptoms. Osteoatritis most often presents as pain in the hand with use, with or without mild morning stiffness, affecting one or more joints of the hand. The IFD joint is usually involved, followed in order by the base of the thumb and the IFP joint. This distribution of the joints involved may be somewhat useful in differentiating OA from other osteoarthritis, but the specificity of this diagnostic approach is low. Similarly, the presence of Heberden's or Bouchard's nodes may aid in diagnosis, but it is not specific enough to be considered as a single diagnostic marker.
X-rays are the first line of research in the presence of a painful hand, taking postero-anterior and lateral wrist x-rays are essential, at the same time they allow us to make the diagnosis and monitoring of osteoarthritis, being an affordable and economical technique. Although conventional radiography is the most widely used technique for assessing the structural features of OA, significant advances have been made in the field of imaging in the last decade, allowing for a more accurate assessment of bone and soft tissue abnormalities 9.
While newer modalities, such as Magnetic Resonance Imaging (MRI) and ultrasound, GO, have increased understanding of the multiple pathologies that contribute to the OA phenotype, it is unclear how they should be used in routine care. The role of imaging in clinical practice for the diagnosis, management, and follow-up of OA has not been clearly defined, given that studies have yet to illustrate a true and reproducible benefit 10.
Bone scanning is not part of the initial evaluation of osteoarticular disease, but it is a valuable diagnostic tool due to its sensitive and non-invasive nature. Changes in GO have been used as a means of assessing the disease process in a patient population with chronic OA of the knee and hip joints. Most had narrowing of the joint space and symptomatic subchondral bony changes in the knees and hips; these signs are generally considered to be the cardinal characteristics of OA 11)(12)(13 .
In the case of the hand, it is increasingly used in the evaluation of painful wrist because it is successful in the early detection of infectious, inflammatory, and pain problems between soft tissue and bone, traumatic and ischemic events of wrist components.
It is often used when patients have wrist pain despite treatment or when the physical examination and x-ray are inconclusive or unspecial. The strength of the technique lies in its ability to provide early physiological information, such as the pattern of perfusion and bone metabolic activity, given that the radiopharmaceutical used is 99mTc-MDP, which reaches the bone through the bloodstream and binds to the hydroxyapatite crystal with high affinity, allowing the osteoblastic activity to be indirectly evaluated 7)(14)(15 .
Between 1986 and 1995, worldwide studies evaluated the radiological features of osteoarthritis of the hand, comparing them with radionuclide bone scanning images. Abnormal uptake with the use of 99mTc-MDP was confirmed to be consistent with early osteophyte formation in the hands. This led to the conclusion that an abnormal scan reflected the progression of OA at a given time point in time and that qualitative gamma graphic changes paralleled the progression of variable OA over time. Subsequently, at the national level in 2016, a single prospective study was carried out on scintigraphic findings in hands in patients without osteoarticular pathology. The goal was to improve diagnostic accuracy, avoiding over- and under-diagnosis. Hyper-uptake patterns were observed in hand and wrist joints on the scintigraphy, although this design did not allow a clinical or imaging correlation of the abnormalities present in the scintigraphy 7)(14)(15 .
Considering the above, this study aimed to evaluate the criterion validity, discriminatory capacity and uptake rate in patients who underwent a 99mTc-methylene diphosphonate (99mTc-MDP) scintigraphy with suspected osteoarthritis in the hands, taking as a reference the clinical diagnosis according to the classification criteria of the American College of Rheumatology (ACR) of 1990.
Methods
Study Design and Population: longitudinal study, which was carried out in a high-complexity center in the department of Santander, Colombia during the year 2023. The population consisted of patients who underwent a total body bone scan with 99mTc - MDP in hands. The inclusion criteria were patients between 40 and 80 years of age who agreed to participate by informed consent. Patients with mental disorders, diagnosis of psoriasis, rheumatoid arthritis, among other exclusion criteria detailed in the protocol, are excluded.
Data collection and variable definition: data were collected using an instrument designed for the study that includes sociodemographic characteristics, comorbidities, scintigraphy indications, scangraphic findings, clinical and functional outcomes of the hand. Primary variables include age, sex, BMI, smoking, physical activity, work activity, indication for scintigraphy, and hand scan results. Data were entered into a database and analyzed using Stata 14®.
Statistical analysis: a univariate analysis was performed to characterize patients and a bivariate analysis using chi-square tests to compare scintigraphic findings with clinical data. Sensitivity, specificity, predictive values, and positive and negative likelihood values were calculated to evaluate the discriminatory capacity of bone scintigraphy in the diagnosis of osteoarthritis, using clinical diagnosis as the reference standard. The area under the ROC curve was used to compare the areas of the curves obtained in both hands. The ROI value with the best discriminatory capacity was defined.
Ethical Considerations: the study was approved by an ethics committee (#08065/2023) and informed consent was obtained from all participants. The ethical principles established in the Declaration of Helsinki and Colombian legislation were respected. The study was judged to be of minimal risk and to comply with the principles of nonmaleficence, beneficence, and autonomy. Confidentiality of patient information was ensured and access to study results was limited to authorized personnel.
Competing interests: they have no competing interests.
Results
A total of 221 patients, of which 192 met the inclusion criteria, with respect to gender, it was observed that most patients were women, representing 65.63% of the sample. The mean age of the patients was approximately 61.7 ± 10.73 years. In terms of BMI, most patients had a BMI in the "Normal" and "Overweight" categories, with a low percentage of patients in the "Underweight" and "Obesity" categories (Table 1).
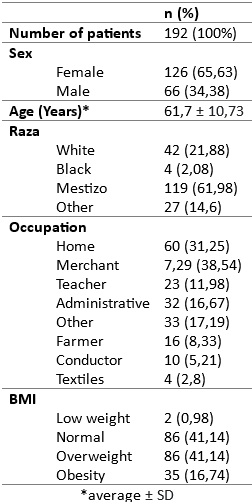
81.89% of the women were in menopause and 21.88% had a family history of OA. It is important to note that none of the patients had previously received a diagnosis of osteoarthritis, had no history of hand trauma, nor did they have a history of hand surgery or tumor injury in the hands. Regarding smoking, a minority of patients were smokers at the time of the study, and 59.90% reported engaging in some physical activity. In addition, it was found that 20.83% of the patients had grasping in the hands, and approximately 51.04% reported experiencing pain.
Similarly, the rheumatology service performed the functional evaluation of the hand using the AUSCAN scale (Australian/Canadian Osteoarthritis Hand Index), highlighting several significant findings in the population evaluated. First of all, it is observed that pain in the hands is a prevalent symptom, affecting more than 80% of patients in general. In addition, there is evidence of marked difficulty in hand function in everyday activities, such as turning faucets, turning handles, buttoning, holding jewelry, and performing tasks that require strength, such as opening jars or carrying heavy pots (Table 2).

Diagnosis of osteoarthritis: it was found that 16.14% of patients had OA, and 83.86% did not. Regarding sex, 80.25% of patients with OA were women, as in the group without OA (62.73%), however, no statistically significant differences were found (p = 0.064).
Joint uptake: measurements of joint-bone uptake and joint-bone uptake index were carried out, and it was observed that, in general, the trapeziometacarpal joint presented the highest uptake, followed by the proximal interphalangeal joint of the third finger.
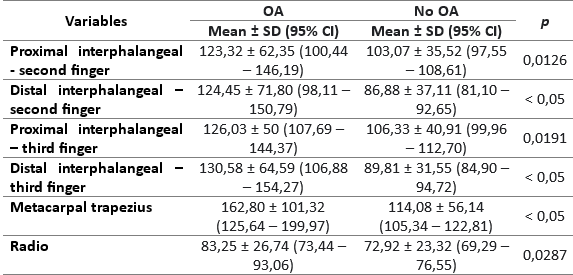
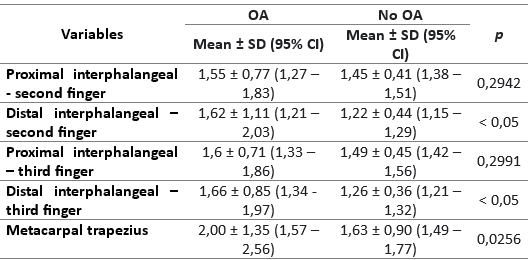
Similarly, we sought to evaluate the level of joint-bone uptake and the uptake index in patients with OA compared to those without OA, revealing that the mean joint-bone uptake in patients with OA was higher; The same was observed in the joint-bone uptake index, as detailed in Tables 3 and 4.
Association uptake and joint index with OA diagnosis: no association was found between uptake and diagnosis of osteoarthritis (OA). However, when considering the uptake rate, significant associations with the diagnosis of OA are revealed. It should be noted that the distal interphalangeal of the second finger shows a significant association with an OR of 2.25 (95% CI 1.27 - 3.98, p = 0.005). Similarly, the distal interphalangeal of the third finger also exhibits a strong association with an OR of 3.71 (95% CI 1.83 - 7.51, p < 0.001) (Table 5).
Sensitivity and specificity: the sensitivity and specificity of joint uptake were evaluated considering multiple slices. It was observed that uptake values between 25 and 50 showed a sensitivity close to 100%; however, at this level, the specificity was less than 20%.
Like joint-bone uptake, when sensitivity reaches 100% with an index of about 0.8, specificity does not exceed 10%. The point at which a balance between sensitivity and specificity can be found is with an approximate uptake index of 1.6, although adequate specificity and sensitivity are not achieved.
Finally, when comparing the uptake and the joint-bone uptake index between patients with OA and those without OA, no significant differences were observed at the time of diagnostic discrimination.
Discussion
As the population ages, the risk of developing osteoarthritis (OA) increases. It has been observed that about 10% of people over the age of 60 and more than 90% of people over the age of 80 suffer from this condition. Despite being a common problem, OA in the hands has received less attention in research compared to OA in the knees and hips. For people between the ages of 71 and 100 years, the prevalence of symptomatic OA is 26% in women and 13% in men. This disease usually results in loss of hand strength and difficulty performing daily manual activities 4)(16.
Our study revealed that people with a diagnosis of OA in the hand were mainly women, with occupations mostly related to housework, followed by those who perform administrative tasks. About 51% of patients with OA were overweight, had never smoked, and most (67.74%) practiced sports. However, when comparing these findings with the group of patients who did not have OA, no statistically significant differences were observed (p < 0.005). Although these results did not reach statistical significance, it is important to note that they are consistent with what has been reported in the international literature.
Previous research has shown that women have a slightly higher risk of developing OA in the hand compared to men, with a relative risk of 1.54 (95% CI 0.83 to 2.86) for incidence and 1.23 (95% CI 1.11 to 1.34) for prevalence. In addition, a possible link between menopause and decreased estrogen levels has been observed, which is associated with an increase in the incidence of OA in women over the age of 40. However, it is important to note that studies on hormone replacement therapy (HRT) do not support a reduction in the risk of OA in these circumstances. Other well-established risk factors include a positive family history, obesity, and joint injuries 17)(18)(19.
When studying osteoarticular conditions in the hands, both degenerative and inflammatory, non-isotopic imaging plays a fundamental role. Conventional radiography stands out as the simplest, most economical, and widely used method, especially in the initial phase of evaluation. On the other hand, magnetic resonance imaging (MRI) is an important technique that allows the evaluation of the first changes in articular cartilage before bone destruction occurs.
However, it is important to note that bone scintigraphy is not currently included in the initial evaluation of osteoarticular diseases. However, this technique demonstrates high sensitivity in detecting changes that precede structural alterations. In addition, it is highly reproducible and has a negative predictive value of more than 90%. Bone scintigraphy can play a crucial role in discerning the source of pain (whether it comes from soft tissues or bone), locating critical areas in patients with complex symptoms, and detecting bone pathologies when other imaging techniques have proven ineffective 20)(21.
In support of this claim, our study revealed that patients diagnosed with osteoarthritis (OA) in the hand had increased joint-bone uptake compared to those who did not have this condition, primarily in the trapeziometacarpal joint. Specifically, in the trapeziusmetacarpal, joint-bone uptake was significantly higher in patients with OA, with a mean of 162.80 ± 101.32 (95% CI: 125.64 - 199.97), in contrast to patients without OA, whose mean was 114.08 ± 56.14 (95% CI: 105.34 - 122.81). This difference was statistically significant (p < 0.05). This pattern of increased joint uptake in patients with OA in the hand was consistently observed in the other joints evaluated, including the proximal and distal interphalangeal joints of the second finger, the proximal and distal interphalangeal joints of the third finger, and in the radius.
In addition, we calculated a joint-bone uptake index using the radius as a reference and confirmed that the uptake with the index is also higher in patients with OA compared to those without. It should be noted that the joint with the highest uptake index was the trapeziometacarpal (2.00 ± 1.35 (1.57 - 2.56) versus 1.63 ± 0.90 (1.49 - 1.77), p 0.002), which is relevant since most of the literature focuses on the distal and proximal interphalangeal joints, both second and third fingers.
However, when the statistical analysis was carried out for the purpose of evaluating the sensitivity and specificity of the measurement of the six joints and their discriminative capacity, it was revealed that, although the sensitivity is high (reaching 100%) when an uptake index of about 0.8 is used in the measurement of the six joints, The specificity is very low, not exceeding 10%. These results conclude that the measurement of the six joints is not an effective tool for the diagnosis of osteoarthritis, since its ability to distinguish between positive and negative cases is limited, and the probability of obtaining false-positive results is high. Therefore, it is suggested to continue to consider other clinical and diagnostic methods in conjunction with this measurement to achieve a more accurate assessment of osteoarthritis.
However, despite the above, an association was identified between the uptake rate and the diagnosis of OA. It is relevant to note that the distal interphalangeal joint of the second finger showed a significant association with an OR of 2.25 (95% CI 1.27 - 3.98, p = 0.005). Similarly, the distal interphalangeal joint of the third finger exhibited a strong association with an OR of 3.71 (95% CI 1.83 - 7.51, p = 0.000), while the trapeziometacarpal showed a marginally significant association with an OR of 1.38 (95% CI 1.01 - 1.89, p = 0.043). This finding is important, because when a patient undergoes a bone scintigraphy and high uptake rates are detected, referral to the rheumatology department for the application of the diagnostic criteria for OA in the hands should be considered; This would contribute to a prompt and timely diagnosis.
Our results, while not supporting bone scintigraphy (GO) as a sensitive and specific diagnostic method for OA in hands, provide relevant association values when performing GO in hands. What we suggest is that if the patient, at the time of GO, has not been referred from the rheumatology service and shows high uptake rates in joints such as the distal interphalangeal of the second or third finger, this patient should be referred to the rheumatology service to undergo additional studies.
Our study provides valuable information to both the medical community and patients in various aspects. First, by identifying associations between bone scintigraphy and osteoarthritis in the hands, it provides an additional tool for the early diagnosis of this condition, potentially leading to more effective treatments and a better quality of life for patients. Likewise, by highlighting the importance of referring patients with high uptake rates to rheumatology, more specialized and accurate medical care is promoted. Finally, this study, being the only one of its kind at the national level, stimulates the generation of more research in this area.
Conclusions
osteoarthritis (OA) is a common condition that significantly affects people's quality of life, especially in the hands. Although its diagnosis presents challenges, our study highlighted the usefulness of bone scintigraphy (GO) as a complementary tool. Although the sensitivity and specificity of GO were limited, significant associations were identified between uptake rates and OA diagnosis. This suggests that GO may be useful in conjunction with other diagnostic methods for a more accurate assessment. In addition, our study underscored the importance of referring patients with high uptake rates to rheumatology for further evaluation. These findings offer valuable insight into improving the diagnosis and care of patients with OA in the hands, promoting more effective treatments and improved quality of life.

