English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
COVID-19 vaccination began worldwide in December 2020. As an event without precedents in the history of public health, in less than 12 months, a vaccine against a previously unknown disease was developed. By mid August 2022, 13.47 billion people had at least one COVID-19 vaccine, out of which 4.90 had a complete scheme, without any doubt, a massive effort to fight the pandemic1.
The World Health Organization (WHO) established that the COVID-19 vaccination strategy's objectives were to minimize mortality and severity, reduce the impact on the health systems, reduce the risk of new variants and reactivate the economy2. By June 2023, 70.3% of the world's population had at least one dose of the vaccine, however, there were large disparities in vaccination rates between high (83.7%) and low-income countries (32.2%)1.
In Colombia, the National COVID-19 Vaccination Plan began in February 2021, and two years after nearly 82.9% of the population had received at least one shot, and 71.3% had full schemes1,3. Even though both Colombia and the world have reached high vaccination coverages, there's still a need to continue efforts to increase trust around vaccination.
Risk communication and health pedagogy strategies based on behavioral sciences are a key part of reaching the community4. According to the WHO, risk communication is the exchange of information, recommendations and opinions between experts, decision-makers, and the public, when facing health threats. Its purpose is that everyone facing risks can take informed decisions to mitigate the uncertainty regarding health risks5. Literature also describes challenges related to the acceptance of vaccines, particularly during the COVID-19 pandemic and its vaccination plan: 1) Doubts, mistrust and skepticism about the vaccine's development and approval processes; 2) Public perception of effectiveness and safety; 3) Antivaccine groups presence4 ; 4) Infodemic, misinformation and barriers to communicate evidence-based content6; 5) Information management and fast variation leading to confusion and delay in vaccine acceptance (e.g. eligibility criteria including time between doses, number or shots, boosters, the combination of vaccines); 6) Public's fatigue and messages of "going back to normal" that make people ignore self-care measures and vaccination4.
Behavioral science's current literature suggests that the reasons not to take the vaccines are modifiable through communication strategies alongside interventions that allow the reduction of people's multiple behavioral barriers when it comes to vaccines. Through communications targeted to increasing knowledge on the effects and vaccine's mechanisms of action, to increasing trust in the communicator (sender), promoting group identity (the behavior of the members of a group), influencing other members' actions7, indispensability of individuals to reach the goal and provide clear information on the contagion risk, adjusting beliefs on consequences and therefore modifying thought processes.
The analysis of critical health events in the past as well as the COVID-19 pandemic (isolation, risk communication, self-care, vaccination), provides valuable lessons such as the importance of fast communication from public health officers, truthful, transparent, easy to understand and up-todate data. Moreover, focusing on mitigating uncertainty and disinformation, as well as increasing the public's trust in their leaders8, experiences during the COVID-19 pandemic have indicated that risk communication, both directly and indirectly, plays a crucial role in promoting and fostering protective behaviors. 8-10
The objective of this topic revision is to present basic concepts, available tools, and recommendations to develop health pedagogy, risk communication and community involvement to promote vaccination strategies, and present an example of communications management during the CO-VID-19 pandemic in Bogotá.
Review's approach
To better understand the process of risk communication and its implications in the COVID-19 vaccination plan, the authors, based on their expertise regarding risk communication and coordination strategies in the Bogotá District, comprised a theoretical framework on which any strategy should be based. These strategies follow a behavioral approach positioned on health pedagogy and both individual and community decision-making. Then we provide some recommendations regarding the nature and form of the messages that should be given in an effective risk communication strategy, and finally, we summarize the results of the vaccination plan in the Bogotá district, including the role of public-private strategies such as the CoVIDA project and their results in vaccination coverage and acceptance.
1. Concepts to develop strategies on health pedagogy, risk communication and community's involvement using behavioral sciences.
1.1. Individual risk perception on health
Individual risk perception is defined as "the probability of hurting health or life quality" given by the frequency in which this can occur and its severity degree, that is, the severity of the consequences. It is individual and built on information available from different sources, as well as personal characteristics such as knowledge in health-related topics, level of schooling, job, religion, trust in authorities and leaders, optimism bias and personal experiences, among others11.
Risk communication in a catastrophic event such as a pandemic becomes crisis communication; therefore, it must have specific characteristics12. It must contribute to minimizing the immediate damage from the crisis since the public is more willing to foster protective conduct to avoid potentially fatal consequences13,14. In the COVID-19 pandemic, it was hard for people to differentiate risk perception from vaccination as one of the ways to end the pandemic; in other words, it was hard to make a difference between a positive action (vaccination) and an adverse event (the pandemic), for the former was seen as a potential risk11,15.
Figure 1 presents a graphic adaptation of risk perception of many situations, ones that may be seen as common in daily life, and others that may pose a greater threat to health. The COVID-19 pandemic and vaccination against this disease are included. The x-axis represents the patient's fear of being infected by SARS-CoV2 (risk), and the y-axis is the level of knowledge about this risk. We placed the COVID-19 pandemic in the upper right quadrant (implying fear because of the uncertainty of the situation), as at the beginning of the pandemic there was very few knowledge regarding the risk attributed to the virus, the pandemic declaration, conflicting reports in media and strategies to avoid contagion all around the world. Although traditional vaccination is known to be an extended practice based on scientific evidence, the vaccine against COVID-19 had no precedents regarding the use of messenger RNA, which is easily mistaken with genetic technology, which also generated high uncertainty and fear. According to multiple studies, the lack of trust in the medical investigation is one factor that negatively impacts vaccination decision-making16,17. However, patients' confidence in their health provider can lead to higher adherence to interventions and treatments17.
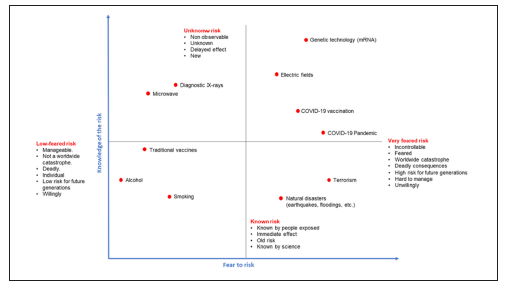
Figure 1 Adapted from Vassie et al 2005, 12 including some common fears that may affect risk communication towards public opinion including events from the COVID-19 pandemic and vaccination.
1.2. Fundamental theoretical models in decisionmaking, motivation, and acceptance of vaccination.
There are two models of behavior change associated with decision-making, motivation, and acceptance of vaccination: 1) COM-B developed by the Centre of Behavioral Changes from the University College-London (UCL) 18, and 2) the Behaviors Model by BJ Fogg19.
1.2.1. COM-B Model of behaviour
The COM-B model encloses more than eighty behaviors change theories and identifies three factors that affect behavior and decision-making, 18 as shown in Figure 2.
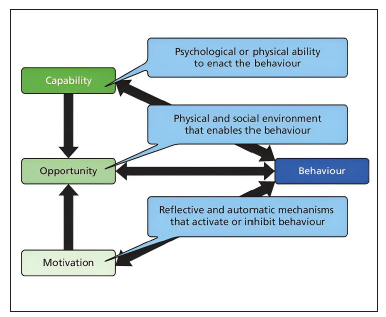
Figure 2 The COM-B Model of the interrelation of dimensions in decisionmaking, adapted from Cataldi et al. 202020
Capability: Knowledge and abilities related to a particular topic.
Opportunity: Environment-related opportunities.
Motivation: Automatic and reflective mechanisms.
The Table 1 includes a detailed explanation of each dimension and a couple of examples of their implication for CO-VID-19 vaccination.
Table 1 Factors and examples of the COM-B Model of the interrelation of dimensions in decision-making20 applied to COVID-19 vaccination.
| Dimension | Factors (Barriers or facilitators) involved in the desired action | Examples on how it becomes a barrier in each dimension |
|---|---|---|
|
Capability: Physical and psychological abilities are required to decide and carry out an action. |
For the policy maker: • Knowledge and understanding on how the virus and vaccines behave; consequences in health of contagion; current data on the prediction of contagion; vaccination data, perception of public's feelings on the virus and vaccination, costs to consider as well as the required logistics for supplying the vaccine. For the public: • Knowledge and understanding of the virus's behavior, how vaccines against COVID-19 and vaccines in general work, differences between vaccine brands, percentages of protection as well as contagion risks. |
For the policy maker: • Misunderstanding vaccines' action mechanisms may lead to providing wrong information to the public on the importance of vaccination (or not communicating it at all) and not taking the necessary restrictive measures to promote vaccination. Not understanding costs and logistics may lead to errors in the planning and execution processes causing a shortage in the supply, excessive costs, and potential loss of the vaccine lots. For the public: • Suppose a young person without risk factors doesn't recognize the importance of vaccination to reduce contagion and consequences on older people or with risk factors; they may not get the vaccine thinking that they don't need it since it only benefits the person who takes them. |
|
Opportunity: Physical characteristics of the individual's environment, social and cultural factors. |
For the policy maker: • Lack of necessary economic resources, providers, time, and infrastructure to buy, store and distribute the vaccines and communication material. • Cultural practices that affect health and vaccination • Restrictive institutional and regulatory framework, that limits decision making and regulation For the public: • Time availability, public transportation, access to vaccines and information about the virus. • Social practices. • Beliefs and cultural practices that influence decision making. |
For the policy maker: • Limited resources to produce communication campaigns may decrease the desired reach to targeted audiences with accurate information on schedules, places, benefits, and risks. For the public: • People with low time available due to work may not get vaccinated as it imposes a burden on their daily basis. |
|
Motivation: Reflective (value judgements, goals, and perceptions) and automatic (feelings, bias) mechanisms that activate or inhibit behavior |
For the policy maker: • Value judgements about the situation and the vaccines. Individual's freedom vs the greater good. Perceptions on what's necessary for the people. Bias on availability, optimism and trust affects the risk perception of the policy maker. For de public: • Value judgements on the importance of vaccines, their personal freedom. • Bias on availability, optimism, and trust, among others. • Feelings on getting the vaccine. |
For the policy maker: • A trust bias may affect the decision-making process and lead to inefficient measures regarding vaccination requirements, thinking that the pandemic will evolve positively. For the public: • Fear or uncertainty regarding the vaccines may prevent them from getting them when the time comes. This may be influenced by a lack of knowledge on how vaccines work or based on negative experiences. |
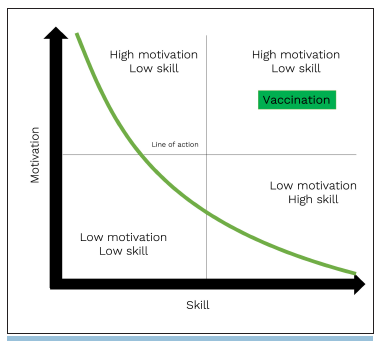
1.2.2. Fogg model of behavior
The Fogg model has been used in studies and campaigns to develop public health messages, mainly to promote contraceptives and other self-care19-21. This model, shown in Figure 3, raises three fundamental elements for the appearance of a behavior: Motivation, skill, and opportunity22. There's a need for the three elements to be present at a high level to have a behavior Figure 3, upper right). Regarding COVID-19 vaccination, motivation is the desire to get the vaccine; availability is the capacity to access the vaccine itself, and skill is the ability to go to vaccination center to get vaccinated. High levels of one factor, but low levels of the other, will limit access.
2. Recommendations for decision-makers on the design and divulgation of messages in health pedagogy and risk communication based on the behavior models
The following recommendations are meant to guide the design of messages related to health pedagogy, risk communication and community involvement to promote COVID-19 vaccination, applicable to other similar public health situations. Explains what, when and who of the communication pieces.
2.1 What to communicate: On the design and content of the message.
According to the "Wheel of behavioral change" methodology from the Behavioral Change Centre, designed by the Faculty of Psychology at University College London (UCL) 23, a decision-maker can use multiple interventions and tools, like suasion, modelling and enablement, to increase the effectiveness of the communication pieces. In turn, these can be used in conjunction with incentives and restructuring the environment to make the vaccine more accessible and attractive.
A decisionmaker must understand the cognitive mechanisms and the public's emotional response and preferences of the people, such that the design of the message is better and has a natural effect on the decision-making process of the targeted audience. It's essential to have a risk communication plan that focuses on the following aspects) 23:
To reduce or mitigate the perceived risk, rumors, and misinformation, and to increase knowledge on safety and effectiveness.
To identify the interested parties in the vaccination process and target the right strategies for them.
To adapt communication to culture and language.
To communicate the associated risk of declining vaccines, such as getting the severe disease, dying, infecting others. It is essential not to scare people excessively since it may be counterproductive.
To advocate for vaccination strategies by listening, involving the community, and creating alliances between public and private sectors to establish joint actions.
When elaborating on the messages, acknowledge that often content tends to be too long and contain too much information. Therefore:
Rely on trust-worthy sources, such as scientists, to access data and write message24.
Identify two or three main messages to share. Avoid long content and be too detailed as it may lose people's attention25.
Adapt the message according to the targeted audience, their schooling, literacy, and cultural background.
Avoid technical words, preferring easy-to-understand language25.
Design messages to inform people willing to get the vaccine and answer their questions. Their behavior changes may inspire others to get the vaccine, too.
Use graphics for people to understand the risk, as it enhances understanding. Show a contrast of risk between certain groups, such as the elderly vs young people, so they know everyone plays a part.
Promote actions rather than passivity.
Show protection strategies against fake news and disinformation.
Assess the particularities of the group to which the message is intended. Even though health literacy remains one the factors related to vaccine hesitancy, other factors such as age, race, country, and type of vaccine interact with each other to produce a decision to take the vaccine26. The COVID-19 pandemic is no exception, and low health literacy has been associated with poorer understanding of symptoms, less ability to identify protective behavior, less access to healthcare during lockdown and higher likelihood of endorsing misinformed beliefs about COVID-19 vaccination27.
Use a multidisciplinary team to assess the in the community's healthcare literacy and points of possible influence, including follow-up strategies for message reception, which are also an essential part of effective risk communication29.
Multiple social media channels can be utilized to monitor and track the evolving landscape of misinformation, enabling timely responses to address them appropriately28.
2.2 When to communicate: On the communication of the message.
There are three transversal factors to be considered when communicating a message, regardless of the persuasion te-chniques25.
2.3 Who will communicate the message.
Various techniques increase comprehension and persuasion, according to available literature7,24,25. Some of them are using trustworthy communicators, social norms, reminders of shared identity, mind maps, information on consequences, feeling of indispensability, reciprocity, empowerment, urgency, and dividing messages according to gender, age, and cultural background.
Those who create the message should be aware of the target's characteristics to adapt the message to them. Who will communicate the message? Why are they adequate? Are they trained? What do they represent for the targeted audience? Will they generate trust or uncertainty?
The communicator/sender should take into consideration the following:
Reinforce favorable social norms to communicate when most people are doing things right.
Explain that the lack of information is not a weakness but a proof of strength and honesty.
Avoid speculation on rumors or data that has not yet been confirmed; neither should they promise results beyond knowledge.
Deliver honest, transparent, and timely information. People reject paternalism or people who make choices for them.
Investigate the audience's language and use it. Avoid the use of humor in times of emergency.
Recognize the audience's fears or doubts, as well as distrust, concerns, anger, and risk perception.
Identify allies and opponents and direct messages to both.
Show positive messages about vaccination, share people's positive experiences with the vaccination process, and include decision-makers, healthcare workers and the community.
Establish trust and empathy with the audience. Uncertainty related to COVID-19, as well as the political and economic context, hurt the public's trust10.
To build the community's trust, we suggest using the COTICE strategy 14 as shown in Table 2. 14
Table 2 COTICE strategy to build the public's trust. Adapted from: Crisis Communication related to vaccine safety: technical guidance. Pan-American Health Organization (2021). 14
| Competence | Demonstrate enough knowledge to handle the crisis. |
| Objectivity | Information and actions shouldn't be affected by conflict of interest. |
| Transparency | Risk communication should be transparent, honest, and open. No facts should be hidden from the public. |
| Inclusivity | Include all relevant opinions. |
| Consistency | All the strategies should be aligned with the purpose and adapted to the context. |
| Empathy | Bidirectional dialogue acknowledges the public's concerns and focuses on collective and individual well-being. |
The emotional factors, social processes, risk communication tools and how messages are communicated should be considered when formulating strategies to promote vaccination. A successful communication strategy should reduce the public's obstacles, affecting their behavior. It should be the first step when designing policies and effective communication strategies. A systematic literature review by Cochrane in 2018 found different methods to increase the Influenza vaccination rates in adults over 60 years of age, including increasing the communities' demand for the vaccine, improvements to access to vaccination and incentives to health services providers29.
Therefore, citizens' governance should be improved in times of emergency. As cooperation of the citizens in terms of risk is encouraged, a better appropriation of knowledge, attitudes, prevention, and mitigation practices is favored. National and international health authorities must improve the risk communication so that messages do not follow a fear narrative but evidence-based information and institutional and people's responses. Similarly, public spaces should be utilized to foster engagement between citizens and health system actors, promoting knowledge sharing, facilitating deliberative dialogues, and providing policy summaries. These efforts are essential for effectively disseminating messages related to prevention, mitigation, and elimination.
3. Lessons learnt in Bogota's experience with the COVID-19 pandemic.
One of the main features of the management of the crisis generated by the COVID-19 pandemic in Bogotá was extensive social research to understand citizens' beliefs, attitudes, and behaviors. The sub-secretariat of citizen's culture and knowledge management of the Bogotá Mayor's Office conducted weekly representative surveys, as well as counts, observations, and interviews to better understand what was happening with citizens' behavior and their cultural motivations. Experiments were also conducted to test the capacity for citizen mobilization based on the messages disseminated in the communication strategy. Research reports on citizen behavior were presented to the District Epidemiological Committee and were used as an input for decision-making and implementation of communication strategies.
3.1. Evidence-based communication strategies in behavioral science.
Regarding vaccination, as a result from the sub-secretariat of citizen's culture investigations, it was possible to observe that people who had not been vaccinated (up to July 2021) has different motivations, depending on their age (citizens under 40 and over 40 years old). Even so, it was possible to organize the citizens into different groups, based on their characteristic motivations, highlighting aspects that were not easy for the health authority to observe. For example, Figures 4 a and b), irrespective of age, the largest groups of people who had not been vaccinated were composed of citizens who did not have enough information and reported difficulties in requesting a vaccination appointment. Additionally, other barriers related to aspects such as the following were observed:
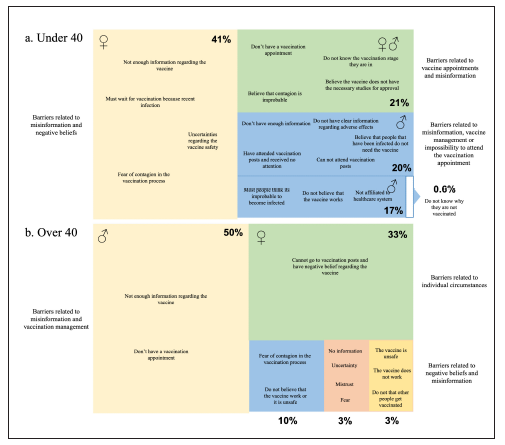
Source: Undersecretariat for Citizen Culture and Knowledge Management
Figure 4 Reasons why people were not vaccinated up to July 2021. a. People under 40; b. people over 40.
People for whom the health care provider companies have not yet scheduled a vaccination appointment.
People who thought they no longer needed the vaccine because they had been previously infected.
People who do not have vaccination centers close to them (difficulty accessing the vaccination centers).
People who wanted to be vaccinated but were afraid of getting infected if they went to a vaccination point.
People who did not know what stage of vaccination they were in.
People who had been to a vaccination point and had not been attended.
People (including migrants) who believed that because they were not affiliated to the health system, they would not have access to the vaccine.
This information allowed official measures to be taken, such as eliminating the need for appointments, massively informing that both the undocumented immigrant population and people without affiliation to health services could be vaccinated and communicating that people could be vaccinated in any nearby centers regardless of the health care provider. Similarly, much more emphasis was placed on clarifying the stages of vaccination and making visible the biosecurity measures implemented in vaccination centers to avoid crowds and ensure adequate ventilation to avoid further contagion.
The media, as key actors in the social construction of reality, were an important part of the risk communication strategy. Several workshops and working groups including news broadcasting teams, editors-in chief and directors of television and digital news media were held, to make the media aware of the strategic value of the information they were presenting to the public and to help them to adequately present the most important messages to overcome the crisis. Both the official pedagogical resources and those issued by the media included real testimonies from citizens celebrating both the quality of care provided at the vaccination centers and their biosecurity measures.
Pedagogical and narrative elements such as the above are essential for the promotion of behavior, given that the social norms approach has shown us that what people think of their community influences their behavior30. For this reason, the communication strategy designed by the Mayor's Office of Bogotá sought to make visible those citizens who cooperated with the vaccination and biosecurity measures, favoring a positive narrative (based on group esteem) of the general response to the pandemic. As we will show below, this was also tested in communication messaging experiments, showing that positive messages motivating the public based on what they value about their community are more effective in risk communication30.
Additionally, in Bogotá, the authorities implemented risk communication strategies based on the evidence and the behavioral sciences to increase the effectiveness of messages, such as:
Short, easy-to-understand messages with concrete actions.
Design attractive, compelling, unforgettable, eye catching advertisements.
Timely delivered communication.
Use of behavioral communication tools already proven to be effective, such as:
Social Norms: Referring to what most people believe and do in the desired direction norms31. The Subse cretary of Civic Culture used the message "Because 8 out of 10 people could be infected and unknowingly spreading the virus, most Bogota's citizens are wearing a face mask. Today 70% trust you to stay at home to save their lives". The sub-secretariat of citizen's culture found that messages using social norms:
Increased perception of Coronavirus infection. o Increased perception that someone in your family may die.
Increased perception that someone in the family may become infected with Coronavirus. o Knowing that it is possible to infect others without knowing it.
Perceiving that you can trust people more.
Mind maps and empowerment: Explains easily how contagion works and reminds people that their actions matter. "8 out of 10 people who contract the virus have no symptoms or mild symptoms. That is, they may have the virus without realizing it. You could be one of them and be unwillingly transmitting the virus. For this reason, it is essential that we all wear a mask. Since the virus is transmitted through saliva when talking or sneezing, by wearing a mask properly, you could be saving the lives of everyone you come across". According to the sub-secretariat of citizen's culture results, shared mind map with precise information makes it easier to generate self-care practices measured by: 31 o Increased perception of Coronavirus infection. o Increased perception that someone in your family may die.
Knowing that you are likely to be infected and not have symptoms.
Increased perception that someone in the family may be infected with Coronavirus. o Knowing that it is possible to be infecting others without knowing it.
Family costs: This strategy explained potential personal and family losses and included a call to action with loved ones in mind. "In Bogota, 7 out of 10 people are infected with Coronavirus, and one person is in serious danger of death. Therefore, when you leave your home, you put yourself and all your loved ones at risk. If you want to ensure your family's health, stay at home." According to the sub-secretariat of citizen's culture results31:
Increased perception that because of the coronavirus crisis, someone in their family may die.
Increased perception of high risk in your place ofresidence.
Unwillingness to risk death to meet my financial needs. o Increased perception that most people in the city are complying with the isolation measure. o Greater trust in people in general.
Other strategies included behavioral tools such as:
Reciprocity: The Behavioral Insights Team (BIT) within Spanish speaking population in the USA and Colombia used the message "Health staff are the first to get the vaccine. To help them fight COVID-19, they need you to get the vaccine when your time comes" and found that the use of reciprocity was the most effective message to increase intention to vaccinate in a controlled experiment where not receiving a message was the control group and 4 types of messages were tested combining behavioral tools such as reciprocity, messenger effect and building trust. (Message taken from the presentation by the BIT to governments and related staff) 32.
The Messenger Effect: To use the public's trust in health personnel and scientist to support call-to-action32.
Indispensability: Use messages such as "You are indispensable to help Colombia reach herd immunity. Get your vaccine."
Urgency: Reducing the feeling that there's plenty of time to get the vaccine, including in the words as now, urgent, today, in the message delivered.
One of the essential learnings from the experiments run in Bogotá was that frightening messages not only did not work but had adverse effects. The following messages had a contrary impact on perceptions and intentions to improve self-care measures. Therefore, using this type of messages was avoided under the hypothesis that they could be generating cognitive dissonance and therefore avoidance of self care measures.
Examples of the messages used as part of the risk communication strategy using the recommendations listed above are as follows:
"Did you know that Suba is the locality with the highest number of infections and the second highest number of deaths in Bogota? Living in an area with a high risk of infection increases the probability of illness and death for you and your family members. Therefore, remember that if you live in this area, you and your family are at greater risk than other Bogota residents. If you want to ensure the health of your family, stay at home."
"Did you know that Kennedy is the locality with the highest number of deaths due to Coronavirus in Bogota? Living in an area with a high risk of infection increases the probability of illness and death for you and your family members. So, remember that if you live in this area, you and your family are at greater risk than other Bogota residents. If you want to ensure the health of your family, stay at home."
3.2. Multi-sectoral partnership (the COVIDA project).
Alliances between universities, the private and public sector were essential to increase the care capacity and available vaccination points. As mentioned in the last section, one of obstacles detected using social research was the lack of vaccination centers available to citizens (mainly in low-income population). At this point, projects such as the CoVIDA strategy "la vacuna es de todos" were essential. This strategy was based on the need to support the progress of the Vaccination Plan against COVID-19 and favor access to the vaccination centers to people from challenged socioeconomic backgrounds and high SARS-CoV-2 transmission rates. The project focused on mitigating the morbidity and mortality risk from COVID-19 in communities with low vaccine coverage and limited access to the vaccines due to geographic and economic hardships, lack of formal work and immigration. The Universidad de los Andes, the Bogotá District Health Secretariat, the National University of Colombia, the National Association of Industrialists (ANDI) and the University Hospital of the Santa Fe de Bogotá Foundation participated in this alliance.
This vaccination initiative had three main pillars that guaranteed its success: a) Epidemiological and public health aspects to choosing vaccine locations by looking for neighborhoods with low vaccination rates; b) Timely and straightforward communication strategies; and c) An operations and logistics strategy to monitor the project; disseminate progress in the media and determine actions that would improve the operational efficiency of the vaccination centers to provide better coverage.
The risk communication strategy was key to solving questions, bringing down myths and fake news about vaccination, and showing the importance of actively including communities in successful public health interventions. The latter was vital in ensuring CoVIDA's success since it was the community, through social leaders, who led workshops where health staff would answer questions and explain the risks associated with SARS-CoV-2 and the importance of massive vaccination. The strategy was based on fighting the targeted audience's misinformation and educating them on the importance of making the vaccine available for everyone to mitigate the pandemic. Therefore, a series of actions were developed to reach the community with a clear, honest, timely message. Some of these actions were: loudspeakers, flyers, word of mouth, door to door visits, community workshops, community media management, motorcycle-billboard tours and digital dissemination through social media, text messages and publications on social networks.
This strategy focused on increasing access to vaccination in groups with high risk of contagion using strategic alliances between the private and public sector. For example, the CO-VIDA project made agreements with the Secretariat of Culture, Recreation and Sport of Bogotá to apply vaccinations in cultural teams, adapting these spaces for the vaccination of the population that did not have vaccination centers nearby. The model implemented by CoVIDA made possible the massive vaccination for a heterogeneous population of over 100,000 people by increasing health pedagogy, implementing risk communication strategies, and reducing the access barriers in terms of logistics and time of wait.
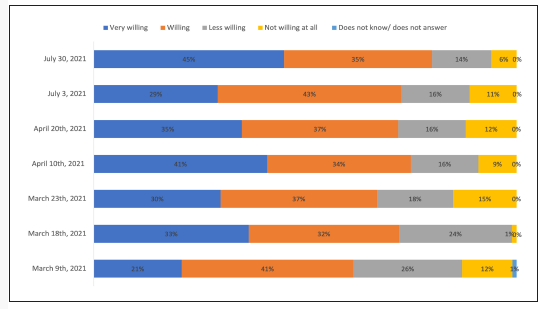
The result of the implementation of this strategy is proved by illustrating the evolution in the obstacles reported to mass vaccination, that went beyond fighting a negative attitude towards the vaccine. As the Figure 5 shows, the proportion of people who were "not at all willing to be vaccinated" was minimal, representing only 6% of the population in July 2021. In conclusion, the risk communication's implicit processes and the modifications of behavior in terms of public health are particularly complex. Multiple factors play a role, particularly in public health emergencies where there is no concrete data on the impact of it, management plans or specific follow-up, which makes it harder to create effective messages. However, as scientific evidence increases on a particular subject, decision-makers, experts, and health staff, among others, should prioritize the development and adaptation of messages according to the public, understanding it is an ongoing process that should be adapted to the most recent scientific evidence. It is key to ensure that risk communication is timely, clear, trust-worthy, targeted to all audiences, and uptodate according to the growing evidence, to properly change behaviors and ensure the well-being of the communities. According to Bogota's experience, social research is a key tool to understand the motivations and behavior of citizens as well as specific change tools strategies, such as using social norms, potential family costs, mind maps, and empowerment that can increase the effectiveness of risk communication. The successful results from the communication strategies from the COVID-19 pandemic and the increased coverage in the SARS-CoV-2 vaccination program can be used as a guideline to better tailor future risk communication strategies as needed.